I AM FINAL YEAR OPHTHALMOLOGY RESIDENT, I WANT TO STUDY OPHTHALMOLOGY FROM THE VERY BASICS TO ADVANCED LEVEL, EVERY TOPIC, FROM WHICH TOPIC SHALL I START MY STUDYING? I HAVE MY EXAMS IN 9 MONTHS FROM NOW. HELP ME MAKE ADVANCED NOTE FROM VERY BASICS TO ADVANCED LEVEL IN EACH AND EVERY TOPIC WITH ILLUSTRATED DIAGRAMS AND FLOWCHARTS WHEREVER POSSIBLE
ophthalmology residency exam preparation systematic study plan topics 2025
Ophthalmology Final Year Residency - Complete Study Plan (9 Months to Exam)
Your Textbook Arsenal (In the Library)
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed - the gold standard comprehensive reference
- The Wills Eye Manual - rapid clinical/ER reference and exam rapid review
Strategic Framework: How to Study
- Foundation - Anatomy, physiology, optics (first 6 weeks, non-negotiable)
- Core Clinical - Disease mechanisms, diagnosis, management (months 2-6)
- Advanced & High-Yield - Surgical techniques, complications, current evidence (months 7-9)
- Definition + epidemiology
- Pathophysiology (with flowchart)
- Clinical features (with diagram/illustration)
- Investigations + findings
- Management (medical → laser → surgical, with decision flowchart)
- Complications
- High-yield exam points (last bullet in red/bold)
PHASE 1: FOUNDATIONS (Month 1 - Weeks 1-4)
Topic 1: Ocular Anatomy (Week 1-2)
Globe layers
├── Fibrous coat: Cornea → Limbus → Sclera
├── Uveal tract: Iris → Ciliary body → Choroid
└── Retina: RPE → 10 layers → fovea/macula
Anterior Segment
├── Cornea (5 layers - Bowman's, Descemet's etc.)
├── Anterior chamber anatomy + trabecular meshwork
├── Iris & pupil pathways
└── Crystalline lens - zones, sutures, capsule
Posterior Segment
├── Vitreous structure
├── Retinal layers (detailed)
├── Macular anatomy
└── Optic nerve head - lamina cribrosa
Adnexa
├── Eyelids (tarsal plates, levator, Müller's)
├── Lacrimal system (secretory + excretory)
├── Conjunctiva
├── Extraocular muscles (origins, insertions, actions)
└── Orbital anatomy (walls, foramina, contents)
Topic 2: Ocular Physiology (Week 2)
- Aqueous humor dynamics (production, flow, drainage) → draw flowchart
- Accommodation mechanism (Helmholtz theory)
- Pupillary light reflex pathway (direct and consensual) → draw arc
- Dark and light adaptation (rods vs cones)
- Tear film (3-layer structure, TFBUT)
- Colour vision (Young-Helmholtz trichromatic theory vs Hering opponent)
- Retinal signal transduction (phototransduction cascade)
Topic 3: Optics and Refraction (Week 3-4) ← VERY HIGH YIELD
GEOMETRIC OPTICS
├── Reflection, refraction, Snell's law
├── Lenses: convex/concave, focal length, power
├── Prisms: deviation, Prentice's rule
└── Mirrors: plane, concave, convex
PHYSIOLOGICAL OPTICS
├── Reduced eye model
├── Nodal point, principal planes
├── Visual angle and acuity
└── Depth of focus vs depth of field
REFRACTIVE ERRORS
├── Myopia (axial vs refractive, types)
├── Hypermetropia (latent/manifest/absolute/total/facultative)
├── Astigmatism (regular/irregular, with/against the rule)
├── Presbyopia
└── Anisometropia, aniseikonia
CLINICAL OPTICS
├── Keratometry principles
├── Retinoscopy (reflex types, neutralization)
├── Subjective refraction
├── Prescribing glasses and contact lenses
├── IOL power calculation (SRK, SRK-II, SRK/T, Haigis, Holladay, Barrett)
└── Low vision aids
INSTRUMENTS (draw each one)
├── Direct ophthalmoscope
├── Indirect ophthalmoscope
├── Slit lamp
├── Applanation tonometer
├── Keratometer / Topographer
└── Autorefractometer
PHASE 2: CORE CLINICAL TOPICS (Months 2-6)
MONTH 2: Anterior Segment I
- Corneal anatomy (5 layers - Epithelium, Bowman's, Stroma, Descemet's, Endothelium)
- Keratoconus (forme fruste → advanced) - Vogt's striae, Munson's sign, Fleischer ring
- Pellucid marginal degeneration vs Keratoglobus
- Corneal dystrophies (Fuchs', Map-Dot-Fingerprint, Macular, Granular, Lattice)
- Keratitis: bacterial, viral (HSV - dendrite → geographic), Acanthamoeba, fungal
- Corneal ulcer management algorithm:
Corneal ulcer
├── Scraping → smear + culture
├── Bacterial → fluoroquinolone drops (moxifloxacin/ciprofloxacin)
├── Fungal → natamycin / voriconazole
├── Viral (HSV) → acyclovir/ganciclovir + NO steroids
└── Acanthamoeba → PHMB + propamidine (Brolene)
- Conjunctivitis: bacterial, viral, allergic, neonatal (ophthalmia neonatorum)
- Trachoma (WHO grading: TF, TI, TS, TT, CO) - VERY high yield
- Pterygium vs Pinguecula
- Subconjunctival hemorrhage, chemosis
- Ocular cicatricial pemphigoid, Stevens-Johnson syndrome
- Entropion (involutional, cicatricial, congenital) + surgical corrections
- Ectropion types + Medial canthoplasty
- Ptosis classification (neurogenic, myogenic, aponeurotic, mechanical, traumatic)
- Levator function measurement
- Hering's law and its clinical implications
- Surgical options: Fasanella-Servat, levator resection, frontalis sling
- Blepharitis (anterior/posterior)
- Chalazion vs Hordeolum
- Eyelid tumors: BCC (most common), SCC, sebaceous cell carcinoma (masquerade syndrome!)
- Dacryocystitis (acute vs chronic)
- Nasolacrimal duct obstruction (CNLDO in children - timing of probing)
- DCR (external vs endoscopic) - steps and indications
- Dry eye disease: DEWS II classification, Schirmer's test, TFBUT, management ladder
- Sjogren's syndrome
MONTH 3: Anterior Segment II
CATARACT
├── Classification (nuclear, cortical, PSC, anterior)
├── Age-related pathogenesis
├── Systemic associations (DM, steroids, myotonic dystrophy, Wilson's)
├── Grading: LOCS III
├── Preoperative workup (biometry, keratometry, endothelial count)
├── IOL calculation formulas (3rd vs 4th vs 5th generation)
├── PHACO technique (CCC, hydrodissection, phacoemulsification modes)
├── Complications:
│ ├── Intraoperative: PC rupture, dropped nucleus, suprachoroidal hemorrhage
│ └── Postoperative: PCO, endophthalmitis, TASS, CME, retinal detachment
└── Pediatric cataract (timing of surgery, amblyopia prevention)
- IOP physiology, optic nerve damage mechanisms
- POAG: optic disc changes (C/D ratio, ISNT rule, NRR changes, disc hemorrhage)
- Visual field defects (arcuate scotoma, nasal step, paracentral)
- OCT-RNFL interpretation
- Gonioscopy: Shaffer grading, van Herick
- Medical therapy ladder:
IOP lowering drugs:
1st line → Prostaglandin analogues (latanoprost, travoprost)
2nd line → Beta-blockers (timolol) - CI: asthma, COPD
3rd line → CAIs (dorzolamide, brinzolamide / oral acetazolamide)
4th line → Alpha-2 agonists (brimonidine)
Add-on → Pilocarpine (miotic)
- SLT (selective laser trabeculoplasty) indications
- Trabeculectomy: steps, antimetabolites (MMC, 5-FU), complications (blebitis, hypotony)
- Tube shunts (Ahmed, Baerveldt) indications
- PACG: anatomical predisposition, acute angle closure crisis management
- Peripheral iridotomy (PI) - indications, technique
- Secondary glaucomas: neovascular, pseudoexfoliation, pigment dispersion, steroid-induced, uveitic
- Congenital glaucoma: buphthalmos, Haab's striae, goniotomy vs trabeculotomy
- Normal tension glaucoma
MONTH 4: Uvea and Retina I
- Anatomical classification (anterior/intermediate/posterior/panuveitis)
- SUN (Standardization of Uveitis Nomenclature) grading
- Key syndromes:
- HLA-B27 associated (AS, Reiter's, IBD, psoriasis)
- Fuchs uveitis syndrome
- VKH (Vogt-Koyanagi-Harada)
- Sympathetic ophthalmia
- Sarcoidosis
- Toxoplasmosis (headlight in fog) - MOST COMMON cause of posterior uveitis
- Toxocariasis
- CMV retinitis (in immunocompromised)
- Management: steroids (topical → periocular → systemic), steroid-sparing agents
DR Classification (ETDRS/International):
Non-Proliferative DR
├── Mild: microaneurysms only
├── Moderate: + hemorrhages/exudates/CWS
└── Severe: 4-2-1 rule (4 quadrants hemorrhage / 2 quadrants IRMA / 1 quadrant NVD)
Proliferative DR
├── NVD/NVE
├── High-risk PDR (NVD >1/3 DD with vitreous hemorrhage)
└── Advanced PDR: tractional RD, vitreous hemorrhage
Diabetic Macular Edema (DME):
├── Center-involving vs non-center-involving
└── Treatment: anti-VEGF (1st line) → laser → vitrectomy
- Screening protocols
- FFA interpretation in DR
- OCT findings in DME
- Anti-VEGF agents: ranibizumab, bevacizumab, aflibercept, faricimab
- Dry AMD: drusen (hard/soft), geographic atrophy
- Wet AMD: CNV (classic/occult), PED, RAP, PCV
- OCT findings in AMD
- Treatment: anti-VEGF, PDT, AREDS supplements
- Stargardt disease, Best disease (vitelliform)
- CRVO (ischemic vs non-ischemic) + BRVO
- CRAO + BRAO - management within 4.5 hours (thrombolysis)
- Hypertensive retinopathy (Keith-Wagener-Barker grading)
- Coats disease
- Eales disease
- FFA interpretation (phases: arterial, A-V, venous, late)
MONTH 5: Retina II + Vitreous
RD types:
├── Rhegmatogenous (break-induced) - most common
├── Tractional (fibrovascular traction - DR, sickle cell)
└── Exudative/Serous (VKH, posterior scleritis, tumors)
Symptoms: flashes → floaters → curtain/shadow → loss of VA
Breaks:
├── Horseshoe/flap tears (vitreoretinal traction) - HIGH RISK
├── Round/atrophic holes (lattice degeneration) - lower risk
└── Dialysis (trauma, young patients)
Management:
├── Laser/Cryo prophylaxis (breaks without detachment)
├── Pneumatic retinopexy (selected cases)
├── Scleral buckling (young, no PVR, peripheral break)
└── PPV (vitrectomy - posterior breaks, PVR, complex cases)
- Lattice degeneration (vitreoretinal tufts, snail track, white-without-pressure)
- PVR classification (A/B/C/D)
- Silicone oil vs gas tamponade (C3F8, SF6)
- PVD (posterior vitreous detachment) - Weiss ring
- Vitreous hemorrhage causes and management
- Retinitis pigmentosa (bone-spicule pigmentation, tunnel vision, ERG findings)
- Stargardt, Best vitelliform, Cone dystrophy
- Usher syndrome, Bardet-Biedl syndrome
- Choroideremia
- Retinoblastoma: genetics (RB1, two-hit hypothesis), leukocoria, Reese-Ellsworth + IIRC classification
- Retinoblastoma treatment algorithm (enucleation, chemotherapy, focal treatments)
- Choroidal melanoma: COMS trial, brachytherapy vs enucleation
- Choroidal hemangioma, osteoma, metastases
- Iris melanoma
MONTH 6: Neuro-Ophthalmology + Strabismus
OPTIC NERVE DISORDERS
├── Optic neuritis (demyelinating - MS, NMO spectrum)
│ └── ONTT results - IV steroids speed recovery but don't change final VA
├── AION: arteritic (GCA - ESR/CRP, temporal artery biopsy, high-dose steroids)
│ vs non-arteritic (altitudinal field defect, disc at risk)
├── Papilledema (bilateral, causes of raised ICP)
├── Pseudopapilledema (drusen)
└── Glaucomatous cupping vs non-glaucomatous
PUPIL DISORDERS
├── RAPD (afferent defect) - optic nerve/retina
├── Horner syndrome: ptosis + miosis + anhidrosis + enophthalmos
│ └── Pharmacological testing (cocaine, apraclonidine, hydroxyamphetamine)
├── 3rd nerve palsy (surgical = complete + PSVM involvement → berry aneurysm)
└── Argyll Robertson pupil (syphilis) vs Holmes-Adie
DIPLOPIA WORKUP
├── 3rd nerve palsy (EOM + ptosis ± pupil)
├── 4th nerve palsy (vertical diplopia, head tilt)
├── 6th nerve palsy (esotropia at distance)
└── INO (MLF lesion - MS commonest)
VISUAL PATHWAY LESIONS → VF DEFECTS (mandatory memorization diagram)
Optic nerve → monocular loss
Chiasm → bitemporal hemianopia
Optic tract → contralateral homonymous hemianopia
LGN → wedge-shaped
Optic radiation → homonymous quadrantanopia
└── Parietal lobe → inferior quadrant (PIE - Parietal Inferior)
└── Temporal lobe → superior quadrant (TIPS - Temporal Superior)
Occipital cortex → macular-sparing homonymous hemianopia
- Binocular vision (stereopsis, fusion, ARC)
- Esotropia: infantile, accommodative (AC/A ratio), non-accommodative
- Exotropia: intermittent, constant
- Brown syndrome, Duane syndrome (types I/II/III)
- Ocular torticollis
- Prism diopter and Hirschberg test
- Surgical planning (resection/recession amounts)
- Amblyopia: types, critical period, treatment (patching, atropine penalization)
PHASE 3: ADVANCED AND SPECIALTY TOPICS (Months 7-8)
Month 7: Surgical Ophthalmology
- Femtosecond laser-assisted cataract surgery (FLACS)
- Premium IOLs: multifocal, extended depth of focus (EDOF), toric
- LASIK: mechanism, flap creation, excimer laser, enhancements, LASIK ectasia
- PRK vs LASIK vs SMILE (indications and differences)
- Corneal cross-linking (CXL) for keratoconus
- DALK vs PK vs DSAEK vs DMEK (indications, graft survival)
- Pars plana vitrectomy: ports, instruments, principles
- Membrane peeling (ILM, ERM)
- Macular hole surgery (classification, ILM peel, gas tamponade)
- Complex RD with PVR
- Diabetic vitrectomy (4 indications)
- Endophthalmitis management (EVS trial results - vitrectomy if LP only)
- Trabeculectomy with antimetabolites (detailed steps)
- Non-penetrating surgery (viscocanalostomy, NPDS)
- Tube shunts (Ahmed vs Baerveldt - TVT trial)
- MIGS (minimally invasive glaucoma surgery): iStent, Hydrus, Kahook blade, goniotomy
- YAG laser iridotomy, SLT, ALT (argon laser trabeculoplasty)
- Cycloablation (TSCPC)
Month 8: Subspecialty Topics
- Thyroid Eye Disease (TED/Graves' orbitopathy):
- NOSPECS/CAS scoring
- Orbital decompression indications
- Steroids, radiotherapy, teprotumumab
- Orbital cellulitis (preseptal vs postseptal) - CT scan findings, IV antibiotics
- Orbital tumors: capillary hemangioma, lymphangioma, dermoid, lacrimal gland tumors
- Orbital fractures: blow-out (floor/medial wall), trap-door in children
- Enucleation vs evisceration vs exenteration (indications)
- DCR surgical steps
- RGP vs soft lenses: fitting, complications (giant papillary conjunctivitis, neovascularization, CLARE)
- Scleral lenses (keratoconus, OSD)
- Orthokeratology
ANTI-GLAUCOMA DRUGS
Prostaglandins: ↑ uveoscleral outflow (SE: iris pigmentation, hypertrichosis)
Beta-blockers: ↓ aqueous production (CI: asthma, heart block)
CAIs: ↓ aqueous production (SE: bitter taste, renal stones - topical vs oral)
Alpha-2 agonists: ↓ production + ↑ uveoscleral outflow (SE: allergy, CNS depression in children)
Miotics (pilocarpine): ↑ trabecular outflow (SE: brow ache, myopia, retinal breaks)
Rho-kinase inhibitors (netarsudil): ↑ trabecular outflow
MYDRIATICS/CYCLOPLEGICS
Tropicamide (0.5/1%) - short acting (4-6h)
Cyclopentolate (1%) - refraction in children
Atropine (1%) - longest (14 days) - maximum cycloplegia
ANTI-VEGF
Bevacizumab (Avastin) - off-label
Ranibizumab (Lucentis) - licensed for wet AMD, DR, CRVO
Aflibercept (Eylea) - longer durability
Faricimab (Vabysmo) - bispecific (anti-VEGF + anti-Ang2)
Brolucizumab (Beovu) - longest interval (12w) but retinal vasculitis risk
ANTIBIOTICS (topical)
Fluoroquinolones (moxifloxacin, ciprofloxacin) - bacterial keratitis
Aminoglycosides (tobramycin, gentamicin) - gram-negative
Chloramphenicol - broad spectrum (aplastic anemia - rare)
STEROIDS
Dexamethasone > prednisolone > fluorometholone (penetration)
Loteprednol - low risk of IOP rise (anterior segment)
Triamcinolone - periocular/intravitreal
Ozurdex (dexamethasone implant) - uveitis, BRVO/CRVO, DME
PHASE 4: REVISION + EXAM PREP (Month 9)
Week 27-28: Rapid Review + Mock Cases
- Revise Wills Eye Manual (covers emergency presentations perfectly)
- Practice clinical cases (present like a registrar: history → examination → diagnosis → management)
- Revise visual field patterns (draw them all from memory)
- Drug doses and contraindications
Week 29-30: High-Yield Final Pass
- Genetics in ophthalmology (AD/AR/X-linked conditions)
- Systemic diseases with ocular manifestations (DM, HTN, thyroid, sarcoid, TB, syphilis, HIV)
- Ocular manifestations of rheumatological diseases
- Emergency ophthalmology (acute angle closure, CRAO, endophthalmitis, open globe, chemical injury)
Week 31-36: Practice and Self-Assessment
- Minimum 100 MCQs/week
- Clinical case discussions
- Surgical video review (YouTube: ophthalmology channels - Cataract & Refractive Surgery, WillsEye)
Weekly Study Template (Per Topic)
Day 1-2: Read Kanski's chapter → make basic notes
Day 3: Draw all diagrams from memory → add flowcharts
Day 4: Clinical correlations → Wills Eye Manual cross-check
Day 5: MCQ practice (20-30 questions on that topic)
Day 6: Revise weak areas → update notes
Day 7: Rest + light review of week's material
Priority Ranking for Exam (Highest to Lowest)
| Rank | Topic | Why |
|---|---|---|
| 1 | Glaucoma | Most complex, most questions |
| 2 | Retina (DR, AMD, RD) | Surgical + medical both tested |
| 3 | Optics & Refraction | Pure theory - full marks possible |
| 4 | Neuro-ophthalmology | Conceptual, high discriminator |
| 5 | Strabismus | High yield, manageable volume |
| 6 | Cataract Surgery | Surgical steps + complications |
| 7 | Cornea | Keratitis, dystrophies, transplant |
| 8 | Uveitis | Pattern recognition |
| 9 | Oculoplastics | Thyroid eye disease + orbital |
| 10 | Pharmacology | Runs across all topics |
Resources to Supplement Notes
| Resource | Use |
|---|---|
| Kanski's Clinical Ophthalmology 10e | Primary textbook (in your library) |
| Wills Eye Manual | Rapid review and emergencies (in your library) |
| Iowa EyeRounds | Clinical images, case-based learning |
| AAO One Network | Preferred Practice Patterns (guidelines) |
| Ophthalmology Review | Board exam style questions |
| BCSC (Basic & Clinical Science Course) | 13-volume series if you need deeper reading |
One Important Note
THIS WAS ALSO SUGGESTED BY YOU. WHICH ONE TO DO?
