Breast in detail according to Sabiston
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have enough content to compose a comprehensive, detailed response on the Breast chapter from Sabiston. Let me compile it all.
The Breast - Sabiston Textbook of Surgery (Chapter 68)
ANATOMY
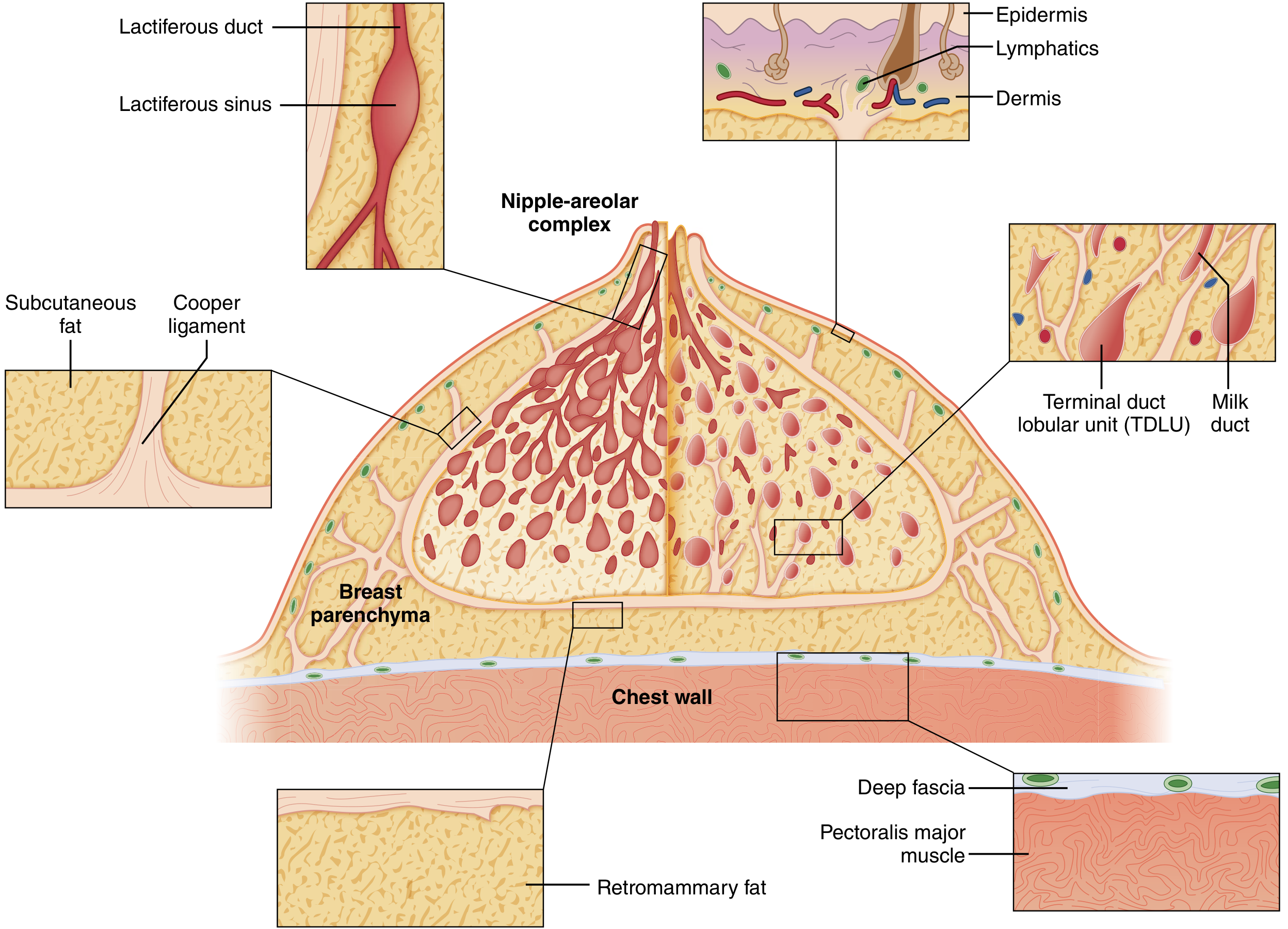
Fig. 68.1 - Cutaway diagram of the mature resting breast.
