mi
It looks like your message got cut off! Could you finish your thought? What would you like help with?
myocardial infarction
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction" AND "diagnosis"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have excellent clinical content from Harrison's (22nd ed.) and Tintinalli's Emergency Medicine. Here is the full clinical bedside summary:
Myocardial Infarction: Clinical Features & Diagnosis
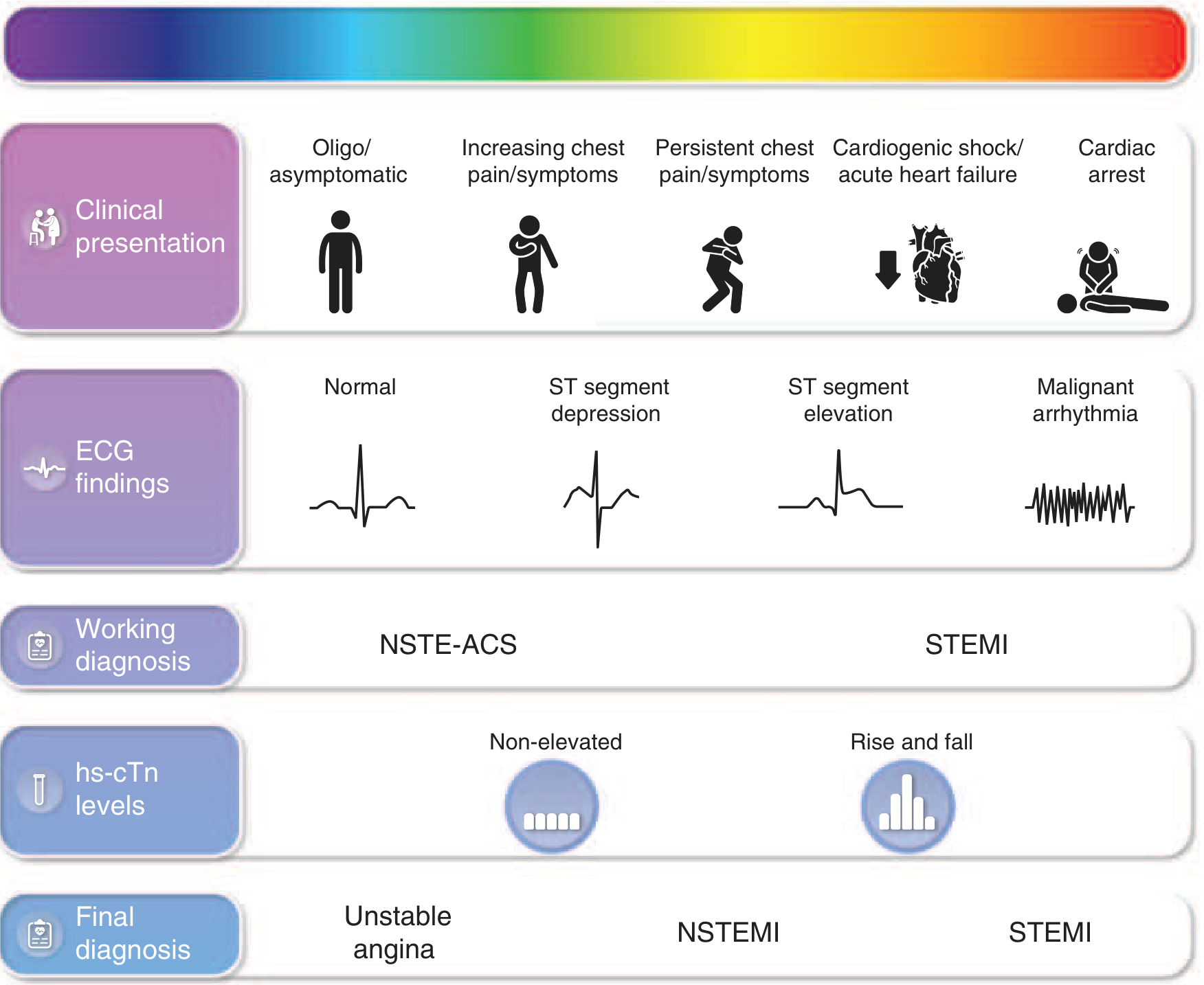
Classification
MI is categorized into two main types based on the presenting ECG:
- STEMI - ST-segment elevation on presenting ECG; reflects transmural injury requiring immediate reperfusion
- NSTEMI - No ST elevation but elevated troponins confirming myocyte necrosis
- Unstable Angina (UA) - Ischemic symptoms without biomarker rise (distinction from NSTEMI increasingly blurred with high-sensitivity troponins)
Clinical Features
Symptoms
The hallmark is chest discomfort - patients often describe it as pressure, heaviness, tightness, fullness, or squeezing rather than sharp pain. Key features:
- Location: Substernal or left chest, radiating to left arm, shoulder, neck, or jaw
- Duration: Prolonged (>10-20 min), unlike stable angina which typically resolves in <10 min with rest
- Little or no relief from sublingual nitroglycerin (in contrast to stable angina)
- Onset: At rest or with minimal exertion
Associated symptoms (especially prominent in acute MI vs. angina):
- Diaphoresis (sweating)
- Nausea and vomiting
- Dyspnea / shortness of breath
- Lightheadedness or syncope
- Palpitations
- Easy fatigability
Atypical presentations are common. Up to 37.5% of women and 27.4% of men present without chest pain. The elderly, women, and diabetics are more likely to present with epigastric pain, jaw pain, fatigue, or vague discomfort. The term "atypical" is misleading since these presentations are frequent. - Tintinalli's Emergency Medicine, 4th ed.