Both Plans Are From Me - Here Is the Difference
Side-by-Side Comparison
| Feature | PDF Plan | Plan I Just Gave |
|---|---|---|
| Phases | 4 phases | 4 phases |
| Foundation duration | 2 months | 1 month |
| Pharmacology placement | Month 2 (dedicated week) | Month 8 (combined with contact lens) |
| Pathology/Embryology | Included in Month 2 | Not explicit |
| Glaucoma depth | Month 5 (full block) | Month 3 (2 weeks) |
| Subspecialty depth phase | Months 6-7 | Month 7 |
| Landmark clinical trials | Explicitly listed (Month 6) | Mentioned but not listed |
| Book recommendations | Full list with Indian exam books | Kanski + Wills only |
| Daily schedule | Explicit (morning/afternoon/evening) | Weekly template |
| Exam tips/star ratings | Explicit ★★★ system | Priority ranking table |
My Honest Recommendation: Use the PDF Plan as your backbone, supplement with the notes I just gave
- It includes Embryology - frequently tested in theory papers (optic cup, hyaloid artery, fetal fissure)
- It dedicates a full week to Pathology - granulomatous vs non-granulomatous inflammation, tumor types, genetics
- Pharmacology is in Month 2 - this is the right time, so it supports all clinical topics in Months 3-5 (you need to know drug mechanisms before studying disease management)
- Landmark clinical trials are explicitly called out - ONTT, ETDRS, Protocol T, EVS, MARINA, ANCHOR, TVT - these are directly asked in exams
- It includes Indian exam-specific books (Parson's, Ruchi Rai MCQs) - if you are in India, these are essential
- The ★★★ star rating system tells you exactly where to spend the most time
- The daily schedule (morning theory / afternoon clinical / evening MCQs / night summary) is practical and proven
- More detailed flowcharts for each disease (glaucoma drugs, corneal ulcer algorithm, DR classification tree)
- More surgical detail (FLACS, MIGS, PPV steps)
- Anti-VEGF drug comparison table (faricimab, brolucizumab)
What To Actually Do Tomorrow
BACKBONE: PDF plan (phases, timing, topic sequence)
+
DETAIL: Use my notes above for disease-specific flowcharts
and management algorithms within each topic
+
READING: Kanski's (primary) + Parson's (Indian exam depth)
+
MCQs: Ruchi Rai / Amit Khosla (Phase 4)
Start with Month 1 Week 1 (Eyeball Anatomy) - which layer first? ADVANCED NOTE FROM BASICS TO ADVANCED LEVEL, EVERYTHING YOU NEED TO UNDERSTAND AND ILLUSTRATED DIAGRAMS AND FLOWCHART WHEREVER POSSIBLE
MONTH 1 - WEEK 1: EYEBALL ANATOMY
Advanced Study Notes - Basics to Advanced Level
OVERVIEW: THE EYEBALL AT A GLANCE
╔══════════════════════════════════════════════════════╗
║ THE EYEBALL - 3 CONCENTRIC COATS ║
╠══════════════════════════════════════════════════════╣
║ OUTER (Fibrous Coat) ║
║ ├── Cornea (anterior 1/6) - transparent ║
║ └── Sclera (posterior 5/6) - opaque, white ║
╠══════════════════════════════════════════════════════╣
║ MIDDLE (Uveal Tract / Vascular Coat) ║
║ ├── Iris (anterior) ║
║ ├── Ciliary body (middle) ║
║ └── Choroid (posterior) ║
╠══════════════════════════════════════════════════════╣
║ INNER (Neural Coat) ║
║ └── Retina (10 layers) ║
╚══════════════════════════════════════════════════════╝
CONTENTS OF THE EYE:
Anterior chamber → Aqueous humor
Posterior chamber → Aqueous humor
Lens (between chambers and vitreous)
Vitreous cavity → Vitreous humor (fills 80% of eye volume)
- Anteroposterior diameter: 24 mm (normal adult)
- Horizontal diameter: 23.5 mm
- Vertical diameter: 23 mm
- Volume: ~6.5 mL
- Weight: ~7.5 g
- Axial length > 26 mm → high myopia
COAT 1: THE FIBROUS (OUTER) COAT
A. THE CORNEA
Basic Facts
| Feature | Detail |
|---|---|
| Makes up | Anterior 1/6 of eyeball |
| Refractive power | ~43 D (total eye ~60 D, so cornea = 2/3 of all refractive power) |
| Central thickness | 0.5 mm (500 µm) |
| Peripheral thickness | ~1 mm |
| Horizontal diameter | 11.7 mm |
| Vertical diameter | 10.6 mm (why cornea appears oval when seen face-on) |
| Blood supply | AVASCULAR - gets O2 from tears (anterior) + aqueous (posterior) |
| Nerve supply | Ophthalmic division of CN V (V1) → nasociliary branch → long ciliary nerves → sub-epithelial plexus |
| Lymphatics | NONE - this is the basis of immune privilege |
Why is the cornea transparent? (High-yield viva question)
CORNEAL TRANSPARENCY - depends on 4 factors:
1. AVASCULARITY
└── No blood vessels = no haemoglobin/red cells to scatter light
2. LATTICE ARRANGEMENT OF COLLAGEN (Maurice's lattice theory)
└── Collagen fibrils in stroma are:
- Uniform diameter (~25 nm)
- Uniformly spaced (~60 nm apart)
- Arranged in parallel lamellae
- Spacing < wavelength of light → destructive interference
of scattered light → net transparency
└── Disruption (oedema, scarring) → irregular spacing → opacity
3. RELATIVE DEHYDRATION (Deturgescence)
└── Stroma is hydrophilic (keratan sulphate proteoglycans attract water)
└── Actively maintained by endothelial PUMP (Na/K ATPase)
└── Tight junctions of epithelium = barrier (no tear entry)
└── If endothelial cell density falls below ~500 cells/mm² → oedema → opacity
4. NO NUCLEI / KERATOCYTES ARE FLATTENED
└── Keratocytes are quiescent, flattened - minimal light scattering
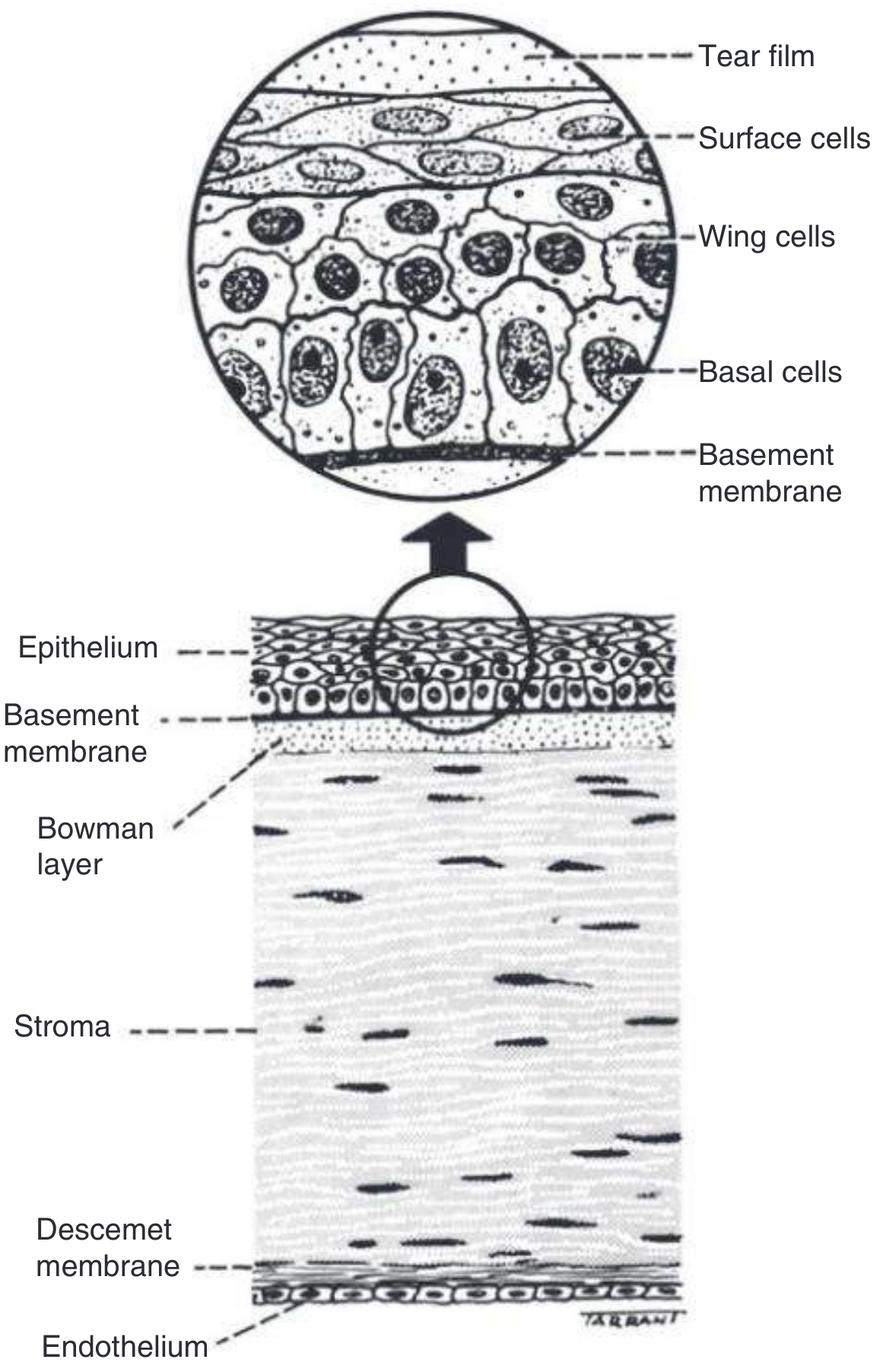
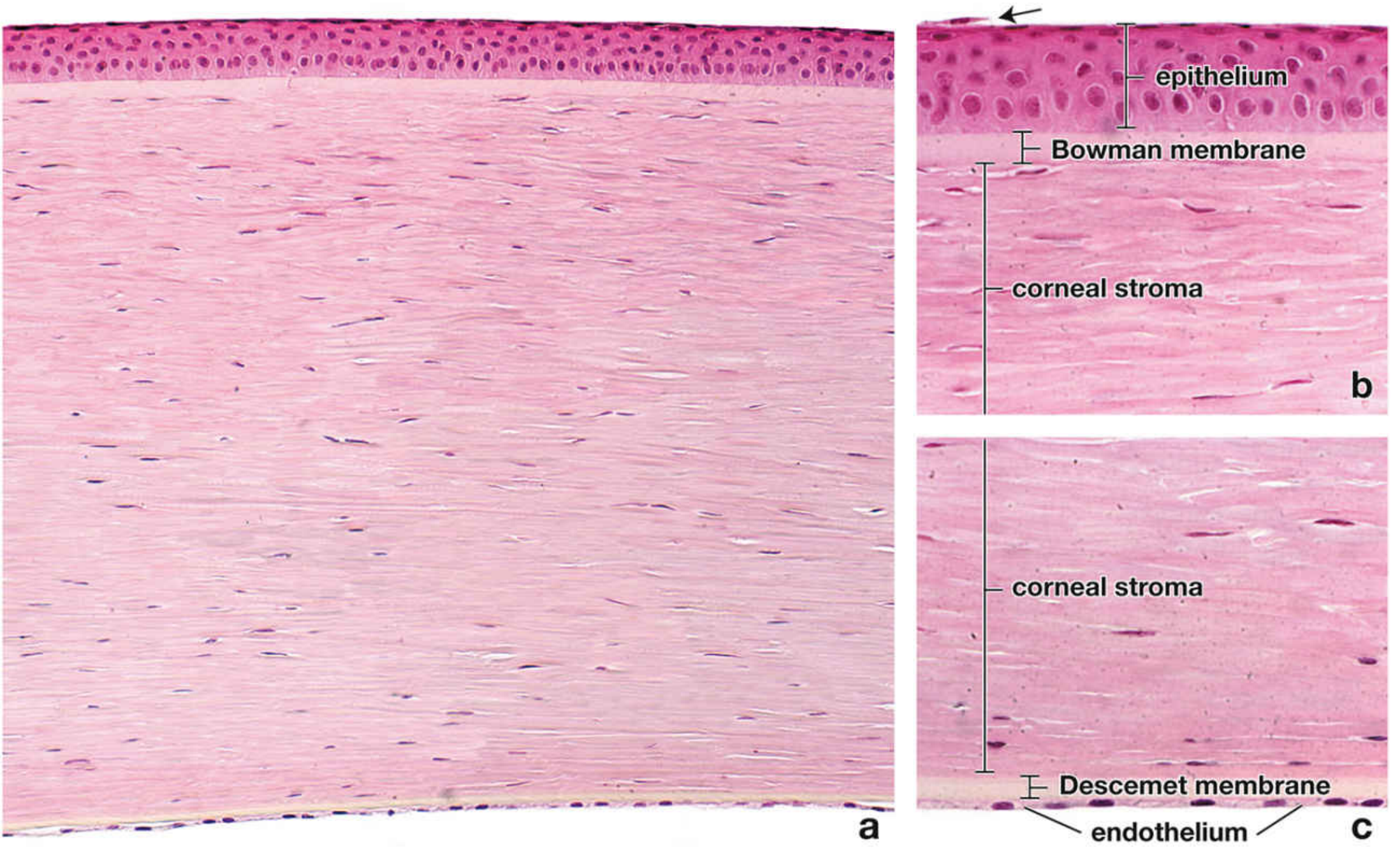
THE 5 LAYERS OF THE CORNEA (+ the proposed 6th)
ANTERIOR (outside world)
│
▼
┌─────────────────────────────────────────────────────────────┐
│ LAYER 1: EPITHELIUM │
│ Thickness: ~50 µm (approx. 10% of total corneal thickness) │
│ Type: Non-keratinized stratified squamous │
│ │
│ Structure (anterior to posterior): │
│ ┌──────────────────────────────────────────────────────┐ │
│ │ Surface cells (2 layers) │ │
│ │ - Squamous, flattened, pyknotic nuclei │ │
│ │ - Microplicae + microvilli on outer surface │ │
│ │ - These anchor the TEAR FILM mucin layer │ │
│ │ - Shed into tear film every few days │ │
│ ├──────────────────────────────────────────────────────┤ │
│ │ Wing cells (2-3 layers) │ │
│ │ - Polyhedral, "wing-shaped" on cross-section │ │
│ │ - Bridge between basal and surface │ │
│ ├──────────────────────────────────────────────────────┤ │
│ │ Basal cells (1 layer) │ │
│ │ - Tall columnar, round nuclei │ │
│ │ - Attached to basement membrane by HEMIDESMOSOMES │ │
│ │ - Site of mitotic activity │ │
│ │ - Most densely innervated (pain fibers here) │ │
│ └──────────────────────────────────────────────────────┘ │
│ │
│ Basement membrane (epithelial BM) │
│ - Type IV collagen, laminin, fibronectin │
│ - Regenerates after damage │
└─────────────────────────────────────────────────────────────┘
│
│ ★ LIMBAL STEM CELLS (Palisades of Vogt)
│ - Located at corneoscleral junction
│ - Maintain epithelial turnover (7-day cycle)
│ - Guard against conjunctivalization
│ - Clinical: LSCD (Limbal Stem Cell Deficiency) → chronic
│ epithelial defects, vascularization, goblet cells on cornea
│
▼
┌─────────────────────────────────────────────────────────────┐
│ LAYER 2: BOWMAN LAYER (Bowman's Membrane) │
│ Thickness: ~12 µm │
│ │
│ - Acellular (NO cells) │
│ - Composed of randomly arranged collagen fibrils │
│ (type I, III, V) - DIFFERENT from stromal arrangement │
│ - Anterior part of stroma (modified) │
│ - DOES NOT REGENERATE if damaged → replaced by SCAR │
│ - Not a true membrane (no basement membrane structure) │
│ │
│ Clinical significance: │
│ → PRK (photorefractive keratectomy) removes Bowman layer │
│ → Reis-Buckler dystrophy = dystrophy of Bowman layer │
│ → Scarring here = permanent anterior stromal opacity │
└─────────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ LAYER 3: STROMA (Substantia Propria) │
│ Thickness: ~500 µm = 90% of total corneal thickness │
│ │
│ Composition: │
│ - 200+ parallel LAMELLAE of type I collagen fibrils │
│ - Each lamella spans the full corneal diameter │
│ - Regular spacing maintained by PROTEOGLYCAN ground │
│ substance (keratan sulphate + chondroitin sulphate) │
│ - Modified fibroblasts = KERATOCYTES (quiescent) │
│ → Activated keratocytes = "fibroblasts" → scar │
│ │
│ Properties: │
│ - HYDROPHILIC (keratan sulphate attracts water) │
│ - Can SCAR but CANNOT regenerate │
│ - Avascular + alymphatic │
│ │
│ Clinical: │
│ → Corneal oedema = fluid enters stroma → cloudy │
│ → Keratoconus = stromal thinning + ectasia │
│ → Deep stromal scarring → DALK (preserves endothelium) │
└─────────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ LAYER 4: DESCEMET MEMBRANE │
│ Thickness: 10-12 µm (adult) - thickens with age │
│ │
│ - True basement membrane of the endothelium │
│ - Fine latticework of collagen fibrils (type IV + VIII) │
│ - TWO ZONES: │
│ a) Anterior banded zone: deposited IN UTERO │
│ b) Posterior non-banded zone: laid down throughout life │
│ │
│ - REGENERATES (unlike Bowman's) │
│ - Elastic properties - can scrolls/detach (Descemet │
│ detachment) during AC surgery │
│ │
│ Exam points: │
│ → Ruptures in congenital glaucoma = HAAB'S STRIAE │
│ → Ruptures in birth trauma = curvilinear breaks │
│ → Descemet scroll = seen after DMEK graft │
│ → Descemet membrane is transplanted in DMEK surgery │
└─────────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ [DUA LAYER - proposed 6th layer] │
│ Between stroma and Descemet membrane │
│ Significance: Big bubble technique in DALK uses this plane │
│ Controversial - some say it's posterior stroma │
└─────────────────────────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────────┐
│ LAYER 5: ENDOTHELIUM │
│ Thickness: Single monolayer of cells, ~5 µm │
│ │
│ - Monolayer of POLYGONAL (hexagonal) cells │
│ - Cell density: ~3000 cells/mm² in young adult │
│ - Decreases ~0.6% per YEAR with age │
│ - CANNOT REGENERATE (no mitosis in adult) │
│ → Lost cells → remaining cells ENLARGE (polymegethism) │
│ and become irregular (pleomorphism) │
│ │
│ Function: DETURGESCING THE STROMA │
│ - Na/K ATPase pump on basolateral membrane │
│ - Actively pumps ions → water follows osmotically │
│ - Maintains cornea at 78% hydration (normal) │
│ │
│ Critical threshold: <500 cells/mm² → CORNEAL OEDEMA │
│ Surgical threshold: <1000 cells/mm² → high risk for PK │
│ │
│ Examined by: SPECULAR MICROSCOPY │
│ (measures cell count, cell size variation = CV%) │
└─────────────────────────────────────────────────────────────┘
│
▼
POSTERIOR (Anterior Chamber)
Kanski's Corneal Anatomy Diagram (from textbook):
Histology of the Cornea (from Junqueira's Histology):
Corneal Innervation Pathway (high yield for viva):
Trigeminal nerve (CN V)
│
└── Ophthalmic division (V1)
│
└── Nasociliary branch
│
┌──────────┴──────────┐
│ │
Long ciliary nerves Short ciliary nerves
(direct) (via ciliary ganglion)
│
▼
Enter cornea at LIMBUS (radially)
│
▼
Lose myelin sheath at LIMBUS
│
▼
Sub-epithelial nerve plexus
(densest nerve supply in the body)
│
▼
Intraepithelial free nerve endings
(pain fibers - explain why corneal
abrasion = intense pain)
Quick Comparison Table - Bowman vs Descemet (Exam Favourite):
| Feature | Bowman Layer | Descemet Membrane |
|---|---|---|
| Position | Under epithelium | Under stroma |
| Nature | Modified anterior stroma | True basement membrane |
| Collagen type | I, III, V (random) | IV, VIII (lattice) |
| Formed by | Keratocytes | Endothelium |
| Regeneration | NO | YES |
| Disease | Reis-Buckler dystrophy | Fuchs' endothelial dystrophy |
| Rupture sign | - | Haab's striae (congenital glaucoma) |
B. THE SCLERA
SCLERA - "The White of the Eye"
Structure:
- Posterior 5/6 of fibrous coat
- Continuous with cornea at the LIMBUS anteriorly
- Continuous with dural sheath of optic nerve posteriorly
- Thickness:
Posterior (around optic nerve): 1.0 mm (thickest)
Equator: 0.4-0.5 mm
Muscle insertion sites: 0.3 mm (THINNEST - risk of perforation
during strabismus surgery!)
