Glomus Tumor
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glomus tumor" diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Glomus Tumor
Overview / Classification
A glomus tumor is a benign vascular neoplasm arising from the glomus body - a specialized neuromyoarterial thermoregulatory structure found in the reticular dermis. It functions as a dermal shunt that regulates skin temperature and blood pressure. Glomus cells are modified perivascular smooth muscle cells (round/oval with dense granular cytoplasm).
Robbins classifies glomus tumor as a benign vascular neoplasm composed of non-endothelial vascular wall cells - distinct from hemangiomas which arise from endothelium.
Two major modern subgroups exist:
| Feature | Glomus Tumor (proper) | Glomuvenous Malformation (GVM) |
|---|---|---|
| Old name | Solitary glomus tumor | Glomangioma |
| Age at presentation | Young adults (20-40 years) | Infancy/childhood (often congenital) |
| Number | Solitary | Multiple |
| Symptoms | Severely painful | Generally asymptomatic |
| Sex | Subungual: female > male; non-digital: male > male | No sex predilection |
| Histology | Solid sheets of glomus cells around small vessels | Dilated vessels rimmed by glomus cells |
| Genetics | Sporadic (GLMN somatic mutation suspected) | Autosomal dominant; GLMN germline mutations on chr 1p22.1 |
| Behavior | Benign (rare malignant transformation) | Always benign |
- Dermatology 2-Volume Set 5e (Belousova), p. 2470
- Andrews' Diseases of the Skin, p. 692
Normal Glomus Body Anatomy
The normal glomus body (Sucquet-Hoyer canal) is an encapsulated oval structure in the reticular dermis containing modified smooth muscle cells that dilate upon exposure to cold. It is densest in the subungual tissue, fingertips, and palms - explaining the predilection of glomus tumors for these sites.
Epidemiology
-
Most common in young adults (mean age 46 years; range 18-72)
-
75% subungual in location; up to 25% elsewhere (forearm, palm, foot, rarely visceral sites)
-
Subungual lesions: female predominance (75%)
-
Non-digital lesions: male predominance
-
Extracutaneous sites reported: GI tract, bone, mediastinum, trachea, mesentery, cervix, vagina
-
GVMs account for only 10-20% of all glomus cell lesions
-
Campbell's Operative Orthopaedics 15th Ed 2026, p. 4542
Pathogenesis
- Most tumors likely represent neoplastic proliferations from pre-existing glomus body populations - the subungual region is densely packed with normal glomus bodies
- Occasional occurrences at sites lacking normal glomus bodies (bone, GI tract, nerve) suggest some arise from pluripotent mesenchymal cells or ordinary smooth muscle cells
- Trauma and genetic mutations implicated
- GVMs: germline mutations in GLMN (encodes glomulin, an immunophilin); >40 different mutations identified; glomulin is essential for embryonic vascular development and expressed in vascular smooth muscle
- Association with neurofibromatosis type I (multiple nontender lesions)
Clinical Features
Classic Triad (Subungual / Digital Type)
- Pain - paroxysmal, lancinating, excruciating
- Cold sensitivity - immersion in ice water dramatically exacerbates pain
- Point tenderness - direct pinpoint pressure causes severe radiating pain

Appearance: Small (usually <1 cm, often only a few mm), skin-colored to dusky blue-red firm papule or nodule. Subungual lesions show a bluish tinge through the translucent nail plate. Occasionally nontender variants occur.
Key Clinical Tests
| Test | Description | Positive Finding |
|---|---|---|
| Love test | Point pressure with a blunt object | Excruciating pain at exact tumor site; no pain 1-2 mm away |
| Hildreth test | Tourniquet-induced ischemia of limb | Elimination of pinpoint tenderness under ischemia |
| Cold sensitivity test | Immersion in ice water | Exacerbation of pain |
| Transillumination | Light through finger pad | Red, opaque dot visible |
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 4542-4543
Nonmyelinated nerve fibers intermixed with thick-walled capillaries are responsible for the lancinating pain.