Physical Examination
| Finding | Significance |
|---|---|
| Pale, cyanotic, diaphoretic | Sympathetic activation, poor perfusion |
| Tachycardia | Pain, anxiety, LV dysfunction |
| Bradycardia | More common with inferior wall MI |
| Hypotension | Pump failure or RV infarction |
| S3 gallop (15-20% of AMI) | Suggests failing myocardium |
| New systolic murmur | Papillary muscle dysfunction, MR, or VSD - ominous sign |
| Pulmonary crackles (rales) | Left ventricular dysfunction / pulmonary edema |
| JVD + peripheral edema | Right-sided heart failure (e.g., RV infarction) |
Diagnosis
Diagnosis rests on three pillars: symptoms, ECG, and cardiac biomarkers.
1. ECG
Obtain within 10 minutes of presentation. The 12-lead ECG is the single most important initial test. Key findings:
| MI Location | ECG Leads with ST Elevation |
|---|---|
| Anteroseptal | V1, V2, (V3) |
| Anterior | V1-V4 |
| Anterolateral | V1-V6, I, aVL |
| Lateral | I, aVL |
| Inferior | II, III, aVF |
| Inferolateral | II, III, aVF, V5-V6 |
| Posterior | Tall R waves in V1-V2, R/S ≥ 1 (reciprocal changes) |
| Right ventricular | ST elevation in II, III, aVF + ST elevation in right-sided leads (V3R-V6R) |
- Reciprocal ST depression in leads away from the infarct zone increases diagnostic specificity
- For inferior STEMI, always get right-sided lead V4R to rule out RV infarction
- New LBBB with ischemic symptoms: treat as STEMI equivalent if clinically appropriate
- Initial ECG is non-diagnostic in ~50% of eventual STEMIs - serial ECGs are essential if symptoms persist - Tintinalli's Emergency Medicine
2. Cardiac Biomarkers
- High-sensitivity cardiac troponin (hs-cTn) is the biomarker of choice - detects myocyte necrosis early
- NSTEMI = ischemic symptoms + rise and/or fall of hs-cTn above the 99th percentile URL
- Serial troponins at 0h and 1-3h (0/1h or 0/2h rapid rule-in/rule-out protocols per ESC 2023 guidelines)
- Troponin can be elevated in non-MI causes (myocarditis, PE, sepsis, renal failure) - context matters
- The wider use of hs-cTn is reclassifying many former "unstable angina" cases as NSTEMI
3. TIMI Risk Score (for NSTE-ACS risk stratification)
| Risk Markers | |
|---|---|
| Age ≥65 years | ST deviation >0.5 mm |
| Known CAD (≥50% stenosis) | ≥2 anginal episodes in prior 24h |
| Elevated cardiac markers | Prior aspirin use |
| ≥3 CAD risk factors |
Risk of death/MI/urgent revascularization at 14 days ranges from 5% (0-1 markers) to 41% (6-7 markers). - Harrison's Principles of Internal Medicine, 22nd ed.
Differential Diagnosis - Don't Miss
The physical exam and workup must exclude these life-threatening mimics:
- Aortic dissection (tearing pain radiating to back, BP differential between arms)
- Pulmonary embolism (dyspnea, pleuritic pain, risk factors, ECG may show S1Q3T3)
- Cardiac tamponade (Beck's triad)
- Boerhaave syndrome, tension pneumothorax in appropriate contexts
Key Bedside Pearls
- Cardiac risk factors do not predict ACS at a single moment - they predict CAD over time, not the likelihood of an acute event in the ED
- Up to 30% of acute MI patients are silent - they never seek care or recall symptoms
- A normal initial ECG does not exclude STEMI - repeat ECGs are mandatory with persistent symptoms
- Reproducible chest wall tenderness occurs in some MI patients and does not rule out ACS
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025) | Tintinalli's Emergency Medicine, 9th ed. | Harrison's Chap. 285 NSTE-ACS
This is a shared conversation. Sign in to Orris to start your own chat.