Behind limbus: 0.6 mm
Composition:
- Type I collagen fibrils (randomly arranged - hence OPAQUE)
- Small amount of elastic tissue
- Fibroblasts (scleral cells)
- Rich in proteoglycans
Layers (outer to inner):
1. Episclera - loose vascular connective tissue
- Tenon's capsule overlies it
- Episcleritis = inflammation here
2. Scleral stroma - dense collagen, interlacing bundles
3. Lamina fusca - inner layer, brown pigment, merges with
suprachoroidal space
IMPORTANT ANATOMICAL OPENINGS IN SCLERA:
┌──────────────────────────────────────────────────────┐
│ LAMINA CRIBROSA │
│ - Posterior scleral foramen (sieve-like) │
│ - Optic nerve axons pass through here │
│ - Weakest point of the eye │
│ - Elevated IOP → posterior bowing of lamina │
│ → Axonal injury → glaucomatous optic neuropathy │
├──────────────────────────────────────────────────────┤
│ EMISSARY CANALS │
│ - Anterior: long posterior ciliary arteries (×2) │
│ - Equatorial: vortex veins (×4) │
│ - Around optic nerve: short posterior ciliary │
│ arteries (×6-8) → form circle of Zinn │
└──────────────────────────────────────────────────────┘
Blood supply: Sparse - from episcleral vessels
(Why sclera heals slowly, scleritis is painful)
Nerve supply: V1 (ophthalmic division)
- Scleritis (deep, boring pain) vs Episcleritis (superficial, less painful)
- Blue sclera → osteogenesis imperfecta (thin sclera shows underlying uvea)
- Staphyloma = ectatic, bulging sclera lined by uvea (in high myopia, advanced glaucoma)
- Scleral buckle surgery → used in RD repair (indent the sclera to support the retinal break)
COAT 2: THE UVEAL (MIDDLE / VASCULAR) COAT
A. THE IRIS
IRIS - ANATOMY
Position: Anterior uvea, in coronal plane, perforated centrally = PUPIL
Color: From melanocyte density in STROMA (not pigment epithelium)
LAYERS (anterior to posterior):
┌────────────────────────────────────────────────────────┐
│ 1. ANTERIOR BORDER LAYER (not a true membrane) │
│ - Discontinuous layer of fibroblasts + melanocytes │
│ - Crypts of Fuchs = gaps in this layer │
│ - Color of iris determined here │
├────────────────────────────────────────────────────────┤
│ 2. STROMA │
│ - Loose connective tissue │
│ - Contains: │
│ a) Sphincter pupillae muscle │
│ - Circular, near pupil margin │
│ - Parasympathetic (CN III → EW nucleus → │
│ ciliary ganglion → short ciliary nerves) │
│ - Action: MIOSIS (constriction) │
│ b) Blood vessels (radial) │
│ - Major arterial circle at iris root │
│ - Minor arterial circle near pupil margin │
│ c) Melanocytes, fibroblasts, clump cells │
├────────────────────────────────────────────────────────┤
│ 3. DILATOR PUPILLAE MUSCLE (myoepithelial) │
│ - Radial fibers │
│ - Sympathetic (superior cervical ganglion → nasocil │
│ iary → long ciliary nerve) │
│ - Action: MYDRIASIS (dilation) │
├────────────────────────────────────────────────────────┤
│ 4. PIGMENT EPITHELIUM (2 layers) │
│ - Anterior layer = dilator muscle (myoepithelial) │
│ - Posterior layer = heavily pigmented │
│ - Continuous with ciliary epithelium │
└────────────────────────────────────────────────────────┘
Pupil Control Flowchart:
LIGHT (bright) ──────────────────────► DARK
│ │
▼ ▼
Parasympathetic Sympathetic
(CN III EW nucleus) (Hypothalamus → T1 →
│ Sup. cervical ganglion →
▼ nasociliary → long ciliary)
Sphincter pupillae │
(circular muscle) ▼
│ Dilator pupillae
▼ (radial muscle)
MIOSIS │
(constriction) ▼
MYDRIASIS
(dilation)
Drug effects:
Pilocarpine → mimics parasympathetic → MIOSIS
Tropicamide/Atropine → blocks parasympathetic → MYDRIASIS
Phenylephrine → stimulates sympathetic → MYDRIASIS
Cocaine → blocks noradrenaline reuptake → MYDRIASIS
B. THE CILIARY BODY
CILIARY BODY - the "engine" of the anterior eye
Shape: Ring-shaped, between iris root and ora serrata
Divisions:
┌─────────────────────────────────────────────────────┐
│ PARS PLICATA (anterior 2mm) │
│ = 70 ciliary processes │
│ - Secretes aqueous humor │
│ - Zonule fibers attach here │
│ - Vascular, folded │
├─────────────────────────────────────────────────────┤
│ PARS PLANA (posterior 4mm) │
│ = flat part │
│ - Safe zone for surgical entry (vitrectomy, │
│ intravitreal injections, drainage implants) │
│ - Entry at 3.5 mm (phakic) or 3.0 mm (aphakic) │
│ from limbus │
└─────────────────────────────────────────────────────┘
CILIARY EPITHELIUM (2 layers):
Outer pigmented layer (continuation of RPE)
Inner non-pigmented layer → secretes AQUEOUS HUMOR
(aqueous production by active secretion via Na/K ATPase
+ carbonic anhydrase)
CILIARY MUSCLE (3 parts):
Longitudinal fibers }
Radial fibers } - All parasympathetic
Circular fibers } (CN III)
Action: Contract → zonules RELAX → lens becomes
MORE CONVEX → increases refractive power
= ACCOMMODATION (near vision)
ZONULES OF ZINN (Zonular Fibers):
- Suspend the lens from ciliary processes
- Attachment zones on lens capsule:
Anterior zone (2mm from equator)
Equatorial zone
Posterior zone (1mm from equator)
- Composition: Fibrillin (FBN1/FBN2)
- Weakness: Marfan syndrome (FBN1 mutation) →
subluxated lens
C. THE CHOROID
CHOROID - the highly vascular posterior uvea
Extent: From ora serrata to optic nerve
Thickness: ~0.25 mm (thinning with age)
Color: Brown-red (melanocytes + vessels)
LAYERS (outer to inner):
┌────────────────────────────────────────────────────────┐
│ 1. HALLER'S LAYER (outer vessels) │
│ - Large caliber choroidal arteries and veins │
├────────────────────────────────────────────────────────┤
│ 2. SATTLER'S LAYER (medium vessels) │
│ - Medium-sized vessels │
├────────────────────────────────────────────────────────┤
│ 3. CHORIOCAPILLARIS │
│ - Dense capillary network │
│ - Lobular arrangement │
│ - FENESTRATED endothelium (allows transport) │
│ - Supplies outer 1/3 of retina (including │
│ photoreceptors and RPE) │
│ - HIGHEST BLOOD FLOW of any tissue in body │
├────────────────────────────────────────────────────────┤
│ 4. BRUCH'S MEMBRANE │
│ - 5-layer structure: │
│ a) RPE basement membrane │
│ b) Inner collagenous zone │
│ c) Elastic zone │
│ d) Outer collagenous zone │
│ e) Endothelial BM of choriocapillaris │
│ - Acts as FILTRATION BARRIER │
│ - Thickens with age → drusen form here │
│ - Breaks in AMD → CNV (new vessels grow through) │
└────────────────────────────────────────────────────────┘
Blood supply:
SHORT POSTERIOR CILIARY ARTERIES (6-8)
→ from ophthalmic artery → pierce sclera near optic nerve
→ Circle of Zinn (Haller) → supplies posterior choroid
LONG POSTERIOR CILIARY ARTERIES (2)
→ pierce sclera further anteriorly
→ run in suprachoroidal space
→ supply anterior choroid, ciliary body, iris
→ form MAJOR ARTERIAL CIRCLE of iris
ANTERIOR CILIARY ARTERIES (×7)
→ from extraocular muscles → enter anteriorly
Venous drainage: VORTEX VEINS (×4, one per quadrant)
→ pierce sclera at equator → drain into ophthalmic veins
Functions:
1. Nutritive: supplies outer retina (photoreceptors)
2. Thermoregulatory: cools the retina
3. Haemodynamic: maintains blood supply despite
pressure fluctuations (autoregulation)
4. Optical: melanin absorbs scattered light (reduces
optical noise) - loss in albinism → poor vision
COAT 3: THE RETINA (INNER / NEURAL COAT)
The 10 Layers - Master Diagram
CHOROID (outside)
│
│ [OUTER BLOOD-RETINAL BARRIER]
│ = RPE tight junctions (zonulae occludentes)
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 1: RETINAL PIGMENT EPITHELIUM (RPE) ║
║ - Single layer of cuboidal cells ║
║ - Hexagonal when viewed face-on ║
║ - Rich in MELANIN (absorbs stray light) ║
║ - Tight junctions = outer blood-retinal barrier ║
║ Functions: ║
║ a) Phagocytose shed outer segments of photoreceptors║
║ (daily, ~10% of OS shed each morning) ║
║ b) Transport nutrients from choroid to photoreceptors║
║ c) Regenerate 11-cis retinal (visual cycle) ║
║ d) Maintain subretinal space dry ║
║ Disease: Dry AMD = drusen accumulate under RPE ║
║ Wet AMD = CNV breaks through RPE ║
║ Stargardt = ABCA4 mutation → RPE lipofuscin ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 2: PHOTORECEPTOR LAYER (Rods + Cones) ║
║ ║
║ RODS (~120 million) CONES (~6 million)║
║ - Long, thin - Shorter, wider ║
║ - Photopigment: RHODOPSIN - 3 types (S/M/L) ║
║ - Sensitive: dim light - Color + acuity ║
║ - Location: PERIPHERAL retina - Location: MACULA║
║ - Fovea: ABSENT - Fovea: ONLY cones║
║ - Night blindness if lost - Central vision ║
║ ║
║ STRUCTURE OF PHOTORECEPTORS: ║
║ ┌─────────────────┐ ║
║ │ OUTER SEGMENT │ ← stacked membranous discs ║
║ │ (OS) │ ← contains visual pigment ║
║ ├─────────────────┤ ← connecting cilium ║
║ │ INNER SEGMENT │ ← mitochondria (IS) ║
║ │ (IS) │ ← site of photopigment synthesis ║
║ ├─────────────────┤ ← outer limiting membrane ║
║ │ CELL BODY │ ║
║ ├─────────────────┤ ║
║ │ SYNAPTIC BODY │ ← connects to bipolar cells ║
║ └─────────────────┘ ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 3: EXTERNAL LIMITING MEMBRANE (ELM) ║
║ - Not a true membrane ║
║ - Row of junctional complexes between photoreceptors ║
║ and Müller cells ║
║ - Seen as bright line on OCT ║
║ - Integrity correlates with VISUAL ACUITY ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 4: OUTER NUCLEAR LAYER (ONL) ║
║ - Cell bodies (nuclei) of RODS AND CONES ║
║ - Rods have single row; cones have multiple rows ║
║ - Thickest at macula (cone-rich) ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 5: OUTER PLEXIFORM LAYER (OPL) ║
║ - Synaptic connections: ║
║ Photoreceptor axons ↔ Bipolar cells ║
║ Horizontal cells also here ║
║ - Outer fiber layer of Henle at macula ║
║ (radially arranged fibers = why hard exudates form ║
║ "star" pattern at macula in HTN retinopathy/EDema)║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 6: INNER NUCLEAR LAYER (INL) ║
║ Contains nuclei of 4 cell types: ║
║ a) BIPOLAR CELLS - vertical signal transmission ║
║ b) HORIZONTAL CELLS - lateral modulation at OPL ║
║ c) AMACRINE CELLS - lateral modulation at IPL ║
║ d) MÜLLER CELLS - span entire retina, support cells ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 7: INNER PLEXIFORM LAYER (IPL) ║
║ - Synaptic connections: ║
║ Bipolar cells ↔ Ganglion cells ║
║ Amacrine cells modulate here ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 8: GANGLION CELL LAYER (GCL) ║
║ - Cell bodies of retinal ganglion cells (RGC) ║
║ - ~1.2 million RGCs → their axons form optic nerve ║
║ - At fovea: GCL cells displaced to periphery ║
║ (Henle layer) - allows direct light to cones ║
║ - LOST IN GLAUCOMA (retrograde degeneration) ║
║ - OCT can measure GCL thickness ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 9: NERVE FIBER LAYER (NFL) ║
║ - Axons of RGCs run parallel to retinal surface ║
║ - CONVERGE at optic disc ║
║ - Arcuate bundles above/below macula ║
║ - RNFL measured by OCT → glaucoma detection ║
║ - RNFL defect = "wedge defect" on red-free photos ║
╚═══════════════════════════════════════════════════════╝
│
▼
╔═══════════════════════════════════════════════════════╗
║ LAYER 10: INTERNAL LIMITING MEMBRANE (ILM) ║
║ - Basement membrane of Müller cells ║
║ - Separates retina from vitreous ║
║ - Peeled during macular hole surgery ║
║ - Vitreous attached firmly here ║
╚═══════════════════════════════════════════════════════╝
│
▼
VITREOUS CAVITY (inside)
│
│ [INNER BLOOD-RETINAL BARRIER]
│ = tight junctions of retinal capillary
│ endothelium (zonulae occludentes)
H&E Histology of the Retina (from textbook):
Memory Trick for 10 Layers (Outer to Inner):
"Really Pretty Ellens Often Order Interesting Ice-cold
Gangrene-Noodle Iced-lattes"
R = RPE
P = Photoreceptors
E = External limiting membrane
O = Outer nuclear layer
O = Outer plexiform layer
I = Inner nuclear layer
I = Inner plexiform layer
G = Ganglion cell layer
N = Nerve fiber layer
I = Internal limiting membrane
Special Retinal Regions
THE MACULA (Macula lutea)
Location: 3-4 mm temporal to optic disc, centered at fovea
Size: ~5.5 mm diameter
Yellow color: Xanthophyll pigments (lutein + zeaxanthin)
in inner retinal layers → Haidinger's brush
Zones (center outward):
┌────────────────────────────────────────────────────┐
│ Foveola (0.35 mm) ← center of fovea │
│ - Cones ONLY (no rods, no blood vessels) │
│ - No ganglion cells / no inner nuclear layer │
│ - Thinnest part of retina (~0.13 mm) │
│ - Highest visual acuity │
│ - Müller cells form Henle's fiber layer │
│ │
│ Fovea centralis (1.5 mm) │
│ - Pit-shaped depression │
│ - GCL cells displaced outward (foveal rim) │
│ - Cones most tightly packed (1 cone per RGC here) │
│ │
│ Parafovea (ring, 0.5 mm wide) │
│ - Thickest GCL (8-9 layers of ganglion cells) │
│ │
│ Perifovea (ring, 1.5 mm wide) │
│ - Transitional zone to peripheral retina │
└────────────────────────────────────────────────────┘
FAZ = Foveal Avascular Zone (0.4 mm diameter)
- No capillaries
- Detected on FFA and OCT-A
- Enlarged FAZ = ischemia (DR, sickle cell)
THE OPTIC DISC (Optic Nerve Head)
Location: Nasal to posterior pole, 15° nasal to fovea
Size: ~1.5 mm × 1.75 mm (vertical > horizontal)
Content: 1.2 million RGC axons enter here
Cup: Central pale area = physiological cup
Normal C/D ratio: 0.3-0.4 (up to 0.6)
Rim: ISNT rule (Inferior > Superior > Nasal > Temporal)
Violation = glaucoma sign
Lamina cribrosa: Sieve plate where axons exit sclera
Fovea is ~3 disc diameters lateral to disc
Blind spot = corresponds to optic disc (no photoreceptors)
Located 15° temporal to fixation point
THE LENS
