Acute Pancreatitis ,
Acute Pancreatitis , Harrison
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"acute pancreatitis" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Harrison's 22E on Acute Pancreatitis. I have enough material to write an in-depth, well-structured answer. Let me compile it now.
Acute Pancreatitis — Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Epidemiology
Acute pancreatitis is one of the most common principal gastrointestinal diagnoses in the United States, accounting for nearly 300,000 hospitalizations per year. The annual incidence is 15-45 per 100,000 persons, with a median hospital stay of 4 days and an estimated annual cost approaching $3 billion. Mortality is approximately 1% overall, but rises sharply in severe cases. Incidence is rising globally, most prominently in North America and Europe, and is higher among African Americans and increases with age.
Etiology
Gallstones and alcohol account for 80-90% of identified cases in the United States.
Common Causes
| Cause | Details |
|---|---|
| Gallstones (incl. microlithiasis) | Leading cause in most series (30-60%); risk is 4x higher with stones <5 mm |
| Heavy alcohol use | 15-30% of cases; incidence among heavy users is ~5/100,000 |
| Severe hypertriglyceridemia | Major metabolic cause |
| ERCP | Especially after therapeutic intervention |
| Idiopathic | Significant proportion |
Uncommon Causes
- Drugs: azathioprine, 6-mercaptopurine, sulfonamides, estrogens, tetracycline, valproic acid, 5-ASA, DPP4 inhibitors (e.g., sitagliptin)
- Connective tissue disorders and TTP
- Pancreatic cancer
- Hypercalcemia
- Periampullary diverticulum
- Pancreas divisum
- Hereditary pancreatitis
- Cystic fibrosis
- Renal failure
- Infections (mumps, coxsackievirus, CMV, echovirus, parasites)
- Autoimmune pancreatitis (type 1 and 2)
- Trauma (especially blunt abdominal)
- Postoperative
Causes of Recurrent Pancreatitis Without Obvious Etiology
- Occult biliary disease or microlithiasis/biliary sludge
- Drugs
- Hypertriglyceridemia
- Pancreas divisum
- Pancreatic duct strictures
- Ampullary or duodenal abnormalities
- Genetic mutations (PRSS1, SPINK1, CFTR, CTRC, CASR, CLDN2)
- Autoimmune pancreatitis
Pathogenesis
Pancreatitis evolves in three phases:
-
Phase 1 - Intrapancreatic enzyme activation: Lysosomal hydrolases (e.g., cathepsin B) colocalize with digestive enzymes, activating trypsinogen prematurely within the acinar cell. Trypsin activation leads directly to acinar cell injury.
-
Phase 2 - Inflammatory cascade: Leukocytes and macrophages are activated, chemically attracted, and sequestered in the pancreas. Neutrophils can themselves activate trypsinogen (an early neutrophil-independent and a later neutrophil-dependent process).
-
Phase 3 - Systemic effects: Activated proteolytic enzymes (trypsin, elastase, phospholipase A2) and cytokines are released, causing:
- Proteolysis, edema, interstitial hemorrhage, vascular damage
- Fat necrosis and coagulation necrosis
- Release of bradykinin, vasoactive substances, and histamine
- Profound systemic effects: SIRS, ARDS, multi-organ failure
Genetic susceptibility genes: PRSS1 (only one sufficient alone to cause disease), SPINK1, CFTR, CTRC, CASR, and CLDN2. The others act as disease modifiers.
Clinical Features
Symptoms
- Abdominal pain: The dominant symptom. Steady, boring, constant, located in the epigastrium, radiating to the back, chest, flanks, or lower abdomen. Ranges from mild to severe and incapacitating.
- Nausea, vomiting
- Abdominal distension (due to gastric/intestinal hypomotility)
Signs
- Distressed, anxious patient
- Low-grade fever, tachycardia, hypotension
- Shock (from: hypovolemia due to exudation into retroperitoneal space; kinin release; effect of proteolytic enzymes on vascular permeability)
- Abdominal guarding and rigidity
- Decreased/absent bowel sounds (ileus)
- Cullen's sign (periumbilical ecchymosis) - rare, indicates hemorrhagic pancreatitis
- Grey Turner's sign (flank ecchymosis) - rare, same significance
Diagnosis
Laboratory Tests
- Serum amylase: Rises within 6-12 hours, returns to normal in 3-5 days. Sensitivity ~85%; not specific (can be elevated in intestinal obstruction, perforated ulcer, renal failure, salivary gland disease).
- Serum lipase: More specific than amylase; remains elevated longer. Preferred test.
- Elevated amylase + lipase together increases diagnostic accuracy.
- Hematocrit >44% (hemoconcentration): marker of severity.
- BUN >20 mg/dL on admission: associated with increased severity.
- C-reactive protein (CRP) >100 mg/L: elevated in severe disease.
- Leukocytosis, hyperglycemia, hypocalcemia (indicative of fat necrosis), elevated LFTs (if gallstone etiology), elevated triglycerides.
Imaging
- CT scan (contrast-enhanced): The standard for assessing severity, detecting necrosis, and identifying complications. Best performed at 48-72 hours if diagnosis is uncertain or patient is not improving.
- Abdominal ultrasound: First-line to identify gallstones; poor visualization of the pancreas due to bowel gas.
- MRI/MRCP: Alternative to CT, especially to detect biliary stones and ductal anatomy without radiation.
- ERCP: Reserved for suspected choledocholithiasis with cholangitis, not routinely early in acute pancreatitis.
Severity Assessment
Revised Atlanta Classification
| Category | Features |
|---|---|
| Mild | No organ failure, no local or systemic complications |
| Moderately Severe | Transient organ failure (<48 h) and/or local/systemic complications |
| Severe | Persistent organ failure (>48 h), single or multi-organ |
Prognostic Scoring Systems (Table 359-3 in Harrison's)
BISAP Score (Bedside Index of Severity in Acute Pancreatitis) - assessed within first 24 hours:
- (B) BUN >25 mg/dL
- (I) Impaired mental status (Glasgow Coma Scale <15)
- (S) SIRS: ≥2 of 4 criteria present:
- Temp <36°C or >38°C
- Heart rate >90 bpm
- Respirations >20/min or PCO2 <32 mmHg
- WBC >12,000/μL, <4,000/μL, or >10% bands
- (A) Age >60 years
- (P) Pleural effusion on imaging
Score ≥3 = substantially increased in-hospital mortality risk
Other markers of severity:
- APACHE II ≥8 at 24 h
- Hematocrit >44%
- Admission BUN >20 mg/dL
- Organ failure (Modified Marshall Score):
- Cardiovascular: SBP <90 mmHg, HR >130 bpm
- Pulmonary: PaO2 <60 mmHg
- Renal: serum creatinine >2.0 mg/dL
Markers during hospitalization:
- CRP >100 mg/L
- Persistent organ failure (≥48 h)
- Pancreatic or extrapancreatic necrosis
Management
Initial Resuscitation
- Aggressive IV fluid resuscitation is the cornerstone of early management
- Lactated Ringer's (LR) is preferred over normal saline (reduces risk of SIRS)
- A decrease in hematocrit and BUN within the first 12-24 hours confirms adequate resuscitation
- A rising BUN during hospitalization signals inadequate hydration and is associated with higher in-hospital mortality
- A less aggressive strategy may suffice in milder pancreatitis
- Adjustments needed in cardiac, pulmonary, or renal disease
Analgesia
- Adequate pain control is essential; opioids are acceptable
Nutrition
- Mild pancreatitis: Oral feeding can resume when pain and nausea improve and bowel sounds return (often within 24-48 h)
- Severe pancreatitis: Enteral nutrition (via nasojejunal or nasogastric tube) is strongly preferred over parenteral nutrition - it maintains gut mucosal integrity and reduces infectious complications
- Total parenteral nutrition (TPN) is reserved for cases where enteral feeding is not tolerated
NPO (Nothing by Mouth)