The breast lies between the skin/subdermal adipose layer and the superficial pectoral fascia, overlying the pectoralis major. The pectoralis minor sits deep to pec major, enclosed in the clavipectoral fascia, which fuses laterally with the axillary fascia.
Cooper's (Suspensory) Ligaments: Multiple fibrous bands running between the chest wall and dermis. They give the breast its shape. When infiltrated by cancer, they cause dimpling - "orange skin" (peau d'orange).
Tissue composition (three principal types):
- Glandular epithelium
- Fibrous stroma
- Adipose tissue
Also contains lymphocytes and macrophages.
- In adolescents: epithelium + stroma predominate
- Postmenopause: glandular structures involute, replaced by adipose tissue
Ductal System:
- Branching ducts in a radial pattern from the nipple-areolar complex (NAC)
- 15-20 lobes, each ending in a lactiferous duct opening at the nipple
- Each duct has a dilated lactiferous sinus below the NAC
- Terminal branching ends in terminal ductules (acini) = the milk-forming glands
- Acini + efferent ductules = Terminal Duct Lobular Units (TDLUs) - the functional unit
- TDLUs are invested in specialized loose connective tissue (intralobular stroma - distinct from denser interlobular stroma)
Lymphatic Drainage:
- Axillary nodes: ~75% of breast lymph drains here (level I, II, III)
- Internal mammary nodes
- Supraclavicular nodes
BREAST DEVELOPMENT AND PHYSIOLOGY
Breast development (thelarche) is estrogen-driven during puberty. Progesterone drives lobular-alveolar development. During pregnancy, prolactin and HPL promote full glandular development. Lactation is sustained by prolactin; oxytocin drives milk ejection. After menopause, glandular tissue involutes to be replaced by fat.
CLINICAL APPROACH TO THE BREAST PATIENT
Patient History
Key elements include:
- Pain (cyclical vs. noncyclical)
- Nipple discharge (color, single vs. multiple ducts, unilateral vs. bilateral)
- Masses (duration, change with menstrual cycle)
- Skin changes
- Risk factors (family history, prior biopsies, hormone use, radiation history)
Physical Examination
Inspection (sitting position):
- Asymmetry, skin changes, nipple retraction, peau d'orange, Paget disease
- Performed with arms at side, then raised, then hands pressed on hips
Palpation:
- Axilla, supraclavicular and infraclavicular spaces for lymphadenopathy (seated)
- Breast palpation: patient supine, arm above head, compression toward chest wall
- Systematic palpation of each quadrant + tissue under NAC
- Characterize masses: size, shape, consistency, location (clock position + cm from nipple), fixation to skin/muscle
Key clinical signs:
- Peau d'orange: edema/dimpling from dermal lymphatic blockage - most feared cause is inflammatory carcinoma
- Nipple discharge from single duct: may signify underlying pathology (e.g., papilloma)
- Paget disease of nipple: psoriatic rash starting at nipple, spreading to areola - malignant ductal cells invading epidermis
- Skin dimpling: traction on Cooper ligaments by scirrhous tumor, best seen with angled indirect lighting during arm abduction
BREAST IMAGING AND DIAGNOSTIC BIOPSY
Screening Mammography
- Performed in asymptomatic females to detect occult cancer
- Average-risk = no personal history, no strong family history, no BRCA mutation, no chest RT before age 30
Guidelines (NCCN):
| Risk | Recommendation |
|---|---|
| Average risk | Annual mammography beginning at age 40 |
| High risk (≥20% lifetime risk) | Annual mammography + MRI beginning at age 30 (or 10 years before earliest affected relative's diagnosis) |
Imaging Modalities
Mammography:
- Primary screening tool; can detect microcalcifications, masses, architectural distortion