LENS - the adjustable focusing element
Shape: Biconvex (more curved posteriorly)
Dimensions:
Adult: 9-10 mm diameter, 4-5 mm thick (thickens with age)
Newborn: More spherical
Power: ~18-20 D at rest (increases to ~33 D during accommodation)
BLOOD SUPPLY: NONE - completely avascular
NERVE SUPPLY: NONE
NUTRITION: From aqueous humor (glucose, amino acids, O2)
STRUCTURE (outside in):
┌──────────────────────────────────────────────────────────┐
│ CAPSULE │
│ - Thickest BM in body │
│ - Composition: Type IV collagen + laminin │
│ - Continuous elastic membrane │
│ - THICKEST: Anterior subcapsular (14 µm) │
│ - THINNEST: Posterior subcapsular (4 µm) │
│ → PSC most vulnerable to trauma (posterior thin cap) │
│ - Zonules insert into anterior and posterior capsule │
├──────────────────────────────────────────────────────────┤
│ ANTERIOR EPITHELIUM │
│ - Single layer of cuboidal cells (only on ANTERIOR) │
│ - No epithelium on posterior surface │
│ - Equatorial cells → continue to multiply throughout │
│ life → elongate → form new lens FIBERS │
│ - Site of: │
│ a) Anterior subcapsular cataract (trauma/steroids) │
│ b) PCO formation (after cataract surgery) │
│ - Germinative zone at equator = mitotic activity │
├──────────────────────────────────────────────────────────┤
│ CORTEX │
│ - Youngest lens fibers (most recently formed) │
│ - Soft, hydrated │
│ - Nuclei present in outermost fibers │
│ - Site of cortical cataract (spoke-like opacities) │
├──────────────────────────────────────────────────────────┤
│ NUCLEUS │
│ - Oldest, most central lens fibers │
│ - HARDEST part of lens (compressed, dehydrated) │
│ - Further divided (from outside in): │
│ Fetal nucleus (soft) │
│ Embryonic nucleus (softer) │
│ Adult nucleus │
│ - Nuclear cataract: yellow-brown coloration (hardening) │
│ - BRUNESCENT cataract = very hard, dark brown │
└──────────────────────────────────────────────────────────┘
LENS SUTURES:
- Y-shaped sutures where fiber ends meet
- Anterior: upright Y-suture
- Posterior: inverted Y-suture (λ)
- In fetal nucleus: prominent (seen on slit lamp)
- Clinical: "Flower cataract" = opacity along suture lines
LENS METABOLISM:
Primary pathway: ANAEROBIC GLYCOLYSIS (85%)
→ Lens is avascular → mainly anaerobic
→ Glucose → pyruvate → lactate (Embden-Meyerhof)
Sorbitol pathway (HMP shunt):
→ Glucose → Aldose reductase → SORBITOL
→ In DIABETES: excess glucose → excess sorbitol
→ Sorbitol cannot leave cell → osmotic swelling
→ Hydration cataract → "snowflake cataract" in juvenile DM
THE VITREOUS
VITREOUS HUMOR
Volume: 4-5 mL (largest compartment of the eye)
Location: Vitreous cavity = between lens and retina
Composition:
- 99% WATER
- Collagen fibrils (type II) → form scaffold
- Hyaluronic acid (hyaluronan) → binds water, gives gel texture
- Hyalocytes (modified macrophages, at vitreous surface)
- No blood vessels, no nerves
STRUCTURE:
┌──────────────────────────────────────────────────────┐
│ VITREOUS BASE │
│ - Strongest attachment to retina │
│ - Straddles ora serrata (2mm anterior + 3mm │
│ posterior to ora serrata) │
│ - Cannot be separated without tearing retina │
│ - Site of dialysis tears in trauma │
├──────────────────────────────────────────────────────┤
│ ANTERIOR VITREOUS FACE │
│ - Borders posterior lens capsule │
│ - Wieger's ligament (hyaloidocapsular ligament) │
│ attaches vitreous to posterior lens capsule │
├──────────────────────────────────────────────────────┤
│ VITREOUS CORTEX │
│ - Condensed peripheral gel │
│ - Hyalocytes located here │
├──────────────────────────────────────────────────────┤
│ CLOQUET'S CANAL │
│ - Remnant of hyaloid artery (fetal circulation) │
│ - Runs from optic disc to posterior lens capsule │
│ - Usually invisible in adults │
│ - Persistent: Mittendorf dot (posterior lens), │
│ Bergmeister's papilla (optic disc) │
└──────────────────────────────────────────────────────┘
VITREOUS ATTACHMENTS (firm → loose):
1. Vitreous base (FIRMEST - cannot separate)
2. Optic disc margin
3. Fovea
4. Posterior lens capsule
5. Along retinal vessels
6. Posterior cortex (loosest - separates first in PVD)
POSTERIOR VITREOUS DETACHMENT (PVD):
PVD = separation of vitreous cortex from retina
(EXCEPT at vitreous base - never separates here)
Process:
Age → syneresis (vitreous liquefaction, gel → sol)
→ Collagen fibrils aggregate → liquid pools form
→ Liquid vitreous enters retrocortical space
→ Cortex detaches from retina
→ WEISS RING = annular condensate around optic disc
Symptoms: Sudden floaters + photopsias (flashes)
Risk: If vitreoretinal traction → RETINAL TEAR → RD
Always dilate pupil and examine peripheral retina!
THE ANTERIOR AND POSTERIOR CHAMBERS
ANTERIOR CHAMBER
Anterior boundary: Posterior surface of cornea
Posterior boundary: Anterior surface of iris + pupil + lens
Angle: Trabecular meshwork, Schwalbe's line, Schlemm's canal
Volume: ~0.25 mL
Contents: Aqueous humor
POSTERIOR CHAMBER
Anterior boundary: Posterior surface of iris
Posterior boundary: Anterior vitreous face
Lateral: Ciliary body
Volume: ~0.06 mL
Contents: Aqueous humor + Zonules
AQUEOUS FLOW PATH:
Ciliary processes (pars plicata)
│
▼
Posterior chamber
│
▼ (through pupil)
Anterior chamber
│
▼
Trabecular meshwork (at angle) → Schlemm's canal
│ │
90% outflow ▼
Aqueous veins
│
▼
Episcleral veins
│
10% outflow (uveoscleral)
│
▼
Supraciliary space → suprachoroidal space → sclera
COMPLETE SUMMARY DIAGRAM - LAYERS OF THE EYEBALL
╔══════════════════════╗
║ CROSS-SECTION ║
║ OF THE EYE ║
╚══════════════════════╝
ANTERIOR POLE
│
┌───────────┼───────────┐
│ CORNEA │ ← Fibrous coat (1/6)
│ (5 layers: E-B-S-D-E)│ Refracts 43 D
│ │ │
│ Anterior Chamber │
│ │ │
│ IRIS ─ pupil │ ← Uveal coat (anterior)
│ (sphincter/dilator)│
│ │ │
│ Posterior Chamber │
│ │ │
│ Ciliary body │ ← Uveal coat (middle)
│ (pars plicata/plana) │ secretes aqueous
│ │ │
│ LENS │ ← Biconvex, avascular
│ (capsule/epi/cortex │ 18-20 D
│ /nucleus) │
│ │ │
│ ────────────────────│
├─SCLERA (5/6 fibrous)──┤ ← Opaque, collagen
│ ┌──────────────────┐ │
│ │ CHOROID │ │ ← Uveal coat (posterior)
│ │ (Haller/Sattler │ │ High blood flow
│ │ /choriocapil │ │
│ │ /Bruch's) │ │
│ └──────────────────┘ │
│ ┌──────────────────┐ │
│ │ RETINA │ │ ← Neural coat
│ │ (10 layers) │ │ Inner: NFL/GCL/IPL
│ │ RPE outside │ │ Middle: INL/OPL/ONL
│ │ │ │ Outer: ELM/PR/RPE
│ └──────────────────┘ │
│ │
│ VITREOUS │ ← 99% water, 4-5 mL
│ (gel, 4-5 mL) │ Type II collagen
│ │ Hyaluronic acid
└───────────────────────┘
│
POSTERIOR POLE
(optic disc + macula)
HIGH-YIELD EXAM BULLET POINTS ★★★
- Cornea = anterior 1/6 of eyeball; Sclera = 5/6
- Cornea is 43 D (total eye ~60 D)
- Corneal thickness: center 0.5 mm (500 µm), periphery 1 mm
- Corneal endothelial density: ~3000/mm² young adult, falls 0.6%/year
- Corneal oedema when density < 500/mm²
- Surgical risk when density < 1000/mm²
- Descemet: anterior banded (in utero) + posterior non-banded (postnatal)
- Retina has exactly 10 layers (RPE = outermost, ILM = innermost)
- Vitreous = 4-5 mL (largest compartment), 99% water
- Foveola = only cones, NO rods, NO blood vessels, NO ganglion cells
- Lens: avascular, no nerves, metabolism primarily anaerobic glycolysis
- 1.2 million RGC axons form the optic nerve
- Choroid = highest blood flow per unit weight of any tissue in body
- Bowman's layer cannot regenerate → permanent scar (hence no steroid use in active HSV)
- Descemet can regenerate → basis of DMEK graft healing
- Stroma = 90% of cornea → diseases here (keratoconus) → structural weakness
- Choriocapillaris fenestrated → leaks on FFA → "background choroidal flush"
- Müller cells span all 10 retinal layers → their end-feet form ILM
- Vitreous base = strongest attachment → dialysis tears at this site in blunt trauma
- Pars plana (4 mm) = safe surgical entry zone for vitrectomy
- Haab's striae = Descemet ruptures due to elevated IOP in congenital glaucoma
- Limbal stem cell deficiency (LSCD) → conjunctivalization of cornea → vascularization
IS THIS NOTE ENOUGH?
What the Note DOES Cover Well ✅
- All 5 corneal layers with cellular detail, clinical correlations, and histology images
- Corneal transparency mechanism (4 factors)
- Bowman vs Descemet comparison table
- Corneal innervation pathway (flowchart)
- Sclera - layers, thickness variations, emissary canals, lamina cribrosa
- Uveal tract - iris muscles + nerve supply (flowchart), ciliary body divisions, choroidal layers + Bruch's membrane
- All 10 retinal layers with cell types, functions, and clinical diseases linked to each
- Macula zones (foveola → fovea → parafovea → perifovea), FAZ, optic disc
- Lens - capsule, epithelium, cortex, nucleus, metabolism, zonules
- Vitreous - structure, attachments, Cloquet's canal, PVD
- Aqueous flow pathway
- High-yield number facts + clinico-anatomical correlations
What is MISSING or Needs Addition ❌
1. Embryology of the Eye
- Optic vesicle → optic cup formation
- Which structure comes from which origin (neural ectoderm vs surface ectoderm vs neural crest vs mesoderm)
- Fetal fissure (choroidal fissure) closure → failure = coloboma (which structures affected, where, appearance)
- Hyaloid artery regression → persistence = persistent fetal vasculature (PFV)
- Myelination of optic nerve (stops at lamina cribrosa → why optic nerve head is normally pink, not white)
2. Limbus (detailed)
- Anatomy of the limbus (where cornea meets sclera)
- Trabecular meshwork structure (uveal/corneoscleral/juxtacanalicular)
- Schlemm's canal
- Schwalbe's line, Sampaolesi's line
- Gonioscopic landmarks (critical for glaucoma)
- Palisades of Vogt (limbal stem cells)
3. Optic Nerve Head Anatomy
- 4 parts of optic nerve (intraocular, intraorbital, intracanalicular, intracranial)
- Blood supply of optic nerve head (SPCA → Circle of Zinn-Haller)
- Physiological cup vs glaucomatous cupping
- ISNT rule explained anatomically
4. Blood Supply Summary (all structures together)
- Central retinal artery (inner 2/3 retina) vs choriocapillaris (outer 1/3 retina)
- Why retinal artery occlusion spares photoreceptors initially (dual supply at fovea - actually NO central retinal supply at fovea → choroid only at fovea = why CRAO spares central vision when cilioretinal artery present)
5. Aqueous Humor Composition
- Compared to plasma (ascorbate higher, protein lower)
- Goldman equation (IOP formula)
- Uveoscleral outflow pathway detail
6. Applied Anatomy (Surgical)
- Where surgeons cut and why
- Phacoemulsification: why CCC (continuous curvilinear capsulorhexis) works on anterior capsule
- Why posterior capsule rupture is serious (thin, no epithelium)
- Pars plana entry distances (phakic 3.5 mm, pseudophakic 3.0 mm, aphakic 2.5-3.0 mm)
Honest Verdict
- Embryology (directly tested in written theory)
- Limbus + Gonioscopic anatomy (critical for glaucoma section)
- Optic nerve head anatomy (bridges into neuro-ophthalmology and glaucoma)
YES
- Full embryology timeline (Day 22 to postnatal year 2) with 3 textbook diagrams
- Every congenital anomaly mapped to its developmental failure
- Tissue origin table (neuroectoderm / surface ectoderm / neural crest / mesoderm)
- Choroid fissure, coloboma, PFV, hyaloid system - all detailed
- Limbus anatomy with full trabecular meshwork layers
- Gonioscopic landmarks (Schwalbe's → iris root) with memory trick
- Shaffer grading + van Herick grading
- Complete aqueous dynamics with Goldman equation
- Optic nerve 4 parts
- Optic nerve head blood supply (why SPCA matters for glaucoma)
- ISNT rule, C/D ratio, PPA (alpha/beta zones)
IS THIS ENOUGH?
Parts 1 + 2 Together = COMPLETE for Week 1
What You Now Have ✅
- Cornea - all 5 layers (+ Dua layer), transparency mechanism, innervation, Bowman vs Descemet comparison, limbal stem cells, 2 histology diagrams from textbooks
- Sclera - layers, thickness at key points, emissary canals, lamina cribrosa
- Uveal tract - iris muscles + autonomic pathways (flowchart), ciliary body divisions, choroidal layers + Bruch's membrane
- Retina - all 10 layers with cell types, blood-retinal barriers, macular zones (foveola/fovea/parafovea/perifovea), FAZ, optic disc
- Lens - capsule/epithelium/cortex/nucleus, sutures, metabolism (sorbitol pathway), zonules
- Vitreous - structure, attachments (firmest to loosest), Cloquet's canal, PVD
- Full tissue origin table (4 sources → all structures)
- Week-by-week timeline (Day 22 to postnatal year 2)
- Optic cup, lens placode, choroid fissure, hyaloid system
- All congenital anomalies mapped to developmental failures
- Key gene mutations (PAX6, PAX2, CHX10)
- 3 embryology diagrams from Langman's + Moore
- TM 3 layers (uveal/corneoscleral/juxtacanalicular)
- Gonioscopic landmarks with memory trick
- Shaffer grading + van Herick
- Goldman equation + aqueous dynamics
- Both outflow pathways with drug targets
- 4 segments with dimensions
- Blood supply by level (CRA vs SPCA vs pial)
- ISNT rule, C/D ratio, PPA zones
What Is NOT in These Notes (Intentionally Left for Later)
| Topic | When to Study |
|---|---|
| Orbit + orbital walls + foramina | Week 2 |
| Extraocular muscles - actions, nerve supply | Week 2 |
| Optic pathway + visual field defects | Week 2 |
| Pupillary pathway (RAPD, Horner) | Week 2 / Neuro-ophthal |
| Lacrimal system anatomy | Week 3 (Adnexa) |
| Eyelid layers | Week 3 (Adnexa) |
| Conjunctiva | Week 3 (Adnexa) |
Bottom Line
IS APPLIED ANATOMY HAS BEEN ADDED?