- Maintained until pain resolves and oral feeding can be tolerated
Triage / Hospital Admission Level
- BISAP score, hematocrit, and BUN guide triage:
- Low scores + no SIRS at 24h → regular ward
- SIRS present, elevated markers → step-down unit or ICU
Role of ERCP
- Urgent ERCP (within 24 h) is indicated in acute biliary pancreatitis with cholangitis or persistent biliary obstruction
- Not indicated routinely in mild gallstone pancreatitis without obstruction
Antibiotics
- Not routinely indicated in acute pancreatitis
- Indicated only when infected pancreatic necrosis is confirmed or strongly suspected (fine-needle aspiration with Gram stain/culture, or CT-guided)
- Prophylactic antibiotics do NOT prevent infection of pancreatic necrosis
Management of Gallstone Pancreatitis
- Cholecystectomy should be performed during the same admission (or soon after) in mild gallstone pancreatitis to prevent recurrence
Complications
Local Complications
| Complication | Description |
|---|---|
| Acute peripancreatic fluid collections | Early (<4 weeks), no defined wall |
| Pancreatic pseudocyst | Fluid collection with fibrous wall, >4 weeks |
| Acute necrotic collection | Contains necrotic tissue, no wall |
| Walled-off necrosis (WON) | Mature encapsulated necrosis, >4 weeks - can be drained endoscopically |
| Infected necrosis | Highest mortality; requires drainage (endoscopic, percutaneous, or surgical) |
Systemic Complications
- ARDS, SIRS, multi-organ failure
- Pleural effusion (usually left-sided)
- Acute kidney injury
- Hemorrhage
- Hypocalcemia (saponification of fat)
- Hyperglycemia
- Disseminated intravascular coagulation (DIC)
Recurrent Acute Pancreatitis
- Defined as two or more documented episodes
- Workup should include: repeat ultrasound, MRCP to evaluate ductal anatomy, EUS to detect microlithiasis, serum triglycerides, calcium, IgG4, genetic testing
- Around 25% of patients previously labeled idiopathic may have an underlying genetic predisposition
Key Points Summary
| Feature | Detail |
|---|---|
| Most common causes | Gallstones (30-60%), Alcohol (15-30%) |
| Best initial test | Serum lipase + amylase |
| Best severity score | BISAP (≥3 = severe) |
| Preferred IV fluid | Lactated Ringer's |
| Preferred nutrition (severe) | Enteral (nasojejunal) > TPN |
| Antibiotics | Only for infected necrosis |
| ERCP indication | Cholangitis / persistent obstruction only |
| Cholecystectomy | Same admission in mild gallstone pancreatitis |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 359 - Diseases of the Pancreas
Rheumatic fever
Reading File
Finding Sources
Searching PubMed
"rheumatic fever" AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have rich content on ARF from Harrison's 22E. I have the global considerations, epidemiology, pathogenesis, and the start of clinical features and management. The content I collected from earlier reads (lines 2142-2390) covered management in detail. I have everything needed for a comprehensive response. Let me now compile it.
Acute Rheumatic Fever (ARF)
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Definition
Acute Rheumatic Fever (ARF) is a multisystem inflammatory disease resulting from an autoimmune reaction to infection with Group A Streptococcus (GAS). While most manifestations resolve completely, the major exception is cardiac valvular damage (Rheumatic Heart Disease - RHD), which can persist long after the acute illness resolves.
Global Considerations
ARF and RHD are fundamentally diseases of poverty. Their incidence declined in high-income countries during the early 20th century due to:
- Improved living conditions (less crowded housing, better hygiene)
- Reduced GAS transmission
- Antibiotic availability and improved medical systems
However, this decline has not been replicated in low- and middle-income countries (LMICs). Key global facts:
- >40 million people worldwide affected by RHD
- >300,000 deaths per year attributable to RHD
- 95% of ARF cases and RHD deaths occur in developing countries
- Highest burden: sub-Saharan Africa, Pacific nations, Australasia, China, South and Central Asia
- RHD is the most common cause of acquired heart disease in children in LMICs
- WHO adopted a Global Resolution on RF and RHD in 2018
Epidemiology
- Primarily a disease of children aged 5-14 years
- Initial episodes are rare after age 30
- Recurrent episodes remain common in adolescents and young adults
- No clear gender association for ARF, but RHD affects females more (up to 2x more frequently than males)
- RHD prevalence peaks between 25-40 years of age
Pathogenesis
Organism Factors
- Caused by Group A Streptococcus (GAS) pharyngeal infection
- Certain M-serotypes (particularly types 1, 3, 5, 6, 14, 18, 19, 24, 27, 29) are classically "rheumatogenic"
- GAS skin infections are generally not considered a trigger for ARF (unlike post-streptococcal glomerulonephritis)
Host Factors
- Only a small proportion (~3%) of individuals develop ARF after GAS pharyngitis
- Susceptibility is partly genetic (familial clustering)
- HLA class II antigens play a role in predisposition
Autoimmune Mechanism - Molecular Mimicry
The central mechanism is molecular mimicry:
- GAS surface proteins (particularly M protein) share structural similarity with human cardiac proteins (myosin, laminin, tropomyosin, vimentin)
- Antibodies generated against GAS cross-react with cardiac tissue
- This leads to valvular endocarditis, myocarditis, and pericarditis
- T-cell mediated immunity also contributes to cardiac injury
- This explains why carditis tends to be the most dangerous long-term manifestation
Clinical Features - The Jones Criteria (Revised 2015)
The revised Jones Criteria are used for diagnosis, stratified by epidemiologic risk:
Major Criteria
| Major Criterion | Features |
|---|---|
| Carditis | Clinical (auscultatory) and/or subclinical (echocardiographic); pancarditis (endo-, myo-, pericarditis); mitral and aortic valves most commonly affected |
| Arthritis | Migratory polyarthritis in high-risk populations; monoarthritis or polyarthritis in low-risk populations; typically large joints (knees, ankles, elbows, wrists); exquisitely tender, responds dramatically to aspirin |
| Chorea (Sydenham's) | Involuntary, purposeless, non-rhythmic movements; emotional lability; muscle weakness; may occur in isolation weeks-months after streptococcal infection |
| Erythema marginatum | Non-pruritic, evanescent, macular rash with central clearing; pink/red margins; found on trunk and proximal extremities (not face) |
| Subcutaneous nodules | Firm, painless nodules over bony prominences (elbows, knees, wrists, occiput); associated with severe carditis |
Minor Criteria
| Minor Criterion | Details |
|---|---|
| Fever | ≥38.5°C |
| Elevated ESR | ≥60 mm/h (high-risk); ≥30 mm/h (low-risk) |
| Elevated CRP | ≥3.0 mg/dL |
| Prolonged PR interval | On ECG (does not count if carditis is a major criterion) |
| Polyarthralgia | Only if arthritis is not used as a major criterion |
| Monoarthralgia | Only in high-risk populations if arthritis not used |
Evidence of Preceding GAS Infection (Required)
- Elevated or rising antistreptolysin O (ASO) titer
- Elevated anti-DNase B
- Positive throat culture for GAS
- Positive rapid GAS antigen test
Diagnostic Rule
≥2 major OR 1 major + 2 minor criteria, PLUS evidence of preceding GAS infection = ARF diagnosis
Exception: Chorea alone, or indolent carditis alone, may be sufficient for diagnosis without fulfilling the full Jones Criteria.