- BI-RADS classification (0-6): 0 = incomplete, 1 = negative, 2 = benign, 3 = probably benign (6-month follow-up), 4 = suspicious (biopsy), 5 = highly suggestive of malignancy, 6 = known malignancy
- Sensitivity ~85%; reduced in dense breasts
Ultrasonography (US):
- Differentiates cystic from solid masses
- Useful in dense breasts, pregnant/lactating females
- Not a standalone screening tool; used as extension of physical exam
- Simple cysts: anechoic, posterior acoustic enhancement, thin smooth walls - no further workup needed
Magnetic Resonance Imaging (MRI):
- Most sensitive modality (~90-95%)
- Indications: screening in high-risk patients (BRCA+), extent of disease for newly diagnosed cancer, response to neoadjuvant therapy, occult primary breast cancer, implant evaluation
- Lower specificity than mammography; high false-positive rate
Biopsy Techniques
| Technique | Notes |
|---|---|
| Fine-Needle Aspiration (FNA) | Cytology only; cannot distinguish invasive from in situ; minimal tissue; useful for cysts and palpable nodes |
| Core-Needle Biopsy (CNB) | Preferred; provides histology (architecture intact); 14-gauge or vacuum-assisted; can determine ER/PR/HER2 status |
| Excisional Biopsy | Surgical removal of entire lesion; used when CNB fails or is nondiagnostic |
IDENTIFICATION AND CARE OF HIGH-RISK PATIENTS
Risk Factors for Breast Cancer (Box 68.1)
Demographic/Lifestyle:
- Increased age (peaks in 8th decade)
- Female sex
- Shift work (nighttime)
- Obesity, smoking, alcohol, physical inactivity
- High-fat/low-fiber diet
Hormone Exposure:
- Early menarche (before age 11)
- Late menopause (after age 55)
- Nulliparity / fewer live births
- First full-term pregnancy after age 30
- Lack of breastfeeding
- HRT, OCP use
Chest Wall Radiation: Radiation before age 30 (e.g., for Hodgkin lymphoma)
Genetic Risk:
- Family history of breast/ovarian cancer
- BRCA1 (chr 17q): 60-80% lifetime risk; associated with triple-negative cancers
- BRCA2 (chr 13q): 40-70% lifetime risk; associated with ER+ cancers; also male breast cancer
- Other: TP53 (Li-Fraumeni), PTEN (Cowden), CDH1 (lobular), PALB2, ATM, CHEK2
Histologic Risk Factors (Relative Risks):
- Proliferative disease without atypia (sclerosing adenosis, papillomatosis, moderate hyperplasia): RR 1.3-1.9
- Proliferative disease with atypia (ADH, ALH): RR 3.7-4.2
- LCIS: RR >7
Risk Assessment Models
- Gail Model: age, race, menarche, first live birth, prior biopsies, atypia, family history; best for average-risk women
- Tyrer-Cuzick (IBIS): incorporates BRCA probability; preferred for high-risk assessment
- ≥20% lifetime risk = high-risk category (qualifies for MRI screening + chemoprevention discussion)
Care of High-Risk Patients
Close surveillance: Annual mammogram + MRI, clinical breast exam every 6-12 months
Chemoprevention:
| Agent | Mechanism | Notes |
|---|---|---|
| Tamoxifen | SERM; blocks ER | 49% RRR in NSABP P-1; premenopausal + postmenopausal; increases risk of endometrial cancer, DVT |
| Raloxifene | SERM | STAR trial: equivalent to tamoxifen in postmenopausal; lower endometrial cancer/DVT risk |
| Exemestane (AI) | Aromatase inhibitor | MAP.3 trial: 65% RRR; postmenopausal only; bone loss risk |
| Anastrozole (AI) | Aromatase inhibitor | IBIS-II trial: 50% RRR; postmenopausal only |
Prophylactic Mastectomy:
- Reduces breast cancer risk by ~90-95% in BRCA carriers
- Bilateral prophylactic salpingo-oophorectomy (BPSO) reduces risk further and addresses ovarian cancer risk
- Genetic counseling and multidisciplinary discussion essential before proceeding
BENIGN BREAST DISEASES
Fibrocystic Changes and Mastalgia
- Common in 4th-5th decades; exaggerated response to hormones/growth factors
- Cyclic mastalgia: premenstrual, bilateral, resolves with menopause