What Applied Anatomy IS Already in the Notes
- Corneal abrasion → intense pain (dense innervation explanation)
- HSV keratitis → reduced corneal sensation → neurotrophic keratopathy
- Bowman's doesn't regenerate → permanent scar (no steroid in active HSV)
- Descemet regenerates → basis of DMEK healing
- Endothelial count thresholds (500 = oedema, 1000 = surgical risk)
- LSCD → conjunctivalization
- PRK removes Bowman's layer
- Keratoconus = stromal thinning
- Thinnest at muscle insertions (0.3mm) → perforation risk in strabismus surgery
- Blue sclera → osteogenesis imperfecta
- Staphyloma in high myopia/advanced glaucoma
- Scleral buckle in RD repair
- Drug effects on pupil (pilocarpine/tropicamide/phenylephrine/cocaine) with mechanism
- Zonule weakness in Marfan syndrome → subluxated lens
- Choriocapillaris fenestrated → leaks on FFA
- FAZ enlargement = ischemia (DR, sickle cell)
- RNFL measured by OCT for glaucoma
- Bruch's breaks in AMD → CNV
- Outer retina supplied by choriocapillaris (not CRA) → why CRAO can spare fovea if cilioretinal artery present
- Sorbitol pathway in diabetes → snowflake cataract
- PSC most vulnerable (posterior capsule thinnest at 4 µm)
- Anterior epithelium = site of PCO after cataract surgery
- Brunescent cataract = very hard nucleus
- Vitreous base strongest → dialysis tears in blunt trauma
- PVD → flashes + floaters → examine periphery for retinal tear
- Pars plana entry distances (3.5mm phakic, 3.0mm pseudophakic)
- Juxtacanalicular meshwork = site of maximum resistance → target of glaucoma surgery
- Sampaolesi line = pseudoexfoliation/pigment glaucoma sign
- Goldman equation for IOP
- Intraorbital segment tortuous → allows eye movement
- SPCA supplies lamina cribrosa → ischaemia here = ION (AION)
- Lamina cribrosa bowing in glaucoma
- ISNT violation = glaucoma
- Beta zone PPA = glaucoma progression marker
What Is MISSING - Dedicated Applied Anatomy Section
1. Surgical Anatomy of the Anterior Segment
- Why CCC works (anterior capsule has epithelium → elastic, tears in circle)
- Why posterior capsule rupture is dangerous (no epithelium, thin 4µm, vitreous follows)
- Phacoemulsification incision anatomy (clear corneal vs scleral tunnel - why scleral is more watertight)
- Why hydrodissection works (fluid wave under capsule separates cortex)
- IOL haptic placement in the bag vs sulcus (anatomical consequences)
- Capsulorhexis edge overlap of IOL optic (prevents PCO - mechanical barrier)
2. Surgical Anatomy of the Posterior Segment
- Pars plana entry points (detailed - distances for 20G/23G/25G/27G)
- Why ILM peel is done in macular hole surgery (removes tractional force)
- Vitreous base cannot be separated → why peripheral breaks are dangerous
- Silicone oil vs gas: buoyancy direction and which breaks they tamponade
3. Surgical Anatomy of the Angle
- Trabeculectomy: why the flap is made at the limbus (access to TM)
- Goniotomy vs trabeculotomy (angle approach vs external approach to TM)
- MIGS procedures and which layer of TM they bypass
4. Clinico-Anatomical Correlations (Quick-fire viva questions)
- Why cornea is avascular but heals poorly → stem cells at limbus (not distributed)
- Why retinal detachment is painless (no sensory nerves in retina)
- Why subretinal fluid accumulates (RPE pump overwhelmed or break)
- Why raised ICP causes papilledema (subarachnoid space communicates with CSF)
- Why glaucoma damages inferior > superior fibers first (arcuate anatomy)
- Why macular disease causes central scotoma (fovea = highest cone density)
- Why cataract causes glare in PSC (pupil constricts in bright light → PSC enters visual axis)
My Recommendation
- Short structured clinical reasoning explanations for each point
- "Why" questions answered with anatomy
- Surgical steps linked to the anatomy we already covered
YES
WEEK 1 EYEBALL ANATOMY - PART 3
Applied and Surgical Anatomy
"The notes that win vivas"
SECTION 1: SURGICAL ANATOMY OF THE ANTERIOR SEGMENT
1.1 - Cataract Surgery (Phacoemulsification)
The Surgical Incision - Why Where We Cut Matters
THREE INCISION OPTIONS - ANATOMY DRIVES CHOICE:
A) CLEAR CORNEAL INCISION (CCI)
┌──────────────────────────────────────────────────────┐
│ Location: 1-2 mm inside corneal limbus │
│ Plane: Through corneal stroma only │
│ Anatomy used: Corneal stroma self-seals (collagen │
│ lamellae parallel to wound edges) │
│ WHY it works: Tunnel construction (3-plane: external │
│ groove → stromal tunnel → internal valve) creates │
│ a valve mechanism - IOP closes the wound │
│ Advantage: Faster, no conjunctival peritomy │
│ Disadvantage: No blood supply (avascular cornea) → │
│ slower healing, higher endophthalmitis risk if │
│ valve fails (hypotony) │
└──────────────────────────────────────────────────────┘
B) SCLERAL TUNNEL INCISION
┌──────────────────────────────────────────────────────┐
│ Location: 2-3 mm behind limbus, in sclera │
│ Anatomy used: Scleral vascularity → better healing │
│ WHY better seal: Scleral collagen = random → wound │
│ swells when hydrated → self-sealing │
│ Advantage: More watertight, less endophthalmitis risk│
│ Better for hard nuclei (less wound burn) │
│ Disadvantage: Needs conjunctival peritomy, more time │
└──────────────────────────────────────────────────────┘
C) LIMBAL (FROWN) INCISION - now largely historical
At limbus - transition zone, moderate healing
INCISION SIZE vs ANATOMY:
Phaco needle: 2.2-2.8 mm
IOL injector: 2.2-3.2 mm (depending on IOL)
Larger incision → more astigmatism (cornea flattens
along incision axis → against-the-rule shift)
PARACENTESIS SITE:
90° away from main incision
Through clear cornea (thin, easily entered)
Allows second instrument + irrigation
Continuous Curvilinear Capsulorhexis (CCC) - Anatomy Behind It
WHY CCC IS POSSIBLE - AND WHY IT WORKS:
The anterior lens capsule = TYPE IV COLLAGEN (elastic)
+ It overlies the ANTERIOR EPITHELIUM (only side with cells)
Properties that make CCC work:
1. Capsule is ELASTIC → when you start a tear and redirect
it, the capsular flap acts as its own guiding force
(like tearing cling film in a controlled circle)
2. Tearing tangentially to the circumference → centripetal
force keeps tear moving in a circle
WHY THE EDGE MUST OVERLAP THE IOL OPTIC:
Anterior capsule edge rests ON the IOL optic surface
→ Creates a MECHANICAL BARRIER (capsular bend)
→ Prevents lens epithelial cells (from equatorial
germinating zone) from migrating onto posterior capsule
→ PREVENTS PCO (Posterior Capsule Opacification)
→ If CCC is too large (doesn't overlap optic) → PCO rate 3-5x higher
WHAT HAPPENS IF CCC RUNS OUT (extends to equator):
Tension vector becomes radial → tear extends into
POSTERIOR CAPSULE → surgical disaster
(vitreous loss, dropped nucleus)
CCC size: Typically 5-5.5 mm (IOL optic = 6 mm, so 0.5 mm overlap each side)
Hydrodissection - The Anatomy
HYDRODISSECTION
= Injection of BSS (balanced salt solution) under the
anterior capsular flap, at capsulo-cortical interface
Anatomy exploited:
Cortex attached to LENS CAPSULE by fine collagen fibrils
(not strongly - just enough to stay in place)
Fluid wave separates:
ANTERIOR CAPSULE ←→ CORTEX ←→ LENS FIBERS
The fluid travels 360° around the equator:
→ separates lens from bag completely
→ Allows nucleus to rotate freely
→ Enables safe phacoemulsification without pulling on zonules
HYDRODELINEATION (different from hydrodissection):
Needle placed WITHIN lens substance
Fluid separates EPINUCLEUS from ENDONUCLEUS
Creates "golden ring" sign
Soft epinucleus shell = protection during phaco
The Posterior Capsule - Why Rupture Is Catastrophic
POSTERIOR CAPSULE vs ANTERIOR CAPSULE - CRITICAL DIFFERENCES:
ANTERIOR CAPSULE POSTERIOR CAPSULE
Thickness 14 µm 4 µm (THINNEST)
Epithelium YES (single layer) NONE
Strength Stronger, elastic Fragile, easily torn
Regeneration YES (from epit) NO
Collagen type Type IV Type IV
WHY PC RUPTURE = SURGICAL EMERGENCY:
1. ANATOMICAL BARRIER IS LOST:
Posterior capsule separates:
- ANTERIOR COMPARTMENT (aqueous, iris, ciliary body, lens)
- POSTERIOR COMPARTMENT (vitreous, retina, choroid)
Loss of this barrier → vitreous moves FORWARD into AC
2. VITREOUS PROLAPSE:
Vitreous = gel, attaches to retina at vitreous base
If pulled anteriorly → TRACTION on retina →
Risk of RETINAL TEAR → RETINAL DETACHMENT
3. DROPPED NUCLEUS:
If lens fragments fall into vitreous cavity →
severe uveitis, secondary glaucoma, retinal injury
→ Requires PPV (pars plana vitrectomy) to retrieve
4. IOL PLACEMENT AFFECTED:
Normal: IOL in the capsular bag (ideal)
PC rupture:
Small → IOL still in bag (if CCC intact)
Large → IOL in sulcus (between iris and anterior capsule)
Very large → IOL on iris (iris-claw) or ACIOL
RECOGNIZING PC RUPTURE INTRAOPERATIVELY:
- Sudden deepening of AC
- Sudden free rotation of nucleus
- Change in fluidics (poor followability)
- "Trampoline" effect of posterior capsule
- Vitreous strands in AC (Weck-cel test)
IOL Placement - Anatomy Determines Position
IOL POSITIONS AND THEIR ANATOMICAL BASIS:
1. IN THE BAG (ideal)
┌──────────────────────────────────────────────────┐
│ Haptics rest in capsular fornix (equatorial bag) │
│ IOL optic centered behind CCC opening │
│ CCC overlaps optic → prevents PCO │
│ Most stable position, predictable power │
│ Required for: toric IOLs, multifocal IOLs │
└──────────────────────────────────────────────────┘
2. CILIARY SULCUS (behind iris, in front of capsular bag)
┌──────────────────────────────────────────────────┐
│ Space between posterior iris surface and │
│ anterior lens capsule = ciliary sulcus │
│ Width: ~0.5 mm │
│ When used: PC rupture with intact anterior │
│ capsule + intact CCC rim │
│ Problem: UGH syndrome (Uveitis-Glaucoma- │
│ Hyphema) if haptic touches iris/ciliary body │
│ IOL optic should be larger (6.5 mm) for sulcus │
│ Not suitable for: toric, multifocal IOLs │
└──────────────────────────────────────────────────┘
3. ANTERIOR CHAMBER (ACIOL)
┌──────────────────────────────────────────────────┐
│ Angle-supported or iris-claw (Artisan) │
│ When: No posterior capsule support at all │
│ Problem: Close proximity to corneal endothelium │
│ → Progressive endothelial cell loss │
│ → Bullous keratopathy (if cell count drops <500) │
│ → Needs specular microscopy monitoring │
└──────────────────────────────────────────────────┘
4. SCLERAL FIXATION (Yamane technique, etc.)
┌──────────────────────────────────────────────────┐
│ Haptics tunnelled through sclera and buried │
│ When: No capsular support + inadequate sulcus │
│ Anatomy: Haptic exits through pars plana region │
│ (3.0-4.0 mm from limbus) │
└──────────────────────────────────────────────────┘
PCO (Posterior Capsule Opacification) - Pure Applied Anatomy
PCO = Most common complication of cataract surgery
ANATOMY OF PCO FORMATION:
Source of cells: Equatorial lens epithelial cells
(Germinating zone - these cells were NOT removed during surgery)
They are ALWAYS left behind (impossible to remove safely)
PATHWAY:
Residual equatorial epithelial cells
│
▼ (post-surgery, no longer inhibited by nucleus)
Proliferate (E→A transformation: epithelial → myofibroblastic)
│
▼
Migrate POSTERIORLY along capsular bag
│
▼
Reach POSTERIOR CAPSULE → deposit fibrous material
│
├── FIBROTIC type: Wrinkled, fibrous membrane
│ = Elschnig's pearls (globular cell clusters)
│ = Soemmering's ring (equatorial accumulation)
└── REGENERATIVE type: Lens fiber regeneration
PREVENTION (anatomical reasoning):
1. CCC overlap of IOL optic = capsular bend = mechanical barrier
2. Sharp-edged IOL (square edge design) = creates 360° barrier
at posterior capsule → cells cannot migrate across
3. Hydrophobic acrylic IOL = better capsule adherence
4. Complete cortex removal = fewer residual cells
TREATMENT: YAG LASER CAPSULOTOMY
Nd:YAG laser → focused on posterior capsule
→ Photodisruption → creates central opening in PCO
Energy: ~1-3 mJ per pulse
Risks of YAG:
- IOL pitting (if aimed too anteriorly)
- IOP spike (immediate) → pre-treat with apraclonidine
- CME (cystoid macular edema) - rare
- Retinal detachment (1-3% increase in risk)
(vitreous moves forward → traction on peripheral retina)
SECTION 2: SURGICAL ANATOMY OF THE POSTERIOR SEGMENT
2.1 - Pars Plana Vitrectomy (PPV) - Entry Site Anatomy
WHY PARS PLANA IS THE SAFE ENTRY ZONE:
Pars plana = posterior flat part of ciliary body (4 mm width)
Extends: 2 mm posterior to ora serrata
to 7 mm posterior to limbus
WHAT'S SAFE ABOUT IT:
- No lens fibers (zonules attach to pars plicata, not plana)
- No ciliary processes (so no aqueous disruption)
- Thin, flat epithelium (easy to cut)
- Retina starts at ORA SERRATA (3.5-4 mm from limbus)
→ entry just anterior to ora = no retinal damage
- Iris and lens are well anterior → not at risk
ENTRY DISTANCES FROM LIMBUS:
┌─────────────────────────────────────────────────────┐
│ PHAKIC EYE (lens in place): │
│ 3.5 mm from limbus │
│ (further back to avoid hitting the lens) │
│ │
│ PSEUDOPHAKIC EYE (IOL in place): │
│ 3.0 mm from limbus │
│ (IOL cannot be damaged by needle) │
│ │
│ APHAKIC EYE (no lens): │
│ 2.5-3.0 mm from limbus │
│ │
│ PEDIATRIC (young child): │
│ 2.0-2.5 mm (smaller eye, pars plana is shorter) │
│ In infants: transvitreal approach may be needed │
└─────────────────────────────────────────────────────┘
PORT PLACEMENT (3-port PPV):
┌─────────────────────────────────────────────────────┐
│ SUPERIOR TEMPORAL (infusion cannula) │
│ │ │
│ ┌────┴────┐ │
│ SUPERIOR│ LENS │SUPERIOR │
│ NASAL │ or │TEMPORAL │
│ (light │ PUPIL │(vitrector/ │
│ pipe) │ │ forceps) │
│ └─────────┘ │
│ │
│ Infusion always placed SUPEROTEMPORALLY first │
│ → Confirm tip is in vitreous cavity before opening │
│ (if in suprachoroidal space → choroidal detachment)│
└─────────────────────────────────────────────────────┘
GAUGE SYSTEMS:
20G (0.9 mm) - older, suture required, larger wound
23G (0.6 mm) - transconjunctival sutureless
25G (0.5 mm) - most common currently, sutureless
27G (0.4 mm) - smallest, minimal trauma, slower
2.2 - ILM Peel - Why and How (Anatomy-Based)
INTERNAL LIMITING MEMBRANE (ILM) PEEL
Used in: Macular hole surgery, ERM (epiretinal membrane), DME
ANATOMY OF THE ILM:
= Basement membrane of MÜLLER CELLS
= Innermost layer of retina (Layer 10)
= Thickness: 1-3 µm at fovea (thinnest), up to 6 µm elsewhere
= Composition: Collagen IV, laminin, fibronectin, agrin
WHY ILM IS PEELED IN MACULAR HOLE:
Normal: Vitreous attached to ILM
In macular hole: Vitreous detaches but leaves behind:
→ Cortical vitreous remnants on ILM surface
→ These exert TANGENTIAL TRACTION on the fovea
→ ILM itself is RIGID → acts as scaffold for tractional forces
Peeling ILM:
→ Removes tractional force completely (no scaffold left)
→ Removes vitreous cortex remnants
→ Allows edges of macular hole to fall inward and close
→ Müller cells at hole edge can regenerate
→ Closure rate: ~95% with ILM peel vs ~60% without
HOW ILM IS PEELED (surgical anatomy):
1. Indocyanine green (ICG) or Brilliant Blue staining → makes
transparent ILM visible (selective affinity for ILM)
2. Microforceps grasp ILM edge away from hole
3. Peeled circumferentially around hole (1.5-2 disc diameter)
4. ILM removed in one piece ideally
RISK OF ILM PEEL:
- Ganglion cell axons can be damaged (NFL is just inner to ILM)
- Dissociated optic nerve fiber layer (DONFL) appearance on OCT
(dimple artifacts) - usually asymptomatic
2.3 - Tamponade Agents - Anatomy Determines Which to Use
VITREOUS TAMPONADE AGENTS - ANATOMY OF ACTION
The concept: After vitrectomy + retinal reattachment,
a TAMPONADE keeps the retina pressed against RPE while
the laser/cryo chorioretinal adhesion forms (2-6 weeks)
GAS TAMPONADE (SF6, C3F8, Air):
Behaviour: BUOYANT - floats upward
Therefore: Patient must POSTURE (face-down usually)
to bring gas bubble over the retinal break
┌──────────────────────────────────────────────────────┐
│ BREAK LOCATION → POSTURE NEEDED: │
│ Superior break → face-down (gas floats up = covers) │
│ Inferior break → face-up (can't use gas alone) │
│ Temporal break → tilt head left (if right eye) │
└──────────────────────────────────────────────────────┘
GAS EXPANSION:
Air: No expansion, absorbed in 5-7 days
SF6 (20%): Expands ×2, lasts 6-8 weeks
C3F8 (14%): Expands ×4, lasts 2-3 months
WARNING: Flying at altitude or N2O anaesthesia →
gas expands → acute angle closure glaucoma!
(Patient must carry warning card)
SILICONE OIL TAMPONADE:
Behaviour: BUOYANT (lighter than water) - floats UP
Also acts on: INFERIOR breaks (patient posture = face-up)
Duration: Indefinite (needs surgical removal 3-6 months)
Used when: PVR (proliferative vitreoretinopathy), inferior
breaks, non-compliant patients, fellow eye
Complications from anatomy:
1. OIL IN ANTERIOR CHAMBER → emulsification → trabecular
blockage → glaucoma (oil droplets clog the TM)
2. CATARACT: Silicone oil contacts posterior lens capsule
→ PSC (posterior subcapsular cataract)
3. BAND KERATOPATHY: Oil emulsifies → droplets in cornea
4. In APHAKIC eye: Oil goes through pupil → directly
contacts corneal endothelium → endothelial failure
(Keyhole PI needed in inferior iris to prevent this)
SECTION 3: SURGICAL ANATOMY OF THE DRAINAGE ANGLE
3.1 - Trabeculectomy - Anatomy of Every Step
TRABECULECTOMY = gold standard glaucoma surgery
STEP-BY-STEP ANATOMY:
Step 1: SUPERIOR CONJUNCTIVAL PERITOMY
Why superior? → Postoperative bleb forms under
upper eyelid → protected from trauma, drying, infection
Conjunctiva cut at limbus → Tenon's capsule exposed
Tenon's = fascial layer over sclera → must be separated
from underlying sclera carefully
Step 2: HEMOSTASIS + ANTIMETABOLITE APPLICATION
Mitomycin C (MMC) or 5-Fluorouracil (5-FU) applied
on wet surgical sponges to SCLERA and TENON'S
→ Inhibits fibroblast proliferation (Tenon's fibroblasts
= main cause of bleb scarring/failure)
Washed off thoroughly → antimetabolites are cytotoxic
to corneal epithelium, endothelium if contact
Step 3: PARTIAL-THICKNESS SCLERAL FLAP
┌────────────────────────────────────────────────────┐
│ Cut 3-4 mm scleral flap, half-thickness (~0.3 mm) │
│ WHY half-thickness? Full thickness = too weak, │
│ hole in sclera uncontrolled; half = flap acts as │
│ resistance to aqueous flow (controls IOP) │
│ │
│ Flap size: 3mm × 3mm (square) or 4mm × 3mm │
│ Location: 1-2 mm posterior to limbus │
│ │
│ WHY LIMBUS LOCATION: │
│ Must reach Schlemm's canal and trabecular meshwork │
│ (which are AT the limbus) │
└────────────────────────────────────────────────────┘
Step 4: SCLERECTOMY (OSTIUM CREATION)
Remove small block of deep sclera + TM + Schlemm's canal
under the scleral flap
→ Creates FISTULA from AC → subconjunctival space
KELLY PUNCH or VANNAS scissors used
Punch sites: At Schwalbe's line anteriorly +
Scleral spur posteriorly
Includes: Full-thickness sclera + corneoscleral TM
Step 5: PERIPHERAL IRIDECTOMY (PI)
WHY MANDATORY?