Carditis (Rheumatic Carditis)
The most important manifestation due to its long-term consequences:
- Occurs in ~50-60% of first ARF episodes
- Pancarditis - all three layers may be involved:
- Endocarditis: most clinically significant; valvulitis causes valvular regurgitation (mitral > aortic)
- Myocarditis: can cause heart failure and cardiomegaly
- Pericarditis: friction rub, chest pain, effusion
- Subclinical carditis: detected only on echocardiography (no murmur audible)
- Pathological finding: Aschoff bodies - granulomatous lesions with central fibrinoid necrosis surrounded by lymphocytes and Aschoff giant cells (pathognomonic)
- Mitral regurgitation is the most common valvular lesion acutely; mitral stenosis develops with repeated attacks over years
Arthritis
- The most common major manifestation (~75% of cases)
- Migratory polyarthritis: moves from joint to joint over days
- Large joints preferentially affected: knees, ankles, hips, wrists, elbows
- Exquisitely painful - often disproportionate to visible signs
- Responds dramatically and completely to salicylates/NSAIDs (failure to respond should question the diagnosis)
- No permanent joint damage
Sydenham's Chorea
- Occurs in 10-30% of cases
- Latency: may appear 1-6 months after GAS infection (longest latent period of all manifestations)
- Features: involuntary, non-rhythmic, purposeless movements; emotional lability; speech disturbance; muscle hypotonia
- Often occurs in isolation without other ARF manifestations
- Resolves spontaneously over weeks to months
Laboratory and Investigations
Always perform:
- ECG (prolonged PR interval)
- Echocardiogram (all suspected cases - to assess subclinical carditis and establish baseline severity)
- CBC (leukocytosis)
- CRP (elevated)
- ASO and anti-DNase B (streptococcal serology)
In relevant situations:
- Throat/skin swab culture
- Blood cultures
- Synovial fluid aspirate
- Autoantibodies (to exclude lupus, JIA)
- Pregnancy test
- Creatinine (before NSAID use)
- Serologic testing to exclude viral arthritis, Yersinia, parvovirus B19, gonorrhea
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Septic arthritis | Monoarticular, fever, joint fluid purulent |
| Juvenile idiopathic arthritis | Chronic, no streptococcal link |
| Reactive arthritis (post-GI/GU) | Asymmetric, may have urethritis/conjunctivitis |
| Gonococcal arthritis | Sexually active, urethritis, skin lesions |
| Systemic lupus erythematosus | Autoantibodies, multi-organ |
| Infective endocarditis | Blood culture positive, vegetations |
| Viral arthritis | Parvovirus B19, rubella |
Management
1. Antibiotics (Eradication of GAS)
- All patients receive antibiotics to eradicate the precipitating streptococcal infection
- Drug of choice: Penicillin
- Oral: Phenoxymethylpenicillin (Penicillin V)
- Parenteral: Single IM injection of benzathine penicillin G
- Penicillin allergy: Erythromycin or a narrow-spectrum cephalosporin
- Note: This treats the initial infection but does NOT alter the course of ARF or prevent RHD
2. Anti-inflammatory Therapy (Symptomatic)
There is no treatment proven to alter the likelihood or severity of RHD development. Treatment is symptomatic.
| Manifestation | Treatment |
|---|---|
| Arthritis | Aspirin (high-dose) or NSAIDs - dramatic response expected; taper over 4-6 weeks |
| Carditis (mild-moderate) | Aspirin or NSAIDs; add corticosteroids for moderate-severe |
| Carditis (severe/heart failure) | Prednisone (corticosteroids) - may be lifesaving; start at 1-2 mg/kg/day, taper over 2-3 weeks |
| Chorea | Symptomatic: haloperidol, carbamazepine, or valproate; also corticosteroids may help |
| Heart failure | Diuretics, ACE inhibitors, digoxin as appropriate |
3. Bed Rest
- Recommended during acute phase, especially with carditis
- Duration depends on severity
4. Secondary Prophylaxis (Most Critical Long-Term Intervention)
Secondary prophylaxis prevents recurrent ARF attacks, which are the major driver of cumulative valvular damage.
Drug of choice: Benzathine penicillin G 1.2 million units IM every 3-4 weeks
- Most effective regimen (superior to oral therapy due to compliance)
- Oral alternative: Penicillin V 250 mg twice daily
Duration of secondary prophylaxis:
| Cardiac Status | Duration |
|---|---|
| No carditis | 5 years after last episode OR until age 21, whichever is longer |
| Carditis (no residual RHD) | 10 years OR until age 21, whichever is longer |
| Residual RHD (mild) | 10 years OR until age 40, whichever is longer |
| Severe RHD / valve surgery | Lifelong |
A 2024 Cochrane systematic review (PMID 39312290) on long-term antibiotic prophylaxis confirmed benefit in preventing recurrence and progression to RHD, supporting current guideline recommendations.
5. ARF Registry and Health Education
- All confirmed/possible cases should be registered in an ARF/RHD registry
- Health education for patients and families on streptococcal infection recognition, sore throat treatment, and prophylaxis compliance
Complications and Long-term Consequences
Rheumatic Heart Disease (RHD)
- The only manifestation with permanent sequelae
- Results from repeated ARF attacks causing progressive valvular scarring and deformity
- Mitral stenosis is the classic late lesion (leaflet fusion, subvalvular fibrosis, calcification)
- Other lesions: mitral regurgitation, aortic regurgitation, aortic stenosis, tricuspid involvement
- Complications: atrial fibrillation, thromboembolic events, pulmonary hypertension, heart failure, infective endocarditis
- Surgical or transcatheter intervention (valvuloplasty, valve replacement) may ultimately be required
Key Summary Points
| Feature | Detail |
|---|---|
| Etiology | GAS pharyngitis → autoimmune (molecular mimicry) |
| Age group | Children 5-14 years most commonly |
| Diagnosis | Revised Jones Criteria 2015 |
| Most common manifestation | Arthritis (~75%) |
| Most dangerous manifestation | Carditis → RHD |
| Pathognomonic lesion | Aschoff body |
| Arthritis treatment | High-dose aspirin/NSAIDs |
| Severe carditis treatment | Corticosteroids (prednisone) |
| Chorea onset | Delayed by 1-6 months after strep |
| Secondary prophylaxis drug | Benzathine penicillin G IM every 3-4 weeks |
| Prophylaxis duration (severe RHD) | Lifelong |
📌 Recent Evidence Note: A 2024 Cochrane meta-analysis (PMID 39312290) on long-term antibiotic prophylaxis confirmed that regular benzathine penicillin G reduces ARF recurrence and RHD progression, reinforcing current guideline-based recommendations.
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 371 - Acute Rheumatic Fever
Bronchial Asthma (CF & RX)
Reading File
Finding Sources
Finding Sources
Searching PubMed
"asthma"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Harrison's 22E on Asthma - pathophysiology, clinical features, diagnosis, classification, treatment (stepwise), medications, and special situations. Let me compile the full structured response.