- Noncyclic mastalgia: idiopathic, harder to treat; require breast imaging in women ≥30
- Scapulothoracic bursitis: referred pain along intercostal nerves mimicking breast pain; trigger-point injections diagnostic + therapeutic
- Histology: macrocysts, microcysts, adenosis, sclerosis, apocrine metaplasia, stromal fibrosis, epithelial hyperplasia
- Simple cysts: confirmed on US; no further workup needed; aspiration if symptomatic; vacuum-assisted excision for large recurrent cysts
- Treatment of mastalgia: danazol, Lupron, tamoxifen (significant side effects); NSAIDs for noncyclical
Fibroadenomas
- Most common breast tumor in young females (teens to 30s)
- Arise from TDLUs; estrogen-sensitive - grow in pregnancy, regress after menopause
- Well-circumscribed, rubbery, mobile ("breast mouse")
- US: homogeneous, hypoechoic, well-defined
- Giant fibroadenoma (>5 cm): may require excision
- Management: CNB confirmation + observation if classic features; excise if enlarging, >3 cm, or patient preference
Breast Infections and Abscess
- Lactational mastitis: S. aureus most common; treat with antibiotics + continued breastfeeding; progress to abscess in ~10%
- Periductal (non-lactational) mastitis: associated with smoking, subareolar; mixed flora; recurrent; fistula formation common
- Abscess: US-guided aspiration or incision and drainage; must exclude inflammatory carcinoma
Idiopathic Granulomatous Mastitis
- Rare; mimics carcinoma clinically
- Diagnosis by core biopsy; rule out TB, fungal infections
- Treatment: steroids ± methotrexate; surgery for resistant cases
Nipple Discharge
- Physiologic (bilateral, multiple ducts, non-spontaneous, non-bloody): reassurance
- Pathologic (unilateral, single duct, spontaneous, bloody/serous): requires workup
- Most common causes: intraductal papilloma (most common cause of bloody discharge), duct ectasia, carcinoma
- Workup: cytology, ductography/galactography, duct excision (microdochectomy)
Papillomas and Papillomatosis
- Solitary papilloma: most common cause of bloody nipple discharge; low malignant potential; treated by duct excision
- Multiple peripheral papillomas (papillomatosis): higher risk of atypia and subsequent carcinoma
Fat Necrosis
- Post-traumatic or post-surgical; mimics carcinoma on imaging (oil cyst, calcifications, spiculated mass)
- Biopsy if imaging uncertain; no treatment if confirmed
Gynecomastia
- Benign glandular proliferation in males; due to estrogen-androgen imbalance
- Causes: puberty, liver disease, renal failure, hypogonadism, drugs (spironolactone, cimetidine, marijuana, anabolic steroids), tumors (HCG-secreting)
- Management: treat underlying cause; tamoxifen/anastrozole pharmacologically; subcutaneous mastectomy for cosmetically unacceptable cases
EPIDEMIOLOGY OF BREAST CANCER
- 297,790 cases of invasive + 55,720 in situ breast cancer diagnosed in the US (2023)
- Second leading cause of cancer death in females (after lung); ~43,700 deaths in 2023
- Most prevalent cancer worldwide: >2 million cases, ~685,000 deaths/year
- 5-year survival improved: 63% (1960s) → 91% (2012-2018)
- Highest incidence in White females (133.7/100,000); highest mortality in Black females (40% higher than White) - due to higher TNBC incidence, later-stage diagnosis, and disparate access to care
PATHOLOGY OF BREAST CANCER
Noninvasive (In Situ) Breast Cancer
DCIS (Ductal Carcinoma In Situ):
- Malignant epithelial cells confined within ductal system, basement membrane intact
- Classified by architecture (comedo, cribriform, micropapillary, papillary, solid) and nuclear grade (low, intermediate, high)
- Comedo DCIS (high-grade, central necrosis with calcifications): more aggressive, higher local recurrence risk