→ Prevents iris from blocking the internal ostium
→ Without PI: Iris can plug the hole → drainage fails
→ Also prevents pupillary block (if AC shallows)
Location: Peripheral iris, away from visual axis
Method: Iris grasped and cut (Vannas scissors)
Result: Small full-thickness hole in iris
Step 6: SCLERAL FLAP CLOSURE
Flap sutured loosely (2-4 releasable sutures)
WHY LOOSELY? Suture tension controls IOP:
Tight sutures = more resistance = higher IOP
Loose sutures = less resistance = lower IOP (hypotony risk)
RELEASABLE SUTURES: Can be removed in clinic
(slit-lamp procedure) to increase flow if IOP rises
LASER SUTURE LYSIS (Hoskins lens):
Argon laser burns through nylon suture through conjunctiva
→ Increases bleb flow → lowers IOP postoperatively
Step 7: CONJUNCTIVAL CLOSURE
Watertight closure essential
Running or mattress sutures at limbus
POSTOPERATIVE BLEB ANATOMY:
Aqueous flows: AC → ostium → under scleral flap →
under Tenon's → under conjunctiva → BLEB forms
Bleb: Translucent, avascular, elevated collection
of aqueous under conjunctiva
Good bleb: Diffuse, low, avascular, mobile
Bad bleb: Encapsulated (Tenon's cyst), vascular, flat
3.2 - Goniotomy vs Trabeculotomy (Congenital Glaucoma)
CONGENITAL GLAUCOMA - SURGICAL ANATOMY:
Problem: Failure of neural crest cell migration →
trabecular meshwork fails to develop properly
→ Barkan's membrane (abnormal tissue over TM)
→ ↑ resistance → ↑ IOP
GONIOTOMY:
┌─────────────────────────────────────────────────────┐
│ INTERNAL approach (from inside AC) │
│ Goniotomy knife entered through clear cornea │
│ Under gonioscopic guidance → knife cuts across │
│ angle from inside → incises Barkan's membrane │
│ → Opens TM from inside │
│ │
│ Requires: Clear cornea (to see angle) │
│ Best for: Primary congenital glaucoma (clear cornea)│
└─────────────────────────────────────────────────────┘
TRABECULOTOMY:
┌─────────────────────────────────────────────────────┐
│ EXTERNAL approach (from outside eye) │
│ Scleral flap raised at limbus │
│ Schlemm's canal identified (intrascleral canal) │
│ Trabeculotome probe passed INTO Schlemm's canal │
│ Rotated internally → RUPTURES TM from outside-in │
│ │
│ Requires: Locating Schlemm's canal (technical) │
│ Best for: Cloudy cornea (cannot do goniotomy) │
└─────────────────────────────────────────────────────┘
COMBINED TRABECULOTOMY-TRABECULECTOMY:
Best for severe cases → opens TM + creates fistula
3.3 - MIGS - Which Layer of TM They Target
MINIMALLY INVASIVE GLAUCOMA SURGERY (MIGS)
All designed to bypass the JUXTACANALICULAR MESHWORK
(= site of maximum resistance = highest IOP impact)
┌────────────────────────────────────────────────────────┐
│ SCHLEMM'S CANAL BASED (Ab interno): │
│ │
│ iStent Inject W: │
│ Tiny titanium stent placed through TM into Schlemm's │
│ Bypasses all 3 TM layers → direct AC→canal drainage │
│ 2 stents placed (at 120°/180° apart) │
│ │
│ Hydrus Microstent: │
│ Scaffold placed INTO Schlemm's canal (8 mm length) │
│ Dilates canal + bypasses TM + opens multiple │
│ collector channels │
│ │
│ Gonioscopy-Assisted Transluminal Trabeculotomy (GATT): │
│ Suture threaded 360° around Schlemm's canal │
│ Pulled through → unroofs entire canal │
├────────────────────────────────────────────────────────┤
│ SUPRACHOROIDAL SPACE BASED: │
│ │
│ iStent Supra / CyPass (now withdrawn): │
│ Stent placed through ciliary body into │
│ suprachoroidal space → uveoscleral outflow enhanced │
├────────────────────────────────────────────────────────┤
│ SUBCONJUNCTIVAL SPACE BASED: │
│ │
│ XEN Gel Stent / PRESERFLO: │
│ Tiny tube creates fistula from AC to subconj space │
│ Similar to trabeculectomy but less invasive │
│ No scleral flap, smaller bleb, less hypotony risk │
└────────────────────────────────────────────────────────┘
SECTION 4: CLINICO-ANATOMICAL CORRELATIONS
The "Why" Questions - Viva Gold
Q1: Why is corneal abrasion so painful but retinal detachment is painless?
CORNEAL ABRASION - PAINFUL:
Cornea = most densely innervated tissue in body
Sub-epithelial nerve plexus + intraepithelial free endings
(density: 7000 nociceptors/mm² → 300-600x denser than skin)
Epithelium lost → free nerve endings directly exposed
→ INTENSE pain, photophobia, reflex lacrimation, blepharospasm
RETINAL DETACHMENT - PAINLESS:
Retina has NO sensory pain fibers
(only contains specialized photoreceptors for light)
Sensory innervation of eye:
→ Cornea/iris/ciliary body = CN V1 (pain)
→ Retina = NONE
Detachment causes visual loss (curtain/shadow) but NO PAIN
Patient describes it as "a curtain coming down" or "shadow"
NOT as pain
Exception: If RD causes secondary uveitis/high IOP → can get some ache
Q2: Why does raised ICP cause papilledema?
RAISED ICP → PAPILLEDEMA - ANATOMY EXPLAINED:
The optic nerve is an OUTGROWTH OF THE BRAIN
→ It is surrounded by THREE MENINGEAL SHEATHS
(dura mater, arachnoid, pia mater)
→ The SUBARACHNOID SPACE around the optic nerve is
CONTINUOUS with the intracranial subarachnoid space
Normal: CSF pressure = same around brain and around optic nerve
Raised ICP:
↑ CSF pressure → transmitted along subarachnoid space
→ surrounds optic nerve → raised pressure around nerve
EFFECT ON AXONAL TRANSPORT:
Raised pressure → compresses axons in optic nerve
→ Blocks AXOPLASMIC FLOW (anterograde transport)
→ Axon contents accumulate at optic disc
→ DISC OEDEMA / SWELLING = PAPILLEDEMA
WHY BILATERAL:
Both optic nerves connect to same subarachnoid space
→ Both affected simultaneously → BILATERAL papilledema
WHY VISION INITIALLY PRESERVED:
Early papilledema = oedema only (no axonal loss yet)
Visual field: Enlarged blind spot (first sign)
Later: Constriction, arcuate defects (axons dying)
Late: Vision loss (irreversible axonal damage)
ANATOMICAL DIFFERENCE FROM OPTIC NEURITIS:
Papilledema = bilateral, ICP cause, vision initially preserved
Optic neuritis = usually unilateral, RAPD present, VA drops early
Q3: Why does glaucoma damage the inferior arcuate fibers first?
INFERIOR ARCUATE NERVE FIBERS - ANATOMICAL VULNERABILITY:
WHERE ARE THEY:
Retinal nerve fibers below the horizontal meridian
Arc from temporal retina → curve around macula →
enter INFERIOR POLE of optic disc
WHY THEY ARE DAMAGED FIRST IN GLAUCOMA:
BLOOD SUPPLY FACTOR:
Inferior optic disc = supplied by inferior division of SPCA
These vessels have LESS AUTOREGULATION capacity
→ More vulnerable to IOP-mediated ischaemia
STRUCTURAL FACTOR:
Inferior and superior poles of disc have:
- Thinnest lamina cribrosa plates (fewer plates, larger pores)
- Axon bundles have LESS CONNECTIVE TISSUE support
→ Same IOP → MORE DEFORMATION of lamina at poles
→ INFERIOR POLE: slightly more vulnerable than superior
NFL ANATOMY:
Inferior arcuate bundle (Bjerrum area) = densely packed
→ One ganglion cell axon per fiber bundle at macula
→ Any injury = proportionally larger field defect
RESULT:
Superior visual field defect first (inferior retina damaged)
= Nasal step or superior arcuate scotoma (Bjerrum scotoma)
Progresses → ring scotoma → tunnel vision → total blindness
ON OCT:
RNFL thinning at INFERIOR DISC POLE first (6 o'clock)
Then superior (12 o'clock)
Nasal and temporal NFL preserved longest
(matches the ISNT rule - temporal = thinnest anyway)
Q4: Why does PSC (posterior subcapsular cataract) cause disproportionate glare in bright light?
PSC IN BRIGHT LIGHT - ANATOMY EXPLAINED:
Location of PSC: Posterior capsule (just inside the posterior pole
of the lens, near the visual axis)
In DIM LIGHT:
Pupil DILATES (mydriasis)
→ Large pupil → light enters through PERIPHERAL lens
→ Bypasses the central PSC opacity
→ Vision relatively preserved (less glare)
In BRIGHT LIGHT:
Pupil CONSTRICTS (miosis - to reduce light)
→ Small pupil (2-3 mm) → only central rays enter
→ ALL light must pass through the PSC opacity
→ Maximal scattering → severe glare, blur
RESULT: "Worse vision in bright light" = PATHOGNOMONIC of PSC
Clinical test: Check VA in bright room vs dim room
PSC: Bright room = much worse
Nuclear cataract: Dim room = worse (increased spherical aberration
with dilation), better in bright room with miosis
WHY PSC FORMS (epithelial migration):
In DM: sorbitol pathway → osmotic damage to epithelium
In steroids: Anterior epithelial cells migrate posteriorly
In trauma: Direct injury to equatorial germinating zone
In radiation: Posterior epithelial damage
Q5: Why does macular disease cause central scotoma but peripheral retinal disease causes peripheral field loss?
RETINOTOPIC MAPPING - ANATOMY OF VISUAL FIELD LOSS:
FOVEA (central 5°):
= Site of highest cone density (one cone : one ganglion cell)
= Direct, undistorted representation of central vision
= Foveal damage → CENTRAL SCOTOMA (loss of detailed vision,
reading, recognizing faces)
Example: AMD, macular hole, CSC, Stargardt
MACULA (central 20-30°):
= Dense cone and ganglion cell representation
= Lesions here → centrocecal or paracentral scotoma
Example: Optic neuritis (centrocecal scotoma)
PERIPHERAL RETINA:
= Rod-dominant, lower spatial resolution
= Many rods share one ganglion cell (convergence)
= Lesions → peripheral field defects
Example: Retinitis pigmentosa → ring scotoma → tunnel vision
ANATOMICAL PRINCIPLE: CORTICAL MAGNIFICATION
Central visual field → disproportionately large representation
in visual cortex (approximately 50% of visual cortex for
central 10°)
→ Means central retinal damage is noticed MUCH EARLIER
than equivalent peripheral damage
CLINICAL CONSEQUENCE:
Patient with large peripheral RD may present late
(peripheral field loss not noticed in monocular RD)
Patient with small macular disease noticed immediately
(central vision affected → severe functional impact)
Q6: Why does chemical injury cause limbal ischaemia and poor prognosis?
LIMBAL ISCHAEMIA IN CHEMICAL INJURY:
WHY LIMBUS IS THE CRITICAL ZONE:
Limbal blood vessels supply:
1. Limbal stem cells (LSCs) at palisades of Vogt
2. Peripheral corneal epithelial renewal
Alkali burns (NaOH, KOH, Ca(OH)2, NH3):
- PENETRATE DEEP (saponify cell membranes)
- Alkali → continues to penetrate until neutralized
- Damages limbal vasculature + LSCs directly
WHITENING OF LIMBUS = BAD PROGNOSTIC SIGN:
White/ischaemic limbus = blood vessels thrombosed
= LSCs destroyed
= No corneal epithelial regeneration possible
→ Conjunctivalization, corneal vascularization,
persistent epithelial defects, corneal melting
ROPER-HALL CLASSIFICATION (grading):
Grade I : Corneal haze only, no limbal ischaemia → excellent
Grade II : Haze + <⅓ limbal ischaemia → good prognosis
Grade III : Total corneal opacity + ½ limbal ischaemia → guarded
Grade IV : Opaque cornea + >½ limbal ischaemia → poor
TREATMENT LOGIC (applied anatomy):
Irrigation → remove alkali → stop penetration
Limbal stem cell transplantation (LSCT) → restore corneal epithelium
(Auto: from fellow eye; Allo: cadaveric/living donor)
Q7: Why does vitreous haemorrhage cause sudden painless vision loss?
VITREOUS HAEMORRHAGE - ANATOMICAL PATH OF VISION LOSS:
Normal vitreous: Clear gel, 99% water → transparent → no scatter
Haemorrhage source:
→ Retinal new vessels (PDR) bleed into vitreous cavity
→ Torn retinal vessel bleeds
→ Posterior vitreous detachment ruptures a bridging vessel
Blood in vitreous:
→ RBCs scatter ALL incident light
→ No focused image reaches retina
→ Painless (vitreous has no pain receptors)
→ Sudden (can develop overnight - patient wakes with symptoms)
Symptoms:
- Red haze (if mild) → "looking through red cellophane"
- Dark floaters
- Complete loss of red reflex (dense haemorrhage)
- Vision 6/60 → LP (depending on density)
Why no pain?
Vitreous = avascular, no nerves
Blood itself has no nociceptive effect
(Compare: Uveitis is painful because iris/ciliary body innervated)
Why eventually clears?
Vitreous has some phagocytic activity (hyalocytes)
RBCs lyse → haemoglobin absorbed
Average: 3-6 months for spontaneous absorption
When to do PPV immediately?
1. Can't see retina (unknown cause → may be RD)
2. B-scan shows retinal detachment under haemorrhage
3. Type 2 diabetes (high-risk PDR)
4. Dense haemorrhage in only-functioning eye
APPLIED ANATOMY QUICK-FIRE SUMMARY TABLE ★★★
| "Why" Question | Anatomical Answer |
|---|---|
| Why is cornea avascular? | Transparency requires no haemoglobin; O2 from tears + aqueous |
| Why does corneal abrasion hurt so much? | Densest nociceptive innervation in body (7000/mm²) |
| Why is RD painless? | Retina has no sensory pain fibers (only photoreceptors) |
| Why is raised ICP bilateral papilledema? | Subarachnoid space of optic nerve = continuous with intracranial CSF |
| Why does glaucoma damage inferior fibers first? | Inferior lamina = thinnest plates + inferior SPCA = less autoregulation |
| Why does PSC = glare in bright light? | Pupil constricts → ALL light passes through central opacity |
| Why does macular disease cause central scotoma? | Fovea = only photoreceptors in center, highest cone density |
| Why is alkaline burn worse than acid? | Alkali penetrates (saponification) vs acid coagulates (self-limiting) |
| Why is limbal ischaemia a bad prognostic sign? | Destroys limbal stem cells → no corneal epithelial renewal |
| Why does vitreous haemorrhage cause sudden painless loss? | Blood scatters light, vitreous has no pain receptors |
| Why must PC rupture be managed immediately? | Vitreous prolapse → retinal traction → RD risk |
| Why is IOL not suitable in sulcus for toric/multifocal? | Sulcus position = unstable rotation → defeats the purpose |
| Why does silicone oil cause cataract? | Contacts posterior lens capsule → PSC formation |
| Why does angle-supported ACIOL cause endothelial loss? | Proximity to corneal endothelium → mechanical + toxic damage |
| Why does YAG capsulotomy increase RD risk? | Vitreous moves forward → traction on peripheral retina |
| Why is pars plana the safe entry zone for vitrectomy? | No lens fibers, no ciliary processes, retina starts at ora serrata |
| Why is scleral tunnel more watertight than clear corneal? | Scleral collagen swells when wet → self-sealing |
| Why does orbital optic nerve have a tortuous course? | Allows full range of eye movement without stretching |
| Why is goniotomy not possible in cloudy cornea? | Cannot visualize angle gonioscopically |
| Why does gas expand at altitude? | Boyle's law: ↓ atmospheric pressure → gas expands → acute angle closure |
- Part 1 = Structural anatomy of all layers with histology images
- Part 2 = Embryology + Limbus/TM + Optic nerve head
- Part 3 = Applied and surgical anatomy - every "why" answered
ANY PHARMAVOLOGICAL BASIS?