Bronchial Asthma - Clinical Features & Treatment
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Definition
Asthma is a chronic inflammatory disease of the airways characterized by:
- Episodic and variable airflow obstruction (often reversible)
- Airway hyperresponsiveness (AHR) to various stimuli
- Underlying airway inflammation (predominantly eosinophilic/type 2 in classic atopic asthma)
- Airway remodeling with structural changes over time
Epidemiology & Risk Factors
Exposures and risk factors that can lead to asthma development:
- Allergen exposure in those with a predisposition to atopy
- Occupational exposures (isocyanates, animal dander, flour, latex)
- Air pollution (particulate matter, ozone, NO2)
- Infections (viral - especially rhinovirus, RSV; Mycoplasma)
- Tobacco (active and passive smoking)
- Obesity
- Diet (low antioxidants, high omega-6)
- Fungi in allergic airway mycoses
- Acute irritants (reactive airway dysfunction syndrome - RADS)
- High-intensity exercise in elite athletes
Pathophysiology
Three Core Mechanisms of Airway Obstruction
1. Airway Hyperresponsiveness (AHR)
- Hallmark of asthma
- Defined as an exaggerated narrowing response of airways to stimuli (methacholine, histamine, allergens, cold air, exercise) that don't cause obstruction in normal individuals
- Component occurs at the level of airway smooth muscle itself
- In many patients, AHR is due to mucosal inflammation and remodeling reducing the threshold for smooth muscle activation
2. Acute Airway Narrowing (Bronchoconstriction)
- Triggers (allergens, irritants, exercise, drugs - see below) activate mast cells and other inflammatory cells
- Release of histamine, leukotrienes, prostaglandins → acute smooth muscle contraction
- Neurogenic mechanisms also contribute (parasympathetic, sensory neuropeptides)
3. Chronic Airway Inflammation and Remodeling
- Leads to persistent symptoms and fixed airflow obstruction
- Airway remodeling components:
- Subepithelial fibrosis (reticular basement membrane thickening)
- Airway smooth muscle hypertrophy and hyperplasia
- Mucus gland hyperplasia → mucus hypersecretion and mucus plugging
- Angiogenesis
- Epithelial goblet cell metaplasia
Inflammatory Cells and Mediators
Type 2 (T2) Inflammation (classic allergic/eosinophilic asthma):
| Cell / Mediator | Role |
|---|---|
| Th2 cells and ILC2s | Drive type 2 inflammatory cascade |
| IL-4 | IgE class switching; promotes Th2 differentiation |
| IL-5 | Eosinophil survival, activation, and recruitment |
| IL-13 | Mucus hypersecretion, airway hyperresponsiveness, subepithelial fibrosis |
| IgE / Mast cells | Allergen binding → degranulation → histamine, leukotrienes, PGD2 |
| Eosinophils | Tissue damage via major basic protein, eosinophil peroxidase |
| TSLP, IL-25, IL-33 | Epithelial "alarm signals" that activate ILC2s and mast cells |
Non-Type 2 Inflammation (neutrophilic/obese asthma):
- Driven by IL-6, IL-17, TNF-α, IL-1β, IL-8
- Associated with obesity, smoking, late-onset asthma, and poor steroid response
Fatty Acid Mediators:
- Cysteinyl leukotrienes (LTC4, LTD4, LTE4): produced by eosinophils and mast cells; potent bronchoconstrictors; promote mucus secretion, vascular leakage, and inflammatory cell recruitment - targeted by leukotriene modifiers
- Prostaglandin D2 (PGD2): produced by mast cells; activates CRTH2 receptors on type 2 cells, upregulating inflammation
- LTB4: potent neutrophil chemoattractant
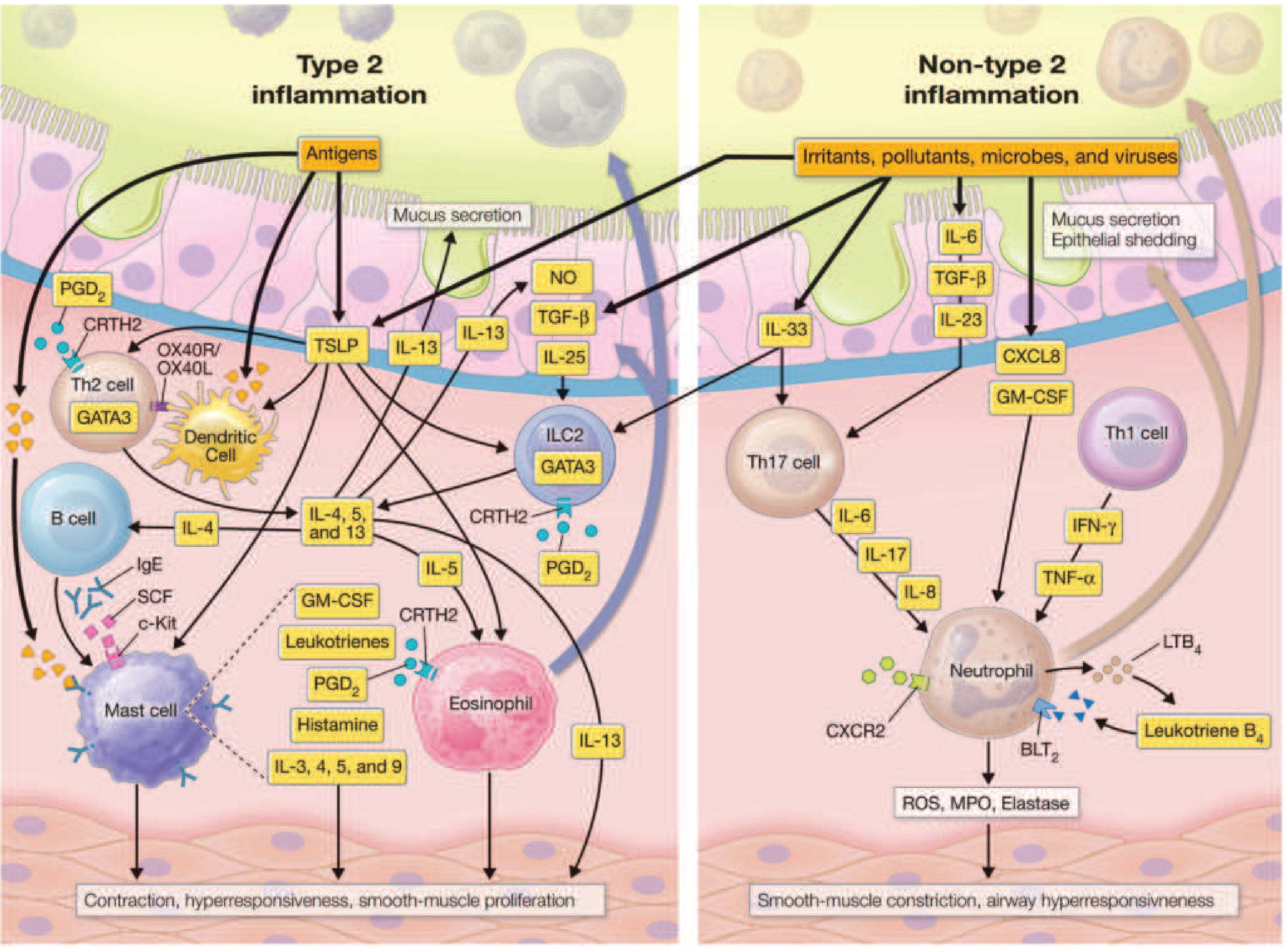
Type 2 and non-type 2 inflammatory pathways in asthma
Triggers of Airway Narrowing
| # | Trigger |
|---|---|
| 1 | Allergens (dust mites, pollen, animal dander, cockroach, molds) |
| 2 | Irritants (smoke, fumes, strong odors, cleaning products) |
| 3 | Viral respiratory infections (rhinovirus most common) |
| 4 | Exercise and cold, dry air |
| 5 | Air pollution |
| 6 | Drugs: NSAIDs/aspirin (aspirin-exacerbated respiratory disease - AERD), beta-blockers, ACE inhibitors |
| 7 | Endocrine factors (menstruation, pregnancy, thyroid disease) |
| 8 | Emotional stress |
Clinical Features
Symptoms
- Episodic wheezing (expiratory, sometimes audible)
- Dyspnea / shortness of breath - variable, episodic
- Chest tightness
- Cough (especially nocturnal and early morning; can be the sole symptom in cough-variant asthma)
- Symptoms are often worse at night and in the early morning (circadian variation in airway tone)
- Symptoms triggered by known precipitants
Signs
- Expiratory wheeze on auscultation (may be absent at rest)
- Prolonged expiratory phase
- Hyperinflation (increased anteroposterior diameter, hyper-resonant percussion) in severe/chronic disease
- Accessory muscle use during acute attack
- Pulsus paradoxus (>10 mmHg drop in systolic BP during inspiration) in severe attack
- Silent chest = ominous sign in acute severe asthma (no wheeze due to minimal airflow)
Features Suggesting Severity of Acute Attack
| Feature | Mild-Moderate | Severe | Life-Threatening |
|---|---|---|---|
| Speech | Full sentences | Phrases | Words only |
| Posture | Can lie down | Prefers sitting | Hunched forward |
| Wheeze | Present | Loud | Silent chest |
| RR | Increased | >25/min | >30/min |
| HR | <100 | 100-120 | >120 or bradycardia |
| SpO2 | >94% | 90-94% | <90% |
| PEF | >50% predicted | 33-50% | <33% ("near-fatal") |
| PaCO2 | Low/normal | Normal rising | Elevated (impending resp failure) |
Diagnosis and Evaluation
Clinical Diagnosis
- Compatible history of recurrent wheezing, dyspnea, chest tightness, or cough related to known precipitants
- Confirmed with pulmonary function testing (PFT) or demonstration of AHR
Pulmonary Function Tests
Spirometry:
- Obstructive pattern: FEV1/FVC ratio < 0.70
- Reversibility: ≥12% AND ≥200 mL improvement in FEV1 after inhaled bronchodilator (albuterol) - confirms asthma diagnosis
- Lung volumes: air trapping (increased RV and TLC) in severe disease
Bronchoprovocation Testing (Methacholine Challenge):
- Used when spirometry is normal but asthma is suspected
- Positive if FEV1 falls ≥20% at a methacholine concentration of ≤8 mg/mL (PC20)
- High sensitivity (~95%), lower specificity - a negative test effectively rules out asthma
Peak Expiratory Flow (PEF):
- Serial home PEF monitoring: diurnal variation >20% supports asthma diagnosis
- Useful for monitoring and guiding treatment adjustments
Additional Evaluation
- Fractional exhaled nitric oxide (FeNO): marker of eosinophilic airway inflammation; elevated (>25 ppb) supports type 2 asthma; guides ICS dosing