Histopathology
Glomus tumor proper:
- Well-circumscribed proliferation of solid sheets and clusters of uniform glomus cells clustering around capillary-sized, endothelium-lined vessels
- Glomus cells: uniformly rounded/polygonal, centrally placed rounded nuclei, pale eosinophilic cytoplasm
- Stroma: myxoid or hyalinized; may contain small nerve twigs
- Dense fibrous pseudo-capsule may be present
- PAS staining reveals basement membrane material around individual cells
- Mitoses may be present but are normally configured
Immunohistochemistry:
- Vimentin: positive (not desmin - key distinguishing feature from typical smooth muscle)
- Smooth muscle actin (SMA): consistently positive
- Desmin: variably positive
Subtypes:
-
Glomangiomyoma: transition from rounded glomus cells to elongated, well-differentiated smooth muscle cells
-
GVM (glomangioma): dilated venous-type vessels rimmed by only 1-2 layers of glomus cells
-
Dermatology 2-Volume Set 5e, p. 2470; Andrews' Diseases of the Skin, p. 692
Imaging
| Modality | Findings |
|---|---|
| X-ray | Limited utility; subungual tumors may show bony erosion, increased nail-to-phalanx distance |
| MRI (high-Tesla) | Hypointense T1, bright T2 signal (classic); strongly enhancing; method of choice. Note: 33% false-negative rate for small/atypical tumors |
| High-resolution US (5-9 MHz) | Defines tumor limits before surgery |
| Color duplex sonography | Used to map vascularity |
| Contrast CT | Strongly enhancing mass |
For head/neck (paraganglioma type): MRI shows the characteristic "salt-and-pepper" appearance - black flow voids representing enlarged vessels intermixed with enhancing tissue.
Head & Neck Glomus Tumors (Paragangliomas/Chemodectomas)
In the ENT context, "glomus tumor" refers to paragangliomas arising from chemoreceptor tissue (historically called chemodectomas). These are distinct from the cutaneous glomus tumor but share the name.
Glomus Tympanicum
- Small tumor of the middle ear
- Presents with pulsatile tinnitus
- Seen otoscopically as a reddish-blue mass behind the tympanic membrane
- CT differentiates it from glomus jugulare extension (bony plate between jugular foramen and middle ear is intact)
- Usually small enough for surgery without embolization
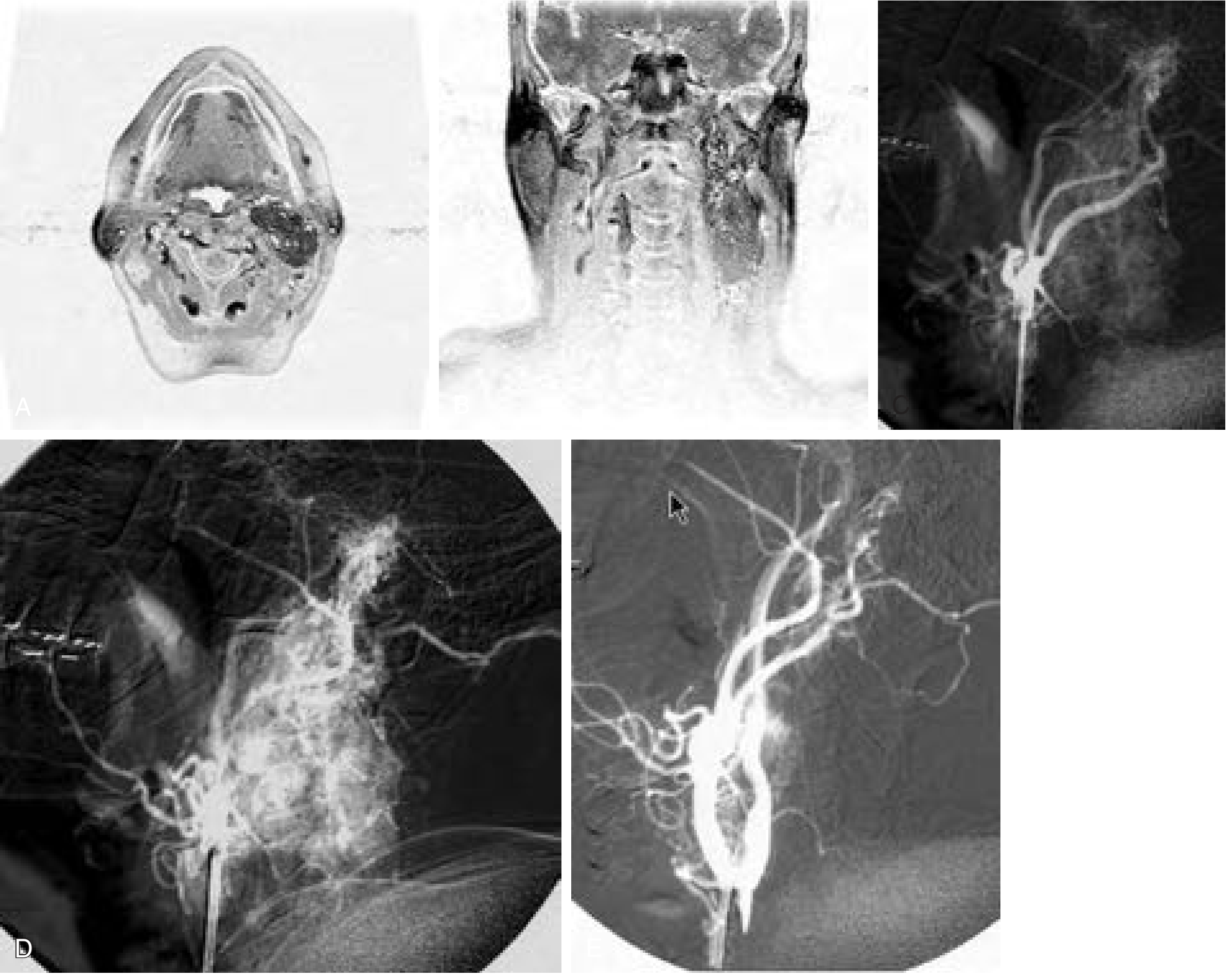
Glomus Jugulare
- Arises in the jugular foramen
- Presents with cranial nerve IX, X, XI dysfunction; if large, CN XII also affected; pulsatile tinnitus
- Extends into: upper neck, middle ear (bone destruction), posterior fossa, around petrous ICA
- Bone destruction can simulate malignancy
- Blood supply: ascending pharyngeal artery + middle meningeal artery (posterior division) most common; also stylomastoid, posterior auricular branches
- Highly vascular - preoperative embolization often required