What Pharmacological Basis IS Already in the Notes
- Pilocarpine → mimics parasympathetic → sphincter pupillae → miosis
- Tropicamide/Atropine → blocks muscarinic → mydriasis
- Phenylephrine → stimulates sympathetic → dilator → mydriasis
- Cocaine → blocks noradrenaline reuptake → mydriasis
- Prostaglandins → increase uveoscleral outflow
- Beta-blockers → decrease aqueous production (Na/K ATPase inhibition)
- CAIs → decrease aqueous production (carbonic anhydrase inhibition)
- Alpha-2 agonists → decrease production + increase uveoscleral
- Pilocarpine → contracts ciliary muscle → reduces uveoscleral outflow
- MMC/5-FU → inhibit fibroblast proliferation (trabeculectomy)
- Apraclonidine → pre-YAG capsulotomy for IOP spike prevention
- ICG/Brilliant Blue → stain ILM for peeling
- BSS → hydrodissection
What Is COMPLETELY MISSING - Dedicated Pharmacology Section
1. Corneal Pharmacology
- Drug penetration routes (transcorneal vs non-corneal)
- Why lipophilic drugs penetrate cornea better
- Why some drugs penetrate even better at limbus (blood vessels)
- Role of preservatives (BAC - benzalkonium chloride) and their toxicity to corneal epithelium + TM
- Topical anaesthetics mechanism (proxymetacaine, oxybuprocaine) → sodium channel blockade → why don't use repeatedly (epithelial toxicity, loss of protective blink reflex)
- Fluorescein staining → stains DISRUPTED epithelium (breaks in tight junctions) → not cells themselves
2. Pupillary Pharmacology (Complete)
- Full receptor pharmacology (muscarinic M3, alpha-1 adrenergic)
- Pharmacological localisation of Horner syndrome (cocaine test, apraclonidine, hydroxyamphetamine)
- Adie's pupil (denervation supersensitivity → dilute pilocarpine 0.1% constricts)
- Argyll Robertson pupil mechanism
- Pharmacological mydriasis vs physiological mydriasis (how to distinguish)
3. Retinal/Intravitreal Pharmacology
- Anti-VEGF: mechanism at receptor level (VEGF-A binds VEGFR-1/2 → downstream signalling → angiogenesis/permeability)
- Why intravitreal route? Systemic delivery poor penetration into eye (blood-retinal barrier)
- Corticosteroid implants (Ozurdex = dexamethasone biodegradable implant in vitreous)
- Photodynamic therapy (PDT) - verteporfin mechanism
4. Glaucoma Pharmacology (Receptor-Level)
- Exact receptor for each drug class
- Carbonic anhydrase isoforms in ciliary body (CA-II, CA-IV)
- Rho-kinase inhibitors (netarsudil) - new mechanism
- Prostaglandin receptor subtypes (FP receptor)
5. Antibiotic Pharmacology for Endophthalmitis
- Why intravitreal vancomycin + ceftazidime? (gram +ve / gram -ve coverage)
- Minimum inhibitory concentrations vs intravitreal levels
- Why intravitreal - blood-ocular barrier prevents systemic antibiotics reaching vitreous
My Honest Verdict
- Mechanism of action at receptor level (written paper)
- Clinical pharmacology - dosing, side effects, contraindications (viva)
- Applied pharmacology - which drug for which situation and why (clinical)
What I Recommend
I WOULD LIKE TO STUDY AS OPTION B BUT NOW Add corneal and pupil pharmacology
WEEK 1 EYEBALL ANATOMY - PART 4
Pharmacological Basis: Corneal Pharmacology + Pupil Pharmacology
SECTION 1: CORNEAL PHARMACOLOGY
1.1 - How Drugs Get Into the Eye (Ocular Pharmacokinetics)
Drug Absorption Pathway Diagram
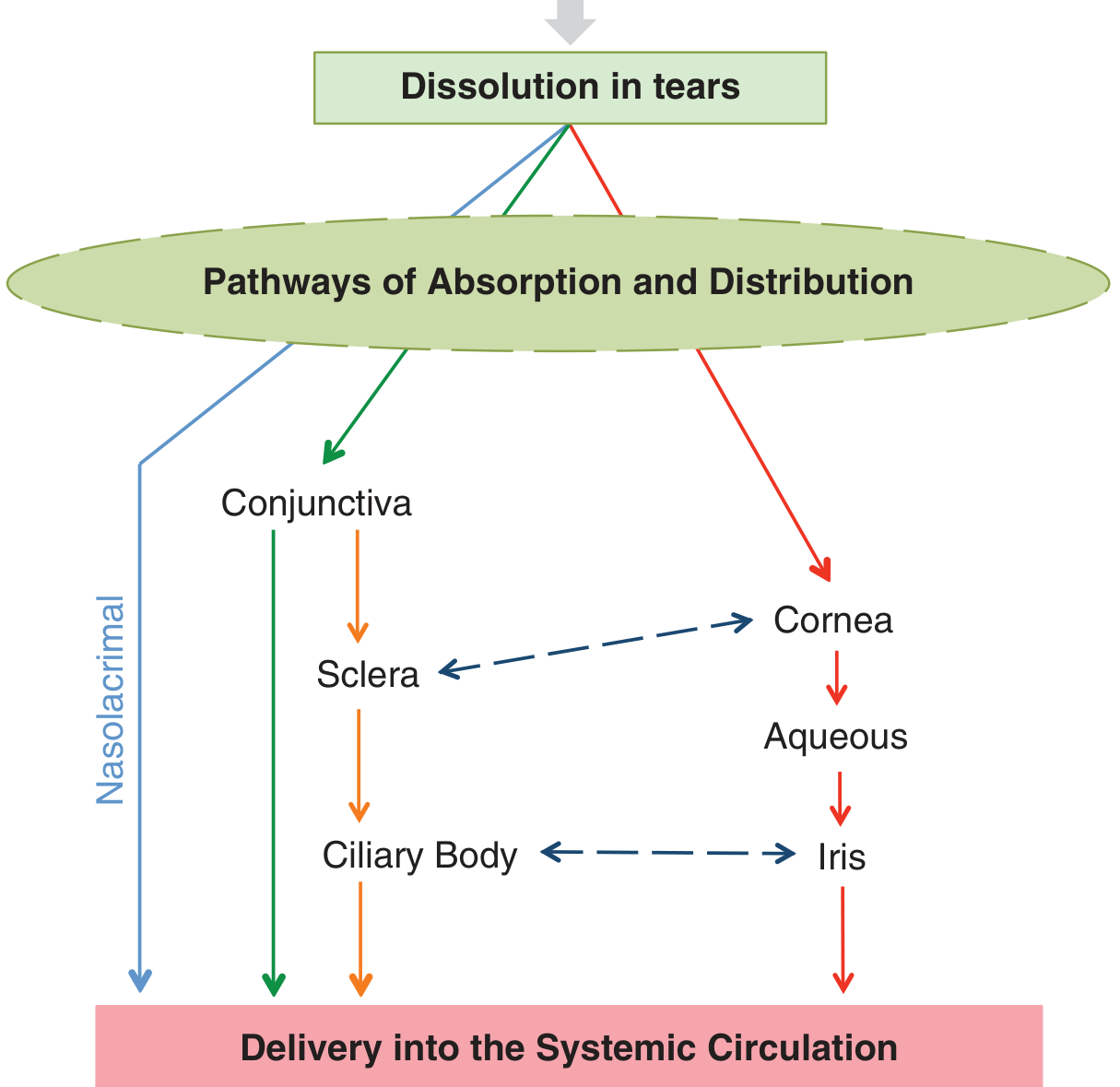
The Fate of a Topical Eye Drop - Full Flowchart
EYE DROP INSTILLED (typically 30-50 µL)
│
│ [Conjunctival sac holds only 7-10 µL]
│ → OVERFLOW immediately → cheek/skin
│
▼
Tear film (7-10 µL volume)
│
┌──────┼──────────────────────────────┐
│ │ │
▼ ▼ ▼
NASOLACRIMAL CONJUNCTIVA CORNEAL ROUTE
DRAINAGE (non-target) (TARGET route)
│ │ │
▼ ▼ ▼
Nasal mucosa Subconj space Aqueous humor
→ systemic → sclera → iris, ciliary body,
absorption → ciliary body lens, vitreous
(NO 1st (bypasses cornea) (intended effect)
pass liver)
│
▼
SYSTEMIC SIDE EFFECTS
(timolol → bradycardia, bronchospasm;
atropine → tachycardia, dry mouth;
pilocarpine → sweating, nausea)
★ NASOLACRIMAL ABSORPTION = main cause of systemic SE
★ Prevention: PUNCTAL OCCLUSION (press inner canthus
for 2 minutes after drop) → blocks drainage
→ keeps drug in eye longer + reduces systemic absorption
1.2 - The Cornea as a Drug Barrier - "Fat-Water-Fat" Model
CORNEAL STRUCTURE AS A PHARMACOKINETIC BARRIER:
Layer Nature Barrier to
─────────────────────────────────────────────────
Epithelium LIPOPHILIC Hydrophilic (water-soluble) drugs
(tight junctions Cannot pass through lipid bilayer
+ lipid cell membrane easily
membranes)
Stroma HYDROPHILIC Hydrophobic (lipid-soluble) drugs
(90% water, Cannot dissolve and diffuse through
collagen, GAGs) watery stroma easily
Endothelium LIPOPHILIC Hydrophilic drugs (again)
(cell membranes)
RESULT - "FAT-WATER-FAT" BARRIER:
Pure hydrophilic drug → blocked at epithelium
Pure lipophilic drug → passes epithelium but blocked by stroma
AMPHIPATHIC drug → passes ALL THREE LAYERS
(both hydrophilic AND lipophilic properties)
→ IDEAL OPHTHALMIC DRUG = AMPHIPATHIC
Drug Examples Classified by Penetration:
GOOD PENETRATION (amphipathic):
Chloramphenicol → small, amphipathic → excellent corneal penetration
→ achieves good AC levels
Fluoroquinolones → ciprofloxacin, moxifloxacin → amphipathic
→ good penetration into aqueous
Prednisolone → amphipathic steroid → good anterior segment penetration
Pilocarpine → amphipathic → good corneal penetration
POOR PENETRATION (too hydrophilic):
Gentamicin → hydrophilic aminoglycoside → poor corneal penetration
→ stays in stroma → good for keratitis,
poor for AC/endophthalmitis
POOR PENETRATION (too lipophilic):
Some antifungals → natamycin is very hydrophilic → poor stromal penetration
→ stays superficial → why only works for superficial fungal keratitis
→ voriconazole more amphipathic → penetrates deeper
PRODRUG STRATEGY (latanoprost example):
Latanoprost = ISOPROPYL ESTER PRODRUG of PGF2α
→ Highly lipophilic (ester group) → easily crosses lipophilic epithelium
→ Corneal esterases cleave ester → releases FREE PGF2α ACID (active form)
→ Free acid is hydrophilic → distributes in aqueous
→ This is how an active molecule crosses the "fat-water-fat" barrier
Loteprednol etabonate = similar strategy
→ Prednisolone prodrug with ester → low IOP rise risk
→ Metabolised within eye → inactive metabolite → minimal systemic effect
1.3 - Factors That Alter Corneal Drug Penetration
FACTORS INCREASING DRUG PENETRATION:
1. EPITHELIAL DEFECT (corneal ulcer, trauma, abrasion)
→ Removes the lipophilic epithelial barrier
→ Hydrophilic drugs suddenly penetrate much better
→ CLINICAL: Use fortified antibiotics (concentrated) in
bacterial keratitis - penetrate through defect
2. CONTACT LENSES
→ Act as drug reservoir (soak up drug → slow release)
→ Remove lenses before instilling most drops
→ Exception: Drug-eluting contact lenses (research)
3. PRESERVATIVE-FREE FORMULATIONS
→ Benzalkonium chloride (BAC) disrupts epithelial tight junctions
→ Paradoxically INCREASES penetration of some drugs
→ But at cost of epithelial toxicity (see below)
4. VEHICLE / FORMULATION:
→ Gel formulations (carbomer gel) → longer contact time
→ Ointments → longer dwell time, higher peak levels
→ Liposomes, nanoparticles → drug delivery research
5. pH ADJUSTMENT:
→ Most drugs are weak bases
→ pH affects ionization (Henderson-Hasselbalch)
→ Unionized (lipophilic) form crosses membranes
→ Aqueous tears (pH 7.4) → must formulate near this
FACTORS DECREASING DRUG PENETRATION:
1. RAPID BLINKING → wipes drug off surface → lost
2. NASOLACRIMAL DRAINAGE → drug leaves eye quickly
3. DILUTION by reflex tearing (pain/irritation from drop)
4. MELANIN BINDING (darkly pigmented irides)
→ Alpha-agonists bind to iris melanin
→ Mydriatic response SLOWER in brown irides than blue
→ Drug reservoir → sustained release can cause prolonged action
5. BLOOD-OCULAR BARRIERS (posterior segment penetration poor)
1.4 - Preservatives in Eye Drops - The Double-Edged Sword
BENZALKONIUM CHLORIDE (BAC / BAK)
Most common preservative in ophthalmic preparations
Concentration: 0.004% - 0.02% in most drops
Mechanism of preservation: Cationic detergent → disrupts bacterial
cell membranes → bactericidal/bacteriostatic
OCULAR TOXICITY (dose and frequency dependent):
CORNEAL EPITHELIUM:
BAC → Disrupts epithelial tight junctions
→ Increases membrane permeability (disrupts lipid bilayer)
→ At low conc (0.004%): increases drug penetration (useful)
→ At high conc or chronic use:
├── Punctate epithelial erosions (PEE) → slit lamp: tiny dots
├── Toxic ulcerative keratopathy (TUK) → larger epithelial loss
└── Reduced goblet cells → worsens dry eye
TRABECULAR MESHWORK:
BAC → TM endothelial cell toxicity
→ Increased TM cell apoptosis
→ Long-term use of preserved glaucoma drops → ↑ TM fibrosis
→ WORSE outcomes at trabeculectomy (conjunctival scarring)
CLINICAL RELEVANCE:
→ Patients on multiple preserved glaucoma drops chronically
→ Consider preservative-free (PF) formulations
→ Pre-trabeculectomy: Switch to PF drops at least 1-3 months prior
→ Dry eye patients: PF artificial tears mandatory
OTHER PRESERVATIVES:
Chlorobutanol: Less toxic than BAC, used in some mydriatics
SofZia (borate/sorbitol/zinc): "Disappearing" preservative
→ converts to harmless components on contact with eye
Purite (oxychloro complex): Similar "vanishing" action
→ Used in Alphagan P (brimonidine PF formulation)
Thimerosal: Mercury-based → largely abandoned (allergy, toxicity)
1.5 - Diagnostic Dyes - Pharmacological Basis
THREE VITAL CORNEAL STAINS - KNOW THE MECHANISM:
┌─────────────────────────────────────────────────────────────┐
│ FLUORESCEIN SODIUM │
│ Colour: Orange dye → fluoresces GREEN under cobalt blue light│
│ │
│ Mechanism: │
│ Normally: Tight junctions of corneal epithelium EXCLUDE │
│ fluorescein (high molecular weight, hydrophilic) │
│ │
│ When epithelium DAMAGED: │
│ Tight junctions disrupted → fluorescein ENTERS the tissue │
│ → Green staining under cobalt blue light │
│ │
│ What it stains: EPITHELIAL DEFECTS (abrasions, ulcers, │
│ dendritic ulcers in HSV, PEE in dry eye/BAC toxicity) │
│ │
│ Other uses: │
│ - Goldmann applanation tonometry (tears stained to measure) │
│ - Fluorescein angiography (IV injection → retinal vessels) │
│ - Seidel test: aqueous leak → dilutes fluorescein → green │
│ stream from wound │
│ - TFBUT: Time for tear film to break up (normal >10 sec) │
│ │
│ DOES NOT stain: Intact cells, mucus, vitreous │
└─────────────────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────────────────┐
│ ROSE BENGAL (1%) │
│ Colour: Red-pink stain │
│ │
│ Mechanism: │
│ Stains DEVITALIZED (dead/dying) epithelial cells │
│ that have lost their protective MUCIN COAT │
│ (Normally, mucin glycoproteins protect cells from staining)│
│ │
│ What it stains: │
│ - Dead epithelial cells (mucin-stripped) │
│ - Filaments and plaques │
│ - Superior limbal conjunctiva in SLK │
│ - Interpalpebral zone in dry eye (KCS) │
│ │
│ Problem: PAINFUL! → sting intensely in dry eye patients │
│ Solution: Give topical anaesthetic first + flush with saline│
│ Kanski tip: "Very small drop to minimize irritation" │
└─────────────────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────────────────┐
│ LISSAMINE GREEN (1%) │
│ Colour: Green stain │
│ │
│ Mechanism: Similar to Rose Bengal │
│ Stains dead/devitalized cells with lost mucin coat │
│ │
│ ADVANTAGE over Rose Bengal: │
│ - Less irritating (does NOT cause intense stinging) │
│ - Preferred for patients with severe dry eye │
│ Kanski: "Lissamine green preferable to 1% rose Bengal │
│ as it stains in similar fashion but causes less irritation" │
└─────────────────────────────────────────────────────────────┘
COMPARISON TABLE:
┌──────────────┬────────────────────────┬──────────────────────┐
│ Dye │ What it stains │ Key use │
├──────────────┼────────────────────────┼──────────────────────┤
│ Fluorescein │ Epithelial DEFECTS │ Ulcers, abrasions, │
│ │ (dead cells excluded, │ HSV dendrites, TBF, │
│ │ gaps in epithelium) │ tonometry, Seidel │
├──────────────┼────────────────────────┼──────────────────────┤
│ Rose Bengal │ DEVITALIZED cells │ KCS, SLK, viral │
│ │ (dead cells + mucin │ epitheliopathy │
│ │ stripped cells) │ (painful!) │
├──────────────┼────────────────────────┼──────────────────────┤
│ Lissamine │ DEVITALIZED cells │ KCS (preferred - │
│ Green │ (same as rose bengal) │ less irritating) │
└──────────────┴────────────────────────┴──────────────────────┘
★ EXAM DISTINCTION: Fluorescein stains WHERE cells are ABSENT
Rose Bengal/Lissamine stain WHERE cells are PRESENT but DEAD
1.6 - Topical Anaesthetics - Mechanism and Dangers
TOPICAL OPHTHALMIC ANAESTHETICS
Agents:
Proxymetacaine (Proparacaine) 0.5% → drug of choice
Oxybuprocaine (Benoxinate) 0.4%
Tetracaine (Amethocaine) 0.5-1% → most potent, most toxic
Cocaine 4-10% → only anaesthetic also causes vasoconstriction
+ mydriasis (still used in ENT, rarely ophthal)
Lignocaine (Lidocaine) 4% → intracameral (cataract surgery)
MECHANISM OF ALL LOCAL ANAESTHETICS:
All = SODIUM CHANNEL BLOCKERS (reversible)
Normal corneal sensation:
Free nerve endings in epithelium
→ Action potential propagated by Na+ influx through voltage-gated
Na+ channels
→ Travels along trigeminal (V1) → trigeminal nucleus → thalamus → cortex
LA mechanism:
Drug (ionized + unionized form) →
Unionized (lipophilic) form crosses axon membrane
→ Re-ionizes inside axon
→ Ionized form BLOCKS Na+ channel from INSIDE (pore blockade)
→ No Na+ influx → no depolarization → no action potential
→ ANAESTHESIA
Onset: 10-20 seconds (cornea very thin → fast penetration)
Duration: 10-20 minutes (proxymetacaine), 30 min (tetracaine)
WHY TOPICAL ANAESTHETICS ARE DANGEROUS IF OVERUSED:
1. CORNEAL EPITHELIAL TOXICITY:
→ Na+ channels also important for normal cell function
→ Prolonged blockade → mitotic arrest in basal cells
→ Impairs epithelial healing (no migration, no proliferation)
→ Paradoxically: CAUSES large epithelial defects
→ "Anaesthetic abuse keratopathy" - seen in Munchausen syndrome
or patients who self-medicate for chronic eye pain
2. LOSS OF PROTECTIVE BLINK REFLEX:
→ Cornea no longer sensitive
→ Patient doesn't blink to protect eye
→ Foreign bodies, drying, rubbing → damage accumulates
→ NEVER give topical anaesthetic to take home
→ Only use in-clinic under supervision
3. CONJUNCTIVITIS AND ALLERGY:
→ Especially tetracaine → high rate of hypersensitivity
→ Proxymetacaine = least allergenic → drug of choice
COCAINE SPECIFICALLY:
Additional effects beyond Na+ channel blockade:
→ Blocks NORADRENALINE REUPTAKE → ↑ sympathetic tone
→ Causes: MYDRIASIS (via dilator pupillae)
VASOCONSTRICTION (blanching of conjunctiva)
Use in Horner syndrome test (see pupil pharmacology below)
SECTION 2: PUPIL PHARMACOLOGY
2.1 - Receptor Pharmacology of the Pupil (Complete)
AUTONOMIC RECEPTORS CONTROLLING PUPIL SIZE:
SPHINCTER PUPILLAE:
Receptor: MUSCARINIC (M3 subtype)
Neurotransmitter: Acetylcholine (ACh)
Pathway: Edinger-Westphal nucleus → CN III → ciliary ganglion
→ short ciliary nerves → sphincter
Activated by: Light (reflex), near vision (accommodation-convergence)
DILATOR PUPILLAE:
Receptor: ALPHA-1 ADRENERGIC
Neurotransmitter: Noradrenaline (NA)
Pathway: Hypothalamus → ciliospinal centre (C8-T2)
→ superior cervical ganglion → internal carotid artery
→ nasociliary nerve → long ciliary nerves → dilator
DRUG EFFECTS - COMPLETE TABLE:
┌──────────────────────┬───────────────────┬──────────────────────┐
│ Drug │ Receptor/Mechanism│ Pupil Effect │
├──────────────────────┼───────────────────┼──────────────────────┤
│ PILOCARPINE │ M3 agonist │ MIOSIS │
│ (1-4%) │ Direct ACh mimic │ Also: ciliary muscle │
│ │ │ spasm → accommodation│
├──────────────────────┼───────────────────┼──────────────────────┤
│ CARBACHOL │ M1+M3 agonist │ MIOSIS (stronger) │
│ │ + nicotinic │ Resistant to │
│ │ (not broken by │ cholinesterase │
│ │ acetylcholinest.) │ │
├──────────────────────┼───────────────────┼──────────────────────┤
│ ATROPINE (1%) │ M3 antagonist │ MYDRIASIS + CYCLOPLEGIA│
│ │ Blocks ACh at │ Longest duration: │
│ │ sphincter │ 14 days │
├──────────────────────┼───────────────────┼──────────────────────┤
│ CYCLOPENTOLATE (1%) │ M3 antagonist │ MYDRIASIS + CYCLOPLEGIA│
│ │ │ Duration: 24h │
│ │ │ Used for refraction │
├──────────────────────┼───────────────────┼──────────────────────┤
│ TROPICAMIDE (0.5/1%) │ M3 antagonist │ MYDRIASIS + mild │
│ │ (shortest acting) │ cycloplegia │
│ │ │ Duration: 4-6h │
│ │ │ Used for fundoscopy │
├──────────────────────┼───────────────────┼──────────────────────┤
│ PHENYLEPHRINE (2.5/ │ Alpha-1 agonist │ MYDRIASIS (no │
│ 10%) │ Stimulates dilator│ cycloplegia) │
│ │ │ Blanches conjunctiva │
├──────────────────────┼───────────────────┼──────────────────────┤
│ COCAINE (4-10%) │ NA reuptake block │ MYDRIASIS │
│ │ ↑ NA at dilator │ + vasoconstriction │
├──────────────────────┼───────────────────┼──────────────────────┤
│ APRACLONIDINE (1%) │ Alpha-2 agonist │ Mild MYDRIASIS │
│ │ (also mild α-1) │ + eyelid retraction │
├──────────────────────┼───────────────────┼──────────────────────┤
│ HYDROXYAMPHETAMINE │ NA releaser from │ MYDRIASIS │
│ (1%) │ presynaptic nerve │ (requires intact │
│ │ terminals │ postganglionic neuron│
│ │ │ with NA stores) │
└──────────────────────┴───────────────────┴──────────────────────┘
2.2 - Pharmacological Diagnosis of Pupil Disorders
Horner Syndrome - 3-Neuron Pathway + Drug Testing
HORNER SYNDROME
= Oculosympathetic paresis
= Interruption of the 3-neuron sympathetic pathway to the eye
COMPLETE CLINICAL TRIAD:
1. PTOSIS (mild, 2mm) → loss of Müller's muscle (sympathetic)
2. MIOSIS (small pupil) → loss of dilator pupillae
3. ANHIDROSIS of face → loss of facial sweating fibers
PLUS: Enophthalmos (apparent, not real → small palpebral fissure)
Lower lid elevation (upside-down ptosis, reverse ptosis)
THE 3-NEURON PATHWAY:
┌────────────────────────────────────────────────────────────┐
│ 1st ORDER NEURON (Central) │
│ Hypothalamus → descends in brainstem + spinal cord │
│ → Ciliospinal centre of Budge (C8-T2) │
│ │
│ Lesions: Brainstem stroke, MS, syringomyelia, │
│ cervical cord tumour, Pancoast tumour (apex lung) │
├────────────────────────────────────────────────────────────┤
│ 2nd ORDER NEURON (Preganglionic) │
│ C8-T2 → exit ventral horn → over apex of lung │
│ → around subclavian artery → up carotid sheath │
│ → Superior cervical ganglion (SCG) │
│ │
│ Lesions: Pancoast tumour ★ (most important) │
│ Thyroid goitre, neck surgery, carotid artery dissection, │
│ cervical lymph nodes, aortic aneurysm (aortic arch) │
├────────────────────────────────────────────────────────────┤
│ 3rd ORDER NEURON (Postganglionic) │
│ SCG → travels with INTERNAL CAROTID ARTERY │
│ → through cavernous sinus (joins CN VI briefly) │
│ → via nasociliary branch of V1 → long ciliary nerves │
│ → dilator pupillae + Müller's muscle │
│ │
│ SUDOMOTOR (sweating) fibers travel with EXTERNAL CAROTID │
│ (not internal) → 3rd order Horner has NO anhidrosis! │
│ │
│ Lesions: Carotid artery dissection, cavernous sinus │
│ thrombosis, cluster headache (pericarotid inflammation) │
└────────────────────────────────────────────────────────────┘
Drug Tests for Horner - The KEY Pharmacological Principle
PHARMACOLOGICAL TESTING IN HORNER SYNDROME
STEP 1: CONFIRM HORNER (any level of lesion)
Using: COCAINE 4-10% drops (or APRACLONIDINE 1%)
COCAINE TEST:
Mechanism: Blocks REUPTAKE of noradrenaline
→ NA accumulates at the synapse → dilates normal pupil
NORMAL pupil: Intact postganglionic neuron releasing NA
→ cocaine blocks reuptake → ↑ NA → MYDRIASIS
HORNER pupil (any level): Interrupted sympathetic pathway
→ NA not being released (nerve damaged)
→ Cocaine has NO NA to block reuptake of
→ Horner pupil DOES NOT DILATE (or dilates very poorly)
RESULT: Anisocoria INCREASES after cocaine
(normal eye dilates, Horner eye stays small)
APRACLONIDINE 1% (now preferred, more widely available):
Mechanism: Alpha-2 agonist (also mild alpha-1)
Normal pupil:
→ Alpha-1 stimulation → mild mydriasis
→ Alpha-2 stimulation → reduces NA release (presynaptic)
→ Net effect: MILD MYDRIASIS or no change
Horner pupil:
→ Postganglionic neuron damaged → alpha-1 receptors on
dilator pupillae undergo DENERVATION SUPERSENSITIVITY
(upregulate receptors, become hyperresponsive to any agonist)
→ Even mild alpha-1 stimulation from apraclonidine
→ REVERSAL OF ANISOCORIA (Horner pupil dilates, becomes equal
or larger than normal pupil)
→ PTOSIS ALSO REVERSES (Müller's muscle supersensitive)
DIAGNOSTIC: Reversal of anisocoria + ptosis = POSITIVE Horner test
ADVANTAGE: Available everywhere (used for IOP spikes)
DISADVANTAGE: May give false negative in acute Horner (<1 week)
(denervation supersensitivity takes days to develop)
STEP 2: LOCALIZE HORNER (which neuron?)
Using: HYDROXYAMPHETAMINE 1%
Mechanism: Releases stored NA from PRESYNAPTIC TERMINALS
(requires intact 3rd-order neuron with NA vesicles to work)
1st or 2nd order lesion (3rd neuron INTACT):
→ Hydroxyamphetamine → releases NA from intact 3rd neuron
→ DILATES the Horner pupil
→ (3rd neuron is healthy, has NA stores)
3rd order lesion (3rd neuron DAMAGED):
→ No intact nerve terminals → no NA stores to release
→ Hydroxyamphetamine → NO DILATION of Horner pupil
→ (Cannot release from a dead nerve)
LOCALIZATION CHART:
┌──────────────────────────────────────────────────────────────┐
│ Test │ 1st/2nd order Horner │ 3rd order Horner │
├──────────────────────────────────────────────────────────────┤
│ Cocaine │ No dilation (confirms│ No dilation (confirms │
│ │ Horner any level) │ Horner any level) │
│ Apraclonidine │ Reversal of anisokor.│ Reversal (+ strong) │
│ │ (confirms Horner) │ (confirms Horner) │
│ Hydroxy- │ DILATES │ DOES NOT DILATE │
│ amphetamine │ (3rd neuron intact) │ (3rd neuron damaged) │
└──────────────────────────────────────────────────────────────┘
WAIT 48 HOURS between cocaine and hydroxyamphetamine tests
(cocaine depletes NA stores → false negative with hydroxyamphetamine if done same day)
CLINICAL URGENCY:
3rd order Horner → Internal carotid artery dissection
→ EMERGENCY (risk of stroke) → urgent MRI/MRA
New Horner + neck/facial pain = carotid dissection until proven otherwise
2nd order Horner + ipsilateral arm pain → PANCOAST TUMOUR
→ Urgent chest X-ray + CT chest
2.3 - Adie's Tonic Pupil - Pharmacological Diagnosis
ADIE'S TONIC PUPIL (Adie syndrome)
Pathology: Damage to ciliary ganglion
→ Loss of postganglionic PARASYMPATHETIC neurons
→ Sphincter pupillae denervated
→ DENERVATION SUPERSENSITIVITY develops
(M3 muscarinic receptors on sphincter upregulate)
Clinical:
- DILATED pupil (unilateral usually)
- SLUGGISH or ABSENT light reflex (sphincter not responding)
- TONIC near reflex (slow constriction to near, SLOW re-dilation)
= "Light-near dissociation" but different from AR pupil
- Vermiform (worm-like) iris movements at slit lamp
(sectoral palsy of sphincter - uneven re-innervation)
- Associated: Absent deep tendon reflexes (Holmes-Adie syndrome)
PHARMACOLOGICAL CONFIRMATION:
DILUTE PILOCARPINE 0.1% (one-tenth normal strength)
Mechanism exploited: Denervation supersensitivity
Normal sphincter: Requires FULL-STRENGTH pilocarpine (1-4%)
to show significant constriction
→ 0.1% pilocarpine → minimal/no constriction of NORMAL pupil
Adie's pupil: M3 receptors SUPERSENSITIVE (upregulated)
→ 0.1% pilocarpine (dilute) → MARKED CONSTRICTION
→ Pupil constricts significantly with dose that barely
affects a normal eye
RESULT: Adie's pupil constricts to 0.1% pilocarpine
Normal pupil does NOT constrict to 0.1% pilocarpine
KEY DISTINCTION FROM 3RD NERVE PALSY:
┌────────────────────────────────────────────────────┐
│ ADIE'S vs CN III PALSY │
├───────────────────┬────────────────────────────────┤
│ Feature │ Adie's │ CN III Palsy │
├───────────────────┼─────────────────┼───────────────┤
│ Ptosis │ NONE │ Complete ptosis│
│ EOM restriction │ NONE │ YES (down+out) │
│ Pupil │ Dilated, tonic │ Fixed, dilated │
│ Light reflex │ Sluggish │ Absent │
│ Near reflex │ Slow but present│ May be absent │
│ 0.1% Pilocarpine │ CONSTRICTS │ No constriction│
│ Cause │ Benign (viral, │ Aneurysm, DM, │
│ │ post-viral) │ herniation │
└───────────────────┴─────────────────┴───────────────┘
2.4 - Argyll Robertson Pupil - Pharmacological Basis
ARGYLL ROBERTSON (AR) PUPIL - "Prostitute's Pupil"
(accommodates but doesn't react)
Classical description:
- Bilateral, small (miotic) pupils
- ABSENT light reflex
- PRESERVED near (accommodation-convergence) reflex
= Light-near dissociation
Cause: NEUROSYPHILIS (Treponema pallidum)
(also seen in: DM, MS - rarely)
ANATOMICAL BASIS:
The pretectal nucleus in midbrain mediates the LIGHT REFLEX
→ Syphilis → damage to pretectal neurons
→ Light reflex LOST
The near reflex uses a DIFFERENT PATHWAY:
→ Visual cortex → frontal eye fields → EW nucleus
→ (bypasses pretectal nucleus)
→ Near reflex PRESERVED
PHARMACOLOGICAL BEHAVIOUR:
Poor dilation with mydriatics (ATROPINE, PHENYLEPHRINE)
→ Sphincter has developed FIBROSIS (chronic denervation)
→ Does not respond normally to drug stimulation either
Poor response to pilocarpine
→ Already miotic, cannot constrict further
DISTINCTION FROM ADIE'S:
┌────────────────────────────────────────────────────┐
│ ADIE'S vs AR PUPIL │
├─────────────────────┬──────────────┬───────────────┤
│ Feature │ Adie's │ AR Pupil │
├─────────────────────┼──────────────┼───────────────┤
│ Size │ LARGE │ SMALL (miotic)│
│ Light reflex │ Absent/poor │ ABSENT │
│ Near reflex │ Preserved │ PRESERVED │
│ 0.1% Pilocarpine │ CONSTRICTS │ No change │
│ Bilaterality │ Usually unilateral│ BILATERAL│
│ Cause │ Benign viral │ SYPHILIS │
└─────────────────────┴──────────────┴───────────────┘
MNEMONIC: "AR (Argyll Robertson) = Accommodation Retained"
"Prostitute's pupil = accommodates but won't react to light"
2.5 - Pharmacological Pupil Dilation for Fundoscopy
MYDRIATICS FOR EXAMINATION - WHICH TO USE WHEN:
ROUTINE FUNDOSCOPY:
Tropicamide 1% + Phenylephrine 2.5%
→ Combination: muscarinic block (tropicamide) +
alpha-1 stimulation (phenylephrine)
→ Synergistic mydriasis (better than either alone)
→ Onset: 20-30 minutes
→ Duration: 4-6 hours
→ WARNING before instilling: Ask about:
1. Narrow angle? (risk of acute angle closure)
2. Driving? (patient cannot drive for 4-6h)
3. Allergy to either drug?
REFRACTION IN CHILDREN (cycloplegia required):
Cyclopentolate 1% (children > 3 months)
Atropine 1% (young children, high hypermetropia, esotropia)
WHY CYCLOPLEGIA NEEDED IN CHILDREN:
Children have powerful accommodation (up to +20D)
→ Without cycloplegia → ciliary muscle contracts
→ Lens accommodates → falsely increases myopia / masks hyperopia
→ Must PARALYZE ciliary muscle to get true refractive error
Drug Cycloplegia onset Duration Use
Cyclopentolate 1% 20-30 min 24h Standard paed refraction
Atropine 1% 1-3 days 14 days High hyperopia, esotropia
PHENYLEPHRINE 10% CAUTION:
Risk: Systemic cardiovascular effects (hypertension, tachycardia)
→ In children: Use 2.5% only (never 10%)
→ In cardiovascular disease: Use 2.5%, avoid 10%
→ Pre-treatment with topical anaesthetic reduces systemic absorption
(less stinging → less reflex tearing → less nasolacrimal washout)
PHARMACOLOGY HIGH-YIELD SUMMARY TABLE ★★★
| Drug | Receptor | Mechanism | Pupil Effect | Duration | Key Exam Point |
|---|---|---|---|---|---|
| Pilocarpine 1-4% | M3 agonist | Direct ACh mimic | Miosis + accommodation | 4-6h | Glaucoma treatment, also causes brow ache |
| Tropicamide 1% | M3 antagonist | Blocks ACh | Mydriasis + mild cycloplegia | 4-6h | Fundoscopy drops |
| Cyclopentolate 1% | M3 antagonist | Blocks ACh | Mydriasis + cycloplegia | 24h | Pediatric refraction |
| Atropine 1% | M3 antagonist | Blocks ACh | Mydriasis + max cycloplegia | 14 days | Penalization, esotropia, max cycloplegia |
| Phenylephrine 2.5/10% | Alpha-1 agonist | Stimulates dilator | Mydriasis only (no cycloplegia) | 3h | Fundoscopy adjunct, NO cycloplegia |
| Cocaine 4-10% | NA reuptake blocker | ↑NA at dilator | Mydriasis | - | Confirms Horner (fails to dilate Horner pupil) |
| Apraclonidine 1% | Alpha-2 agonist | Denervation SS | Reverses Horner anisocoria | - | Diagnose/confirm Horner (reversal of anisocoria) |
| Hydroxyamphetamine 1% | NA releaser | Releases NA vesicles | Dilates if 3rd neuron intact | - | Localizes Horner to 3rd order (no dilation = 3rd order) |
| Dilute pilocarpine 0.1% | M3 agonist | Denervation SS | Constricts Adie's pupil only | - | Diagnoses Adie's tonic pupil |
| Proxymetacaine 0.5% | Na+ channel blocker | Blocks nerve conduction | No pupil effect | 10-20 min | Safest topical anaesthetic, least allergenic |
Quick-Fire Pharmacology "Why" Questions ★★★
| Question | Answer |
|---|---|
| Why is latanoprost a prodrug? | Too hydrophilic in active form → ester group added → lipophilic → crosses epithelium → esterases cleave → active PGF2α released |
| Why does mydriatic work slower in brown irides? | Melanin binds alpha-agonists → slower release → delayed onset |
| Why do topical drops cause systemic side effects? | Nasolacrimal drainage → nasal mucosa → systemic absorption bypassing liver first-pass |
| Why press the inner canthus after eye drops? | Punctal occlusion → blocks nasolacrimal drainage → more drug stays in eye, less systemic absorption |
| Why does fluorescein stain epithelial defects (not intact epithelium)? | Tight junctions exclude it when intact; gap in epithelium allows entry |
| Why does Rose Bengal sting more in dry eye? | No aqueous dilution, and devitalized mucin-stripped cells have no protection |
| Why not send home topical anaesthetic drops? | Loss of protective blink reflex + direct epithelial toxicity → severe keratopathy |
| Why does Horner pupil not dilate with cocaine? | No NA being released from damaged sympathetic neuron → cocaine has nothing to block reuptake of |
| Why does Adie's constrict to 0.1% pilocarpine? | Denervation supersensitivity → upregulated M3 receptors → hypersensitive to even dilute agonist |
| Why is there no anhidrosis in 3rd order Horner? | Sweating fibers travel with external carotid, not internal → 3rd order lesion (internal carotid) spares sweating |
| Part | Content |
|---|---|
| Part 1 | Structural anatomy - all 3 coats, lens, vitreous, retinal layers (with histology images) |
| Part 2 | Embryology + Limbus/TM/Gonioscopy + Optic Nerve Head |
| Part 3 | Applied and Surgical Anatomy - surgical steps + clinico-anatomical "why" questions |
| Part 4 | Pharmacological Basis - corneal drug penetration, diagnostic dyes, topical anaesthetics, complete pupil pharmacology, Horner/Adie/AR tests |
Create a study guide PDF combining all Week 1 parts (Parts 1-4)
WHAT HAPPENED
WHY
MAKE IT IN PART