- Blood eosinophil count and serum IgE: assess atopy and eligibility for biologics
- Allergy skin testing / RAST (specific IgE): identify allergen sensitization
- CXR: usually normal; may show hyperinflation; rules out pneumothorax, infiltrate
- Sinus CT: if chronic rhinosinusitis suspected
- Induced sputum eosinophils (if available)
Differential Diagnosis
| Condition | Key Features |
|---|---|
| COPD | >40 years, smoker, minimal reversibility |
| Vocal cord dysfunction (ILO) | Inspiratory stridor, laryngoscopy confirms |
| Heart failure | Bilateral crackles, elevated BNP, orthopnea |
| Foreign body aspiration | Unilateral wheeze, sudden onset |
| Bronchiectasis | Chronic productive cough, CT shows dilated bronchi |
| Endobronchial tumor | Monophonic wheeze, no bronchodilator response |
| Eosinophilic granulomatosis (EGPA) | Neuropathy, sinusitis, ANCA positivity |
Comorbidities That Make Asthma Difficult to Control
- Chronic rhinosinusitis ± nasal polyposis
- Obesity
- Gastroesophageal reflux disease (GERD)
- Inducible laryngeal obstruction (vocal cord dysfunction)
- COPD (asthma-COPD overlap)
- Anxiety/depression
- Obstructive sleep apnea
Classification of Asthma Severity
GINA Phenotypic Classification (also NAEPP steps):
| Severity | Symptoms | Nighttime | FEV1 % predicted | PEF variability |
|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2x/month | ≥80% | <20% |
| Mild persistent | >2 days/week but not daily | 3-4x/month | ≥80% | 20-30% |
| Moderate persistent | Daily | >1x/week | 60-80% | >30% |
| Severe persistent | Continuous | Frequent (7x/week) | <60% | >30% |
Treatment
Goals of Therapy (GINA/NAEPP)
- Achieve and maintain symptom control (minimal/no daytime or nocturnal symptoms)
- Prevent exacerbations (reduce frequency and severity)
- Maintain normal lung function (FEV1/FVC near normal)
- Maintain normal activity level (including exercise)
- Minimize side effects of medications
1. Reducing Triggers
- Remove occupational exposures where possible (may lead to resolution)
- Allergen mitigation (impermeable mattress/pillow covers, pet removal, pest control)
- Eliminate secondhand smoke and cannabis combustion products
- Flu vaccine (yearly), pneumococcal vaccine, COVID-19 and RSV vaccines
- Allergen immunotherapy: evidence supports use in mild-moderate atopic asthma under control; reduces IgE-mediated responses
2. Medications
A. Reliever (Rescue) Medications
Short-Acting β2-Agonists (SABA)
- E.g., albuterol (salbutamol), levalbuterol, terbutaline
- Mechanism: activate β2-receptors on smooth muscle → cAMP → smooth muscle relaxation
- Onset: 5-15 minutes; duration: 4-6 hours
- Use: on-demand relief of acute bronchospasm; pre-exercise prophylaxis
- Risk: regular use → tachyphylaxis of bronchoprotective effect; potential for increased airway reactivity with Arg/Arg polymorphism at codon 16 of β2-receptor
- GINA now recommends ICS/formoterol as preferred reliever at all steps (Anti-Inflammatory Reliever - AIR strategy) due to evidence it reduces severe exacerbations compared to SABA alone
ICS/Formoterol as Reliever (AIR Strategy - GINA)
- Combination of ICS + fast-onset LABA (formoterol) used as-needed
- Provides both anti-inflammatory and bronchodilator effects with each puff
- Reduces exacerbation risk even in mild asthma (Step 1)
- NAEPP recommends ICS/formoterol as reliever at Steps 3-4
ICS/SABA Combination (New - US)
- Recently introduced in the US as an alternative anti-inflammatory reliever
B. Controller (Maintenance) Medications
Inhaled Corticosteroids (ICS) - Cornerstone of controller therapy
- E.g., budesonide, fluticasone, beclomethasone, ciclesonide, mometasone
- Mechanism: bind glucocorticoid receptors → reduce transcription of inflammatory cytokines (IL-4, IL-5, IL-13); reduce eosinophilic inflammation; decrease AHR
- Effect: reduce symptoms, exacerbations, and airway remodeling over time
- Side effects: oral candidiasis (use spacer, rinse mouth), dysphonia, adrenal suppression at high doses, osteoporosis with long-term use
- Dose categories: low, medium, high (vary by drug - e.g., budesonide low = 200-400 mcg/day, high = >800 mcg/day)
Long-Acting β2-Agonists (LABA)
- E.g., salmeterol, formoterol, vilanterol, indacaterol
- Duration: 12-24 hours
- Must NOT be used as monotherapy in asthma (black box warning in US) - only as add-on to ICS
- ICS/LABA combination = cornerstone of Steps 3-5 therapy
- Formoterol has rapid onset (can serve as both controller and reliever - SMART/MART strategy)
Leukotriene Modifiers
- Leukotriene Receptor Antagonists (LTRAs): montelukast, zafirlukast
- Block cysteinyl leukotriene receptors (CysLT1)
- Reduce bronchospasm, mucus secretion, and eosinophilic inflammation
- Alternative to low-dose ICS in Step 2 (mild persistent)
- Particularly useful in: aspirin-exacerbated disease (AERD), exercise-induced asthma, allergic rhinitis comorbidity
- ⚠️ FDA warning (2020): montelukast associated with serious neuropsychiatric effects including suicidal ideation - use with caution
- 5-Lipoxygenase inhibitor: zileuton - reduces leukotriene synthesis; requires liver function monitoring
Long-Acting Anticholinergics (LAMA)
- E.g., tiotropium (18 mcg/day inhaled)
- Mechanism: block muscarinic M3 receptors → reduce bronchoconstriction and mucus secretion
- Role: add-on therapy at Steps 4-5; particularly useful in asthma-COPD overlap and those with significant cholinergic triggers
- Improves FEV1 and reduces exacerbations when added to ICS/LABA
Theophylline
- Mechanism: phosphodiesterase inhibitor → increases cAMP → bronchodilation; also has mild anti-inflammatory and immunomodulatory effects
- Narrow therapeutic index: target serum level 5-15 mcg/mL
- Side effects: nausea, headache, tachyarrhythmia, seizures at toxic levels; multiple drug interactions
- Role: rarely used today; considered an add-on option in Step 4-5 when biologics unavailable; requires serum level monitoring
C. Biologic (Targeted) Therapies - Step 5
Used in severe uncontrolled asthma with type 2 inflammation (eosinophilic and/or allergic phenotype) despite high-dose ICS/LABA:
| Biologic | Target | Indication | Notes |
|---|---|---|---|
| Omalizumab | Anti-IgE | Allergic asthma, serum IgE 30-700 IU/mL | SC injection every 2-4 weeks; reduces exacerbations and ICS use |
| Mepolizumab | Anti-IL-5 | Severe eosinophilic asthma (eos ≥150/μL) | SC injection monthly |