- Treatment: BCS + radiation; mastectomy for extensive/multicentric DCIS; endocrine therapy (tamoxifen) to reduce contralateral risk in ER+ DCIS
LCIS (Lobular Carcinoma In Situ):
- No longer classified as carcinoma in AJCC 8th edition - recognized as a risk marker
- Bilateral, multicentric; most detected incidentally
- Marker for subsequent invasive cancer (bilateral risk, either ductal or lobular)
- Management: surveillance or chemoprevention; bilateral prophylactic mastectomy in select high-risk cases
Invasive Breast Cancer
Classification (Box 68.2):
| Type | Frequency | Features |
|---|---|---|
| Invasive ductal carcinoma (IDC/NST) | ~75% | Most common; no special type; variable grade |
| Invasive lobular carcinoma (ILC) | ~10-15% | Single-file ("Indian file") growth pattern; lacks E-cadherin; higher bilateral risk; harder to detect on mammography |
| Tubular | <5% | Well-differentiated; excellent prognosis |
| Mucinous (colloid) | <5% | Gelatinous tumor; favorable prognosis; older women |
| Medullary | <5% | Lymphocytic infiltrate; high grade but better prognosis |
| Inflammatory | 1-5% | Most aggressive; dermal lymphatic involvement |
Molecular Markers (Intrinsic Subtypes)
| Subtype | Receptors | Features |
|---|---|---|
| Luminal A | ER+/PR+, HER2-, low Ki-67 | Best prognosis; endocrine therapy |
| Luminal B | ER+/PR+, HER2+ or high Ki-67 | Intermediate prognosis; endocrine ± chemo |
| HER2-enriched | ER-, PR-, HER2+ | Aggressive; anti-HER2 targeted therapy |
| Triple-Negative (TNBC) | ER-, PR-, HER2- | Most aggressive; chemotherapy only; higher in Black women |
Genomic Assays:
- Oncotype DX (21-gene): predicts recurrence score (RS) and benefit from chemotherapy in ER+/HER2-/N0 or N1 disease
- RS <18: endocrine therapy alone; RS ≥18 (node-negative, postmenopausal) or ≥26: benefit from chemotherapy
- MammaPrint (70-gene): risk stratification for distant recurrence
Other Breast Tumors
Phyllodes Tumors:
- Stromal/epithelial mixed tumor; classified benign, borderline, malignant
- Present as rapidly enlarging mass (bulky, firm); leaf-like architecture on histology
- Treatment: wide local excision with 1-cm margins; mastectomy for large/malignant
- Malignant phyllodes: sarcomatous stroma; hematogenous spread (not lymphatic - no axillary dissection needed)
Angiosarcoma:
- Rare; primary (young women) or secondary (post-radiation, post-lymphedema - Stewart-Treves syndrome)
- Purple/blue skin discoloration; aggressive; poor prognosis
- Treatment: wide surgical resection; chemotherapy (anthracycline-based)
STAGING (AJCC 8th Edition)
TNM staging augmented with:
- Tumor grade (histologic)
- Biologic markers: ER, PR, HER2 status
- Genomic assays (Oncotype DX RS, where applicable)
- Response to neoadjuvant therapy
Prefixes/Suffixes:
yprefix: after neoadjuvant therapy (ypTNM)rprefix: recurrent tumormsuffix: multiple primary tumorsc= clinical staging;p= pathologic staging
Clinical workup for staging:
- History + physical + bilateral breast imaging for all patients
- CT, bone scan reserved for: clinically positive nodes, abnormal labs/CXR, locally advanced/inflammatory cancer, or symptomatic patients
SURGICAL TREATMENT OF BREAST CANCER
Historical Perspective
- Halsted radical mastectomy (1894): en bloc removal of breast, both pectoral muscles, axillary contents - reduced local recurrence but no survival benefit vs. less aggressive surgery
- Modified radical mastectomy (MRM): removes breast + pectoralis fascia + axillary dissection; preserves pectoralis muscles (Patey/Auchincloss procedures) - became standard
- NSABP B-06 trial: proved BCS + RT equivalent to total mastectomy in OS and DFS for tumors ≤4 cm
Selection of Surgical Therapy
