State the management and prognosis of acute post streptococcal glomerulonephritis.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"post-streptococcal glomerulonephritis" AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive information from both Goldman-Cecil Medicine sources. I now have everything needed to compose a thorough answer.
Management and Prognosis of Acute Post-Streptococcal Glomerulonephritis (APSGN)
Background (Brief)
APSGN is a postinfectious, immune complex-mediated glomerulonephritis following infection by nephritogenic strains of Group A beta-hemolytic streptococci (occasionally Groups C or G). It predominantly affects children aged 2-18 years (M:F = 2:1). The latency period is 7-10 days after throat infection and 2-4 weeks after skin infection.
Management
1. Eradication of Residual Streptococcal Infection
- If streptococcal infection is still present at the time of diagnosis, benzathine penicillin G 1.2 million units IM is administered to:
- Treat the individual
- Prevent spread of the nephritogenic strain to contacts
- This does NOT alter the course of the glomerulonephritis itself but is important for infection control
2. Supportive / Symptomatic Treatment
Treatment is primarily supportive, targeting the two main clinical problems - volume overload and hypertension.
a. Control of Volume Overload (Edema / Oliguria)
- Loop diuretics (e.g., furosemide) - to manage fluid retention and reduce edema
- Salt restriction - dietary sodium restriction to reduce fluid accumulation
b. Control of Hypertension
- Antihypertensive agents as needed, guided by BP severity
- Diuretics also contribute to BP reduction via volume depletion
c. Management of Specific Complications
| Complication | Management |
|---|---|
| Hypertensive encephalopathy | IV antihypertensives (nitroprusside, labetalol) |
| Pulmonary edema / heart failure | IV furosemide, oxygen, fluid restriction |
| Acute kidney injury / azotemia | Monitor electrolytes, restrict potassium/phosphate; dialysis if severe |
| Nephrotic-range proteinuria | Supportive; more common in elderly |
| Rapidly progressive crescentic GN (rare) | Consider corticosteroids / immunosuppression (rare indication) |
3. No Specific Immunosuppressive Therapy
- Steroids and immunosuppressants are not routinely used - the disease is self-limiting in the vast majority
- Renal biopsy is rarely necessary; it should be considered when there is diagnostic uncertainty or the course is atypical (e.g., absence of complement recovery, prolonged azotemia, or nephrotic syndrome without prior infection)
4. Monitoring During Recovery
- Serial urinalysis (hematuria and proteinuria resolve over weeks to months)