| Reslizumab | Anti-IL-5 | Severe eosinophilic asthma (eos ≥400/μL) | IV infusion; higher eos threshold |
| Benralizumab | Anti-IL-5Rα | Severe eosinophilic asthma | SC monthly x3, then every 8 weeks; depletes eosinophils directly |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 + IL-13) | Severe eosinophilic asthma; also nasal polyposis | SC biweekly; broadest type 2 blocker |
| Tezepelumab | Anti-TSLP | Severe asthma (any phenotype, including low eos) | Broadest biologic; works upstream of type 2 cascade |
Biomarkers guiding biologic selection:
- Blood eosinophils (≥150-300/μL → IL-5 pathway agents)
- Total serum IgE + sensitization → omalizumab
- FeNO >25 ppb → type 2 inflammation, supports ICS/biologic response
- TSLP → tezepelumab (works regardless of eosinophil count)
D. Systemic Corticosteroids
- Oral prednisone (30-50 mg/day for 5-7 days) for moderate-severe exacerbations
- IV methylprednisolone for acute severe exacerbations requiring hospitalization
- Minimize long-term systemic use due to adrenal suppression, osteoporosis, diabetes, weight gain, cataracts
3. Stepwise Management (GINA/NAEPP Adapted)
| Step | Preferred Controller | Preferred Reliever | Notes |
|---|---|---|---|
| Step 1 (Intermittent) | None (or as-needed ICS/formoterol) | ICS/formoterol as-needed OR SABA | GINA recommends ICS/formoterol at all steps |
| Step 2 (Mild persistent) | Low-dose ICS | ICS/formoterol OR SABA | LTRA as alternative to ICS (montelukast warning) |
| Step 3 (Moderate persistent) | Low-dose ICS/LABA | ICS/formoterol (MART) | Medium-dose ICS as alternative |
| Step 4 (Moderate-severe persistent) | Medium-high dose ICS/LABA | ICS/formoterol (MART) | Add LAMA (tiotropium); evaluate for biologics |
| Step 5 (Severe uncontrolled) | High-dose ICS/LABA + LAMA | ICS/formoterol | Add biologic (see table above); consider low-dose oral steroid as last resort |
MART strategy = Maintenance And Reliever Therapy: same ICS/formoterol inhaler used for both daily maintenance AND as-needed relief
Key GINA 2025 update: As-needed ICS/formoterol is recommended as the reliever at all steps, including Step 1 (intermittent asthma), replacing SABA monotherapy as preferred reliever due to reduced severe exacerbation risk.
4. Management of Acute Asthma Attack
Mild-Moderate Attack:
- SABA (albuterol) via MDI + spacer: 4-8 puffs every 20 minutes x 3 doses, then reassess
- Or nebulized albuterol 2.5 mg every 20 min x 3
- Oral prednisolone 40-50 mg/day if not responding quickly
- Supplemental oxygen to maintain SpO2 ≥94%
- Monitor PEF, SpO2, RR, HR
Severe Attack (hospital setting):
- Continuous nebulized SABA or high-dose MDI with spacer
- Ipratropium bromide (SAMA) added to albuterol (reduces hospitalizations - synergistic bronchodilation)
- IV methylprednisolone 40-80 mg/day or oral prednisolone
- Supplemental O2 (target SpO2 93-95%)
- IV magnesium sulfate 2 g over 20 minutes - causes smooth muscle relaxation; recommended for acute severe asthma (Evidence: 2024 meta-analysis [PMID 38395640] confirms benefit in children)
- Heliox (helium-oxygen mixture) - reduces work of breathing in near-fatal asthma
Life-Threatening / Near-Fatal:
- Intensive care admission
- IV bronchodilators (terbutaline, salbutamol)
- Non-invasive ventilation (NIV/BiPAP) in selected cases
- Mechanical ventilation: last resort; risk of dynamic hyperinflation (auto-PEEP)
- Ketamine anesthesia - has bronchodilator properties
Discharge criteria: PEF >60-70% predicted, SpO2 >94%, symptoms improved
5. Special Considerations
Aspirin-Exacerbated Respiratory Disease (AERD/Samter's Triad):
- Triad: asthma + nasal polyposis + NSAID/aspirin sensitivity
- Mechanism: COX-1 inhibition → shunting of arachidonic acid to leukotriene pathway → massive bronchoconstriction
- Treatment: avoid NSAIDs; leukotriene modifiers are particularly effective; aspirin desensitization in select cases
Exercise-Induced Bronchoconstriction (EIB):
- Cold, dry air during exercise triggers bronchospasm 5-15 min after exercise
- Prevention: pre-exercise SABA (or ICS/formoterol); warm-up; LTRA
Asthma-COPD Overlap (ACO):
- Patients with features of both; often older smokers with partially reversible obstruction
- Treat with ICS + LABA + LAMA; avoid LABA monotherapy
High-Risk Asthma Patients (for mortality):
- Prior near-fatal asthma (ICU admission, intubation)
- ≥2 hospitalizations or ≥3 ED visits in past year
- Current use or recent discontinuation of oral steroids
- Poor perception of symptoms (blunted dyspnea response)
- Low socioeconomic status, poor adherence
- Major psychosocial problems
Severe Asthma:
- Asthma requiring high-dose ICS/LABA and/or oral corticosteroids to maintain control, or remaining uncontrolled despite this therapy
- Requires evaluation for biologic eligibility
Recent Evidence Note
A 2025 JAMA systematic review and network meta-analysis (PMID 39465893) on inhaled reliever therapies confirmed that ICS/formoterol combination reliever significantly reduces severe asthma exacerbations compared to SABA monotherapy, supporting the GINA recommendation to replace SABA alone as the preferred reliever across all asthma severity steps.
Key Summary
| Concept | Detail |
|---|---|
| Hallmark | Airway hyperresponsiveness + reversible obstruction |
| Primary inflammation | Type 2 (eosinophilic/IgE-mediated) in most |
| Diagnosis | History + spirometry with ≥12% reversibility after bronchodilator |
| Key spirometry finding | FEV1/FVC <0.70, reversed by bronchodilator |
| Reliever of choice (GINA 2025) | ICS/formoterol (AIR strategy) |
| Controller cornerstone | ICS (low dose) - escalate with LABA |
| Acute severe: add-on | Ipratropium + IV magnesium sulfate |
| Severe asthma biologics | Dupilumab, mepolizumab, benralizumab, tezepelumab |
| Montelukast warning | Serious neuropsychiatric effects (FDA 2020) |
| LABA rule | Never as monotherapy - only with ICS |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 298 - Asthma
Iron Deficiency Anemia (Etiology & RX),
Reading File
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND treatment
Finding Sources
Searching PubMed
"iron deficiency" AND "anemia" AND therapy
Reading File
Reading File
Reading File
Excellent - I have very comprehensive content. The read captured epidemiology, pathophysiology, causes, clinical features, lab diagnosis, and I can see it starts covering treatment. I have everything I need to compile the full detailed response.