Breast-Conserving Surgery (BCS/Lumpectomy) + Radiation = Standard for most stage I-II cancers
Absolute Contraindications to Radiation (Box 68.4 - contraindications to BCS):
- Prior breast or chest wall radiation
- Active connective tissue disease involving skin (scleroderma, lupus)
- Pregnancy (1st/2nd trimester)
- Multicentric disease
- Diffuse malignant-appearing microcalcifications
Relative Contraindications:
- Large tumor-to-breast ratio
- Involved margins after reexcision
- Certain collagen vascular diseases
Breast-Conserving Surgery (BCS) - Technical Aspects
- Also called: lumpectomy, partial mastectomy, segmentectomy, wide local excision
- Excise tumor with surrounding rim of grossly normal parenchyma
- Specimen oriented + inked before sectioning
- Specimen radiography for all nonpalpable lesions or lesions with microcalcifications
- Cavity shave margins (level I evidence): reduce positive margins and need for re-excision
- Clips placed in cavity for radiation planning
Margin Standards:
- Invasive cancer: "no ink on tumor" = adequate negative margin (SSO/ASTRO consensus)
- DCIS: ≥2 mm = adequate negative margin (SSO/ASTRO/ASCO consensus)
Localization of Nonpalpable Lesions
- Wire-localization (traditional)
- Radioactive seed localization
- Magnetic seed (Magseed)
- Radar reflector (SAVI SCOUT)
- Radioactive tracer injection (SCOUT)
Mastectomy Types
| Type | Breast Tissue | Pectoralis | Axillary Dissection | Notes |
|---|---|---|---|---|
| Simple (total) | All + NAC | Preserved | No | For DCIS, prophylactic |
| Skin-sparing mastectomy (SSM) | All + NAC | Preserved | ± | Preserves skin envelope for reconstruction |
| Nipple-sparing mastectomy (NSM) | All | Preserved | ± | Preserves NAC; select cases |
| Modified radical (MRM) | All + NAC | Preserved | Yes (level I-III) | Standard for node-positive |
| Radical (Halsted) | All + NAC | Both removed | Yes | Historical; rarely used |
Axillary Surgery
Sentinel Lymph Node Biopsy (SLNB):
- Standard for clinically node-negative breast cancer
- Dual tracer (blue dye + radioisotope) maximizes identification rate and minimizes false-negative rate (FNR)
- If SLN negative: no further axillary surgery needed
- ACOSOG Z0011 trial: patients with 1-2 positive SLNs undergoing BCS + whole breast irradiation (WBI) - ALND can be omitted without difference in OS or DFS
- AMAROS trial: axillary RT equivalent to ALND for 1-2 positive SLNs
Axillary Lymph Node Dissection (ALND):
- Level I-III dissection (relative to pectoralis minor)
- Standard for: locally advanced/inflammatory breast cancer, >3 positive nodes, mastectomy without WBI, clinically positive nodes after neoadjuvant therapy
- Complications: lymphedema (~20%), paresthesias (intercostobrachial nerve), seroma, shoulder dysfunction
Sentinel Node in Neoadjuvant Setting:
- Initially cN+ patients: SLNB accuracy improved with ≥2 SLNs retrieved, dual tracer, and clipping the biopsy-proven node
- Targeted Axillary Dissection (TAD) = SLNB + retrieval of clipped biopsy-proven node: FNR as low as 1.4%
Axillary Reverse Mapping (ARM):
- Identifies arm lymphatics (blue dye in arm) vs. breast lymphatics (isotope in breast)
- Preserves arm lymphatics during ALND, reducing lymphedema
- Alliance 221702 is ongoing to validate
RADIATION THERAPY
After Breast-Conserving Surgery
- Whole breast irradiation (WBI): standard after BCS; reduces local recurrence by ~50-70%
- Hypofractionated WBI (FAST-Forward trial): 26 Gy/5 fractions (vs. standard 50 Gy/25 fractions) - equivalent outcomes; preferred for most patients
- Accelerated Partial Breast Irradiation (APBI): radiation to lumpectomy cavity only; suitable for select patients (see ASTRO guidelines - age ≥50, tumor ≤2 cm, pN0, negative margins ≥2 mm, ER+, no LVI)