Glomus Vagale
-
Arises along the vagus nerve in the neck
-
Cummings Otolaryngology Head and Neck Surgery, p. 2616
Malignancy Criteria
The vast majority are benign. Malignant glomus tumor (glomangiosarcoma) is defined by:
- Size >2 cm AND deep location, OR
- Marked nuclear atypia AND high mitotic rate (≥5/50 HPF), OR
- Atypical mitotic figures
If these criteria are met: metastatic rates exceed 25%. Large, deeply located extremity lesions with sarcomatous areas intermingled with benign glomus areas characterize glomangiosarcoma.
- Dermatology 2-Volume Set 5e, p. 2470; Campbell's Operative Orthopaedics 15th Ed 2026, p. 4543
Differential Diagnosis
- Blue nevus (subungual)
- Venous malformation / GVM
- Pyogenic granuloma
- Subungual melanoma
- Hemangioma (cavernous)
- Mucoid cyst
- High jugular bulb (mimics glomus tumor on MRI/otoscopy)
Treatment
Cutaneous / Subungual Glomus Tumor
Complete surgical excision is the treatment of choice and produces immediate, dramatic pain relief.
- Performed under local anesthesia; lesion marked just before surgery
- Meticulous excision of the well-encapsulated lesion
- Subungual approach: nail plate avulsion, then longitudinal (nail bed tumor) or transverse (nail matrix tumor) incision with fine curved scissors
- Nail bed sutured with interrupted absorbable sutures; nail plate returned and secured
- Recurrence rate: ~6.9-12%; reoperation rates 12-24% reported
- Satellite lesions can explain new tumor sites
- No significant difference in outcomes between microscopic and loupe-assisted procedures
Head & Neck Paragangliomas
- Surgery is primary treatment; preoperative embolization for large hypervascular tumors (glomus jugulare)
- Radiation therapy/stereotactic radiosurgery for unresectable or elderly patients
- 2024 meta-analysis (PMID: 38722318) comparing endoscopic vs. microscopic resection of temporal bone paraganglioma shows comparable success and safety profiles
Summary Table
| Feature | Details |
|---|---|
| Origin | Glomus body (Sucquet-Hoyer canal); modified perivascular smooth muscle cells |
| Most common site | Subungual (fingertip), 75% |
| Classic triad | Pain, cold sensitivity, point tenderness |
| Key tests | Love test, Hildreth test |
| Histology | Solid sheets of round glomus cells; vimentin+, SMA+, PAS+ BM |
| Imaging of choice | High-resolution MRI (bright T2) |
| Treatment | Complete surgical excision |
| Malignancy | Rare; >2cm + deep OR marked atypia + high mitoses |
| Genetics (familial) | GLMN mutations, chr 1p22.1, autosomal dominant |
Sources: Andrews' Diseases of the Skin, p. 692 | Dermatology 2-Volume Set 5e | Campbell's Operative Orthopaedics 15th Ed 2026, p. 4542 | Cummings Otolaryngology | Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.