- Serum complement C3 levels - should normalize within 6-8 weeks; persistent low C3 beyond 8 weeks suggests an alternative diagnosis (e.g., MPGN, lupus nephritis)
- Blood pressure monitoring
- Renal function tests (BUN, creatinine)
Prognosis
In Children (Excellent)
- Short-term prognosis is excellent
- Acute symptoms (hematuria, edema, hypertension, oliguria) typically resolve within 2-7 days of supportive treatment
- Proteinuria and microscopic hematuria may persist for several months but eventually resolve
- Complete recovery of kidney function in the vast majority
- Long-term progression to end-stage renal disease (ESRD) is uncommon in the absence of other contributing factors
- Recurrence is rare (immunity develops after infection with the nephritogenic strain)
In Adults (Worse Outcomes)
- More serious morbidity can occur, partly due to preexisting cardiovascular and metabolic disease
- Greater likelihood of azotemia, heart failure, and nephrotic-range proteinuria at presentation
- Underlying kidney disease (especially diabetic nephropathy) is associated with a worse prognosis
- Risk of progression to chronic kidney disease is higher than in children
Factors Associated with Worse Prognosis
| Factor | Significance |
|---|---|
| Advanced age | Higher comorbidity burden |
| Preexisting diabetic nephropathy | Reduces renal reserve |
| Heavy proteinuria at presentation | Marker of more severe injury |
| Crescent formation on biopsy | Risk of RPGN course |
| Persistent hypertension | Ongoing renal injury |
| Delayed complement recovery (>8 weeks) | May indicate alternative/superimposed diagnosis |
Long-Term Outlook
- Subclinical disease (microscopic hematuria + low C3 alone) - resolves completely in essentially all cases
- Clinical APSGN in children - near-complete recovery expected
- Clinical APSGN in adults with comorbidities - subset may develop chronic kidney disease or ESRD over years
- Post-streptococcal GN has been identified as a risk factor for chronic kidney disease in long-term follow-up studies, particularly in indigenous/Aboriginal populations with recurrent or severe disease
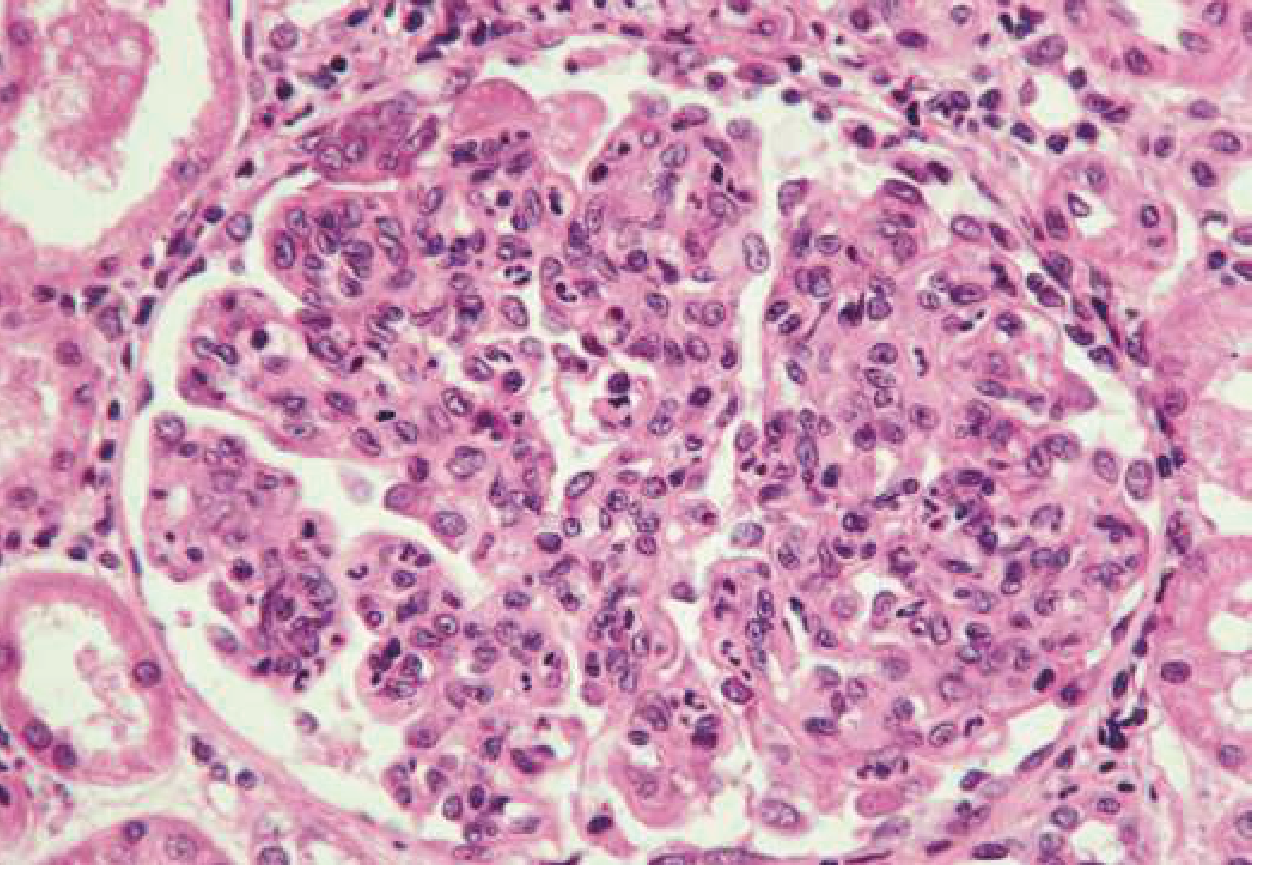
Histology of APSGN: A hypercellular glomerulus densely infiltrated by PMNs. Capillary lumens are compressed. This "endocapillary proliferative" pattern is characteristic.
Sources:
- Goldman-Cecil Medicine, Chapter 269 (Streptococcal Infections - Treatment and Prognosis of PSGN)
- Goldman-Cecil Medicine, Chapter 107 (Glomerular Disorders - Treatment and Prognosis)
- Brenner and Rector's The Kidney (long-term outcomes in adult APSGN)
This is a shared conversation. Sign in to Orris to start your own chat.