Iron Deficiency Anemia - Etiology & Treatment
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Definition and Concept
Iron deficiency and iron deficiency anemia (IDA) exist on a spectrum:
| Stage | Iron Stores | Hb | Ferritin | Transferrin Sat |
|---|---|---|---|---|
| Iron depletion | Depleted | Normal | Low (<15-30 μg/L) | Normal |
| Iron-deficient erythropoiesis | Absent | Normal or borderline low | Very low | <20% |
| Iron deficiency anemia | Absent | Low | Very low | <15-20% |
- Absolute iron deficiency: iron stores completely exhausted
- Functional iron deficiency: erythropoiesis is iron-restricted but stores may be adequate or even elevated (as in inflammation, CKD, heart failure on ESA therapy)
Iron Metabolism - Brief Overview
- Daily dietary iron: ~15 mg; only 1-2 mg absorbed from the intestine per day
- Transferrin: hepatic glycoprotein (204-360 mg/dL) that carries iron in plasma; fast turnover; carries 3-4 mg at any time
- Erythroid precursors need 20-25 mg/day for red cell production - most is recycled from macrophages
- Hepcidin: key regulatory hormone produced by the liver
- Binds and degrades ferroportin (the sole iron exporter) on enterocytes and macrophages
- Elevated hepcidin (in inflammation, infection) → blocks iron absorption and release from stores → functional iron deficiency
- Suppressed hepcidin (in iron deficiency, hypoxia, hemorrhage) → increases iron absorption
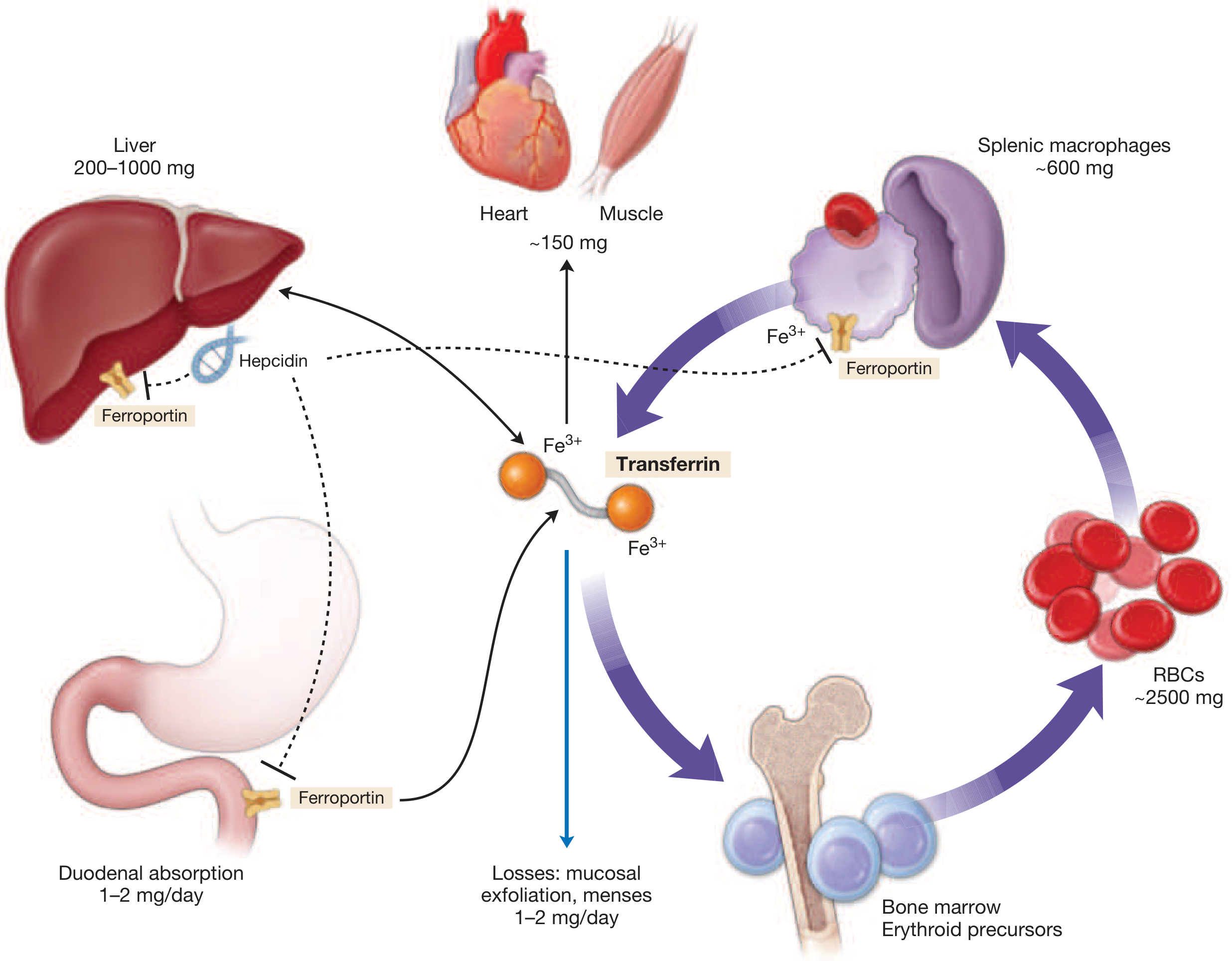
The iron body cycle: transferrin shuttles iron; hepcidin controls ferroportin-mediated iron export from enterocytes and macrophages
Epidemiology
- ~1.2 billion individuals affected worldwide - roughly half of all anemic people globally
- One of the leading causes of years lived with disability globally
- Highest-risk groups:
- Preschool children: prevalence ~25%
- Young women (12-21 years): 38.6% iron deficiency; 6.3% IDA (US data)
- Pregnant women: >40% with severe forms in low-income countries
- Especially prevalent in low-income countries, but high-income countries are not spared
Etiology / Causes of Iron Deficiency
Iron deficiency arises when supply is inadequate for iron needs, due to one or more of the following mechanisms:
1. Excessive Demand / Increased Requirements
| Population | Reason |
|---|---|
| Infants and children | Rapid growth increases iron requirements |
| Adolescents | Growth spurts + onset of menstruation in girls |
| Pregnancy | Fetal and placental demands + expanded maternal red cell mass (~700-1000 mg extra iron needed) |
| Erythropoiesis-stimulating agents (ESAs) | Expanded erythropoiesis outpaces iron supply → functional iron deficiency |
2. Inadequate Intake / Poor Nutrition
| Cause | Mechanism |
|---|---|
| Poor dietary intake | Diets low in heme iron (vegetarian/vegan) or calorie-restricted diets |
| Exclusive breastfeeding beyond 6 months | Breast milk low in iron |
| Cow's milk in infants | Poor iron content + may cause GI blood loss |
| Western diet contains ~6-7 mg/1000 calories; most people in LMICs consume inadequate amounts |
3. Defective Absorption (Malabsorption)
| Condition | Mechanism |
|---|---|
| Celiac disease | Mucosal damage in duodenum and proximal jejunum - prime site of iron absorption |
| Helicobacter pylori gastritis | Competes for iron; affects luminal iron availability |
| Atrophic gastritis / achlorhydria | Reduced gastric acid impairs conversion of Fe³⁺ to Fe²⁺ (absorbable form) |
| Post-gastrectomy / bariatric surgery | Bypass of duodenum; reduced gastric acid; rapid transit |
| Inflammatory bowel disease (IBD) | Combined absolute deficiency (malabsorption, blood loss) + functional deficiency (inflammation) |
| IRIDA (Iron-Refractory IDA) | Rare hereditary; mutations in TMPRSS6 → high hepcidin → refractory to oral iron |
| Proton pump inhibitors (long-term) | Reduce gastric acidity needed for iron absorption |
| Antacids, calcium, phosphate binders | Chelate dietary iron |
4. Blood Loss - The Most Common Cause in Adults
Chronic blood loss is the most common cause of IDA in adults, especially in developed countries. Even small but sustained losses exceed the capacity of intestinal absorption to compensate.