- Radiation boost to lumpectomy cavity reduces local recurrence further, especially in young patients (<40)
Post-Mastectomy Radiation Therapy (PMRT)
- Indicated for: ≥4 positive lymph nodes, T3/T4 tumors, positive margins
- Consider for: 1-3 positive nodes (supported by Danish trials, EBCTCG meta-analysis)
- Danish Breast Cancer Cooperative Group Trials (82b/82c): PMRT + chemotherapy or tamoxifen significantly improved locoregional control and OS in stage II/III disease
- Radiation fields: chest wall + axillary, infraclavicular, supraclavicular, and internal mammary nodal basins
SYSTEMIC THERAPY
Goals and Assessment
- Adjuvant therapy reduces risk of distant recurrence and death
- Tools to assess benefit: ER/PR/HER2 status, grade, Oncotype DX, MammaPrint, Ki-67
- For ER+/HER2-/N0: TAILORx trial - Oncotype RS 0-10: endocrine therapy alone; RS 11-25 (postmenopausal): endocrine therapy alone; RS 26-100: add chemotherapy
- RxPONDER trial: in N1 (1-3 nodes) ER+/HER2- postmenopausal patients with RS ≤25: no benefit from adding chemotherapy
Chemotherapy
- Anthracyclines (doxorubicin/cyclophosphamide = AC) + Taxanes (paclitaxel/docetaxel) = backbone
- Regimens: TC (taxane + cyclophosphamide); AC-T; dose-dense AC-T
- Capecitabine: adjuvant in TNBC with residual disease after neoadjuvant chemo (CREATE-X trial)
- Olaparib/niraparib: PARP inhibitors for BRCA-mutated HER2-negative early breast cancer with residual disease (OlympiA trial)
HER2-Targeted Therapy
- Trastuzumab (Herceptin): anti-HER2 monoclonal antibody; ~50% reduction in recurrence; 1 year adjuvant
- Pertuzumab + trastuzumab: dual HER2 blockade; APHINITY trial: benefit in node-positive disease
- T-DM1 (ado-trastuzumab emtansine): for residual disease after neoadjuvant therapy (KATHERINE trial): reduces recurrence by 50%
- Lapatinib: oral TKI, dual EGFR/HER2 inhibitor; used in metastatic HER2+ disease
- Cardiotoxicity monitoring required for all HER2-targeted agents
Endocrine Therapy
Tamoxifen:
- SERM; competitive ER antagonist in breast (agonist in bone, endometrium)
- Standard for premenopausal ER+ breast cancer; also used postmenopausal
- 5 years: standard; ATLAS trial - 10 years reduces distant recurrence and mortality further
- Risks: endometrial cancer, thromboembolic events (DVT/PE), hot flashes
Aromatase Inhibitors (AIs):
- Anastrozole, letrozole (non-steroidal); exemestane (steroidal)
- Block peripheral aromatization of androgens to estrogen
- Postmenopausal only (ovarian estrogen production not suppressed)
- Superior to tamoxifen in postmenopausal ER+ disease (ATAC, BIG 1-98 trials)
- Risks: arthralgia, bone loss (osteoporosis), fractures - monitor bone density + bisphosphonates
Ovarian Suppression/Ablation:
- GnRH agonists (goserelin, leuprolide): medical castration
- Combined with AI (SOFT/TEXT trials): superior to tamoxifen alone in high-risk premenopausal patients
- Surgical oophorectomy: permanent
CDK4/6 Inhibitors (adjuvant):
- Abemaciclib (monarchE trial): adjuvant in high-risk ER+/HER2- patients with ≥4 nodes or 1-3 nodes + high-grade/large tumor/high Ki-67; added to endocrine therapy
Neoadjuvant Systemic Therapy
- Converts inoperable to operable disease; allows BCS in previously mastectomy-only candidates
- Provides in vivo chemosensitivity data; pathologic complete response (pCR) = prognostic marker
- pCR (no residual invasive disease in breast + nodes) correlates with improved survival, especially in TNBC and HER2+
- Residual disease after neoadjuvant: escalate therapy (T-DM1 for HER2+; capecitabine for TNBC; olaparib for BRCA-mutated)
TREATMENT OF SPECIAL CONDITIONS
Locally Advanced and Inflammatory Breast Cancer (LABC/IBC)
Locally Advanced (Stage IIB, IIIA, IIIB, IIIC):
- Includes: tumors >5 cm, chest wall involvement, skin involvement, bulky/fixed axillary nodes, internal mammary/supraclavicular involvement
- Current approach: neoadjuvant chemotherapy → surgery (MRM preferred) → RT ± further systemic therapy
- Surgery alone: 30-50% local recurrence; RT alone: similar; trimodality required
Inflammatory Breast Cancer:
- 1-5% of all breast cancers; most aggressive subtype
- Hallmark: dermal lymphatic involvement (pathologic) causing erythema, edema, warmth, peau d'orange
- Rapid onset: progression over weeks to 3 months
- Clinical diagnosis - palpable mass not required; pathologic confirmation of dermal lymphatics helpful but not prerequisite
- Staging: always T4d = stage IIIB minimum
- Treatment: neoadjuvant chemotherapy → modified radical mastectomy (no immediate reconstruction) → PMRT → adjuvant systemic therapy
- SLNB has high FNR in IBC - always perform ALND
- 5-year outcomes: locoregional recurrence ~6.9%; distant recurrence ~35.1% with trimodal treatment
Breast Cancer in Older Adults
- CALGB 9343 / PRIME-II trials: in women ≥65-70 with ER+, HER2-, small tumors (≤2-3 cm), clinically node-negative - lumpectomy + endocrine therapy without radiation: no OS difference at 10 years (inferior local control but clinically acceptable)
- SLNB may be safely omitted in older patients with early ER+ disease (SOUND, INSEMA trials evaluating this)
Breast Cancer in Males
- Rare (~1% of breast cancers)
- Risk factors: BRCA2 mutation (RR ~7), Klinefelter syndrome, gynecomastia, exogenous estrogens
- Usually ER+ (>90%); presents at more advanced stage due to delayed diagnosis
- Treatment: same principles as female breast cancer; MRM preferred (less breast tissue)
- Tamoxifen is the endocrine therapy of choice (AIs less effective due to intact gonadal estrogen production in premenopausal males)
Breast Cancer During Pregnancy (Pregnancy-Associated Breast Cancer)
- Defined as breast cancer diagnosed during pregnancy or within 1 year postpartum
- Most common cancer in pregnancy; ~1 in 3000 pregnancies
- Delayed diagnosis common due to physiologic breast changes
- Diagnosis: US safe at all trimesters; mammography (with shielding); MRI without gadolinium preferred in 2nd/3rd trimester; CNB safe
- Surgery: safe at any trimester; MRM if BCS would require radiation in 1st/2nd trimester
- Chemotherapy: safe after 1st trimester (AC regimen); taxanes in 2nd/3rd trimester
- Radiation: contraindicated during pregnancy
- HER2-targeted therapy: contraindicated (fetal harm - oligohydramnios)
- Endocrine therapy: contraindicated (teratogenic)
- Prognosis: stage for stage, similar to non-pregnant females; delayed diagnosis leads to worse outcomes
BREAST RECONSTRUCTION
Postmastectomy reconstruction options:
- Immediate: done at time of mastectomy; preferred for psychological wellbeing; requires coordination with oncologic surgery and radiation planning
- Delayed: after completion of all oncologic treatments; safer in high-risk radiation candidates
Reconstruction Types:
- Implant-based: tissue expander → permanent implant; most common; simpler; may be affected by radiation
- Autologous flaps:
- TRAM flap (transverse rectus abdominis myocutaneous): pedicled or free; abdominal donor site
- DIEP flap (deep inferior epigastric perforator): microsurgical; spares rectus muscle; preferred when available
- Latissimus dorsi flap: with or without implant; used when abdominal tissue unavailable
- SIEA flap (superficial inferior epigastric artery): alternative microsurgical; limited pedicle
- Nipple reconstruction: after breast mound achieved; tattooing for areola
Sabiston Textbook of Surgery, 21st Edition - Chapter 68: The Breast (pp. 1369-1416)
This is a shared conversation. Sign in to Orris to start your own chat.