Gastrointestinal (Most Common Source in Men and Post-Menopausal Women)
| Source | Examples |
|---|---|
| Peptic ulcer disease | Most common GI cause |
| Colorectal cancer / polyps | Must always be excluded in adults >50 years |
| Gastric cancer | |
| Esophageal varices | Chronic slow bleeding |
| Hiatus hernia (Cameron lesions) | |
| Angiodysplasia / vascular ectasias | Common in elderly |
| NSAID-induced GI bleeding | Very common; chronic occult blood loss |
| Aspirin use | |
| Inflammatory bowel disease (Crohn's, UC) | Blood + malabsorption |
| Hookworm infestation | Major cause in tropics (Ancylostoma duodenale, Necator americanus) |
| Celiac disease | Malabsorption + mucosal bleeding |
Gynecological (Most Common Source in Pre-Menopausal Women)
| Source | Notes |
|---|---|
| Menorrhagia (heavy menstrual bleeding) | Most common cause of IDA in women of reproductive age |
| Uterine fibroids | Cause menorrhagia |
| Intrauterine device (IUD) | Copper IUDs can increase menstrual blood loss |
| Repeated pregnancies | Each pregnancy depletes ~500-1000 mg iron |
Urological / Other
| Source | Notes |
|---|---|
| Hematuria (renal cell carcinoma, bladder cancer, stones) | Chronic blood loss in urine |
| Pulmonary hemosiderosis | Alveolar hemorrhage with macrophage iron sequestration |
| Intravascular hemolysis | Hemoglobinuria (e.g., PNH, mechanical heart valves) with urinary iron loss |
| Iatrogenic | Frequent phlebotomy (hospitalized patients, dialysis patients) |
| Self-inflicted blood donation / repeated blood donation |
5. Genetic / Rare Causes
| Condition | Mechanism |
|---|---|
| IRIDA (Iron-Refractory IDA) | TMPRSS6 mutations → inability to suppress hepcidin → poor oral iron absorption |
| Variants in TF (transferrin gene), TMPRSS6 | Genetic susceptibility identified in GWAS studies |
Clinical Features
Symptoms of Anemia
- Fatigue, lethargy, reduced exercise tolerance
- Dyspnea on exertion
- Palpitations, tachycardia
- Dizziness, headache
- Pallor (conjunctival, palmar, nail bed)
Symptoms Specific to Iron Deficiency (Beyond Anemia)
- Pica: craving for non-food substances (ice - pagophagia, dirt - geophagia, clay, starch)
- Pagophagia (ice craving) is highly specific for iron deficiency
- Restless leg syndrome: strong urge to move legs, especially at rest
- Koilonychia: spoon-shaped nails (brittle, concave nails) - in severe/chronic IDA
- Angular cheilitis (stomatitis): cracking at corners of mouth
- Glossitis / atrophic tongue
- Dysphagia + upper esophageal web = Plummer-Vinson (Paterson-Kelly) Syndrome (rare, severe IDA)
- Impaired cognition and learning in children
- Blunted immune response: lymphocytes require iron for metabolic burst
- Cardiac effects: in CHF, iron deficiency causes symptoms even independently from anemia (functional impairment of cardiomyocytes)
Laboratory Diagnosis
Complete Blood Count and Red Cell Indices
| Parameter | IDA Finding |
|---|---|
| Hemoglobin | Low (severity varies) |
| MCV (Mean Corpuscular Volume) | Low (<80 fL) - microcytosis |
| MCH (Mean Corpuscular Hemoglobin) | Low (<27 pg) - hypochromia |
| MCHC | Low |
| RDW (Red Cell Distribution Width) | Elevated (>14.5%) - anisocytosis; earliest CBC change |
| Reticulocyte count | Low (hypoproliferative) |
| Platelets | Often elevated (reactive thrombocytosis) |
Iron Studies
| Test | IDA | Anemia of Inflammation | Combined |
|---|---|---|---|
| Serum Iron | Low | Low | Low |
| TIBC | High (>360 μg/dL) | Low/Normal | Variable |
| Transferrin Saturation | <15% | Low-Normal | <15% |
| Serum Ferritin | Low (<15-30 μg/L) | Normal/High | Low-Normal |
| Soluble Transferrin Receptor (sTfR) | Elevated | Normal | Elevated |
| sTfR/log ferritin index | High | Low | High |
| Hepcidin | Very low | Elevated | Variable |
Ferritin is an acute-phase reactant - it can be falsely normal or elevated in IDA with co-existing inflammation. A ferritin <100 μg/L in a patient with inflammation still likely indicates iron deficiency. sTfR or sTfR/log ferritin ratio is more reliable in this setting.
Peripheral Blood Smear
- Hypochromic, microcytic red cells (pale cells with central pallor >1/3 diameter)
- Pencil cells (elongated elliptocytes)
- Anisocytosis and poikilocytosis
- Target cells (less common)
Bone Marrow
- Absent iron stores on Prussian blue stain (definitive test, rarely needed)
- Absent hemosiderin and ferritin in macrophages
Differential Diagnosis of Microcytic Anemia
| Cause | Key Distinguishing Feature |
|---|---|
| IDA | Low ferritin, high TIBC, low Tsat |
| Anemia of chronic disease/inflammation | Normal-high ferritin, low TIBC, normal-high hepcidin |
| Thalassemia trait | Normal ferritin, Hb electrophoresis abnormal, family history; RDW often normal |
| Sideroblastic anemia | Ring sideroblasts on marrow; high ferritin |
| Lead poisoning | Basophilic stippling; elevated blood lead |
| IRIDA | IDA refractory to oral iron; TMPRSS6 mutation |
Treatment
Principles of Treatment
- Identify and treat the underlying cause (mandatory - do not just replace iron without investigating the source of blood loss or malabsorption)
- Replenish iron stores (not just correct hemoglobin)
- Continue iron until stores are fully restored (typically 3-6 months after Hb normalizes)
A. Oral Iron Therapy - First Line
Preparations (Ferrous Salts - Best Absorbed):
| Preparation | Elemental Iron per tablet | Notes |
|---|---|---|
| Ferrous sulfate 325 mg | ~65 mg elemental iron | Most commonly used; inexpensive |
| Ferrous gluconate 300 mg | ~35 mg elemental iron | Better tolerated; fewer GI side effects |
| Ferrous fumarate 200 mg | ~65 mg elemental iron | Good alternative |
| Ferrous bisglycinate | Variable | Chelated form; better absorbed with fewer GI effects; evidence base growing (Meta-analysis PMID 36728680) |
| Ferric iron (Fe³⁺) preparations | e.g., ferric carboxymaltose oral, ferric maltol | Alternative for those intolerant of ferrous; generally less well absorbed |
Standard Dosing:
- Adults: 150-200 mg elemental iron per day (e.g., ferrous sulfate 325 mg TID)
- Children: 3-6 mg/kg/day elemental iron in divided doses
Optimizing Oral Iron Absorption:
- Take on empty stomach (best absorbed) - though GI side effects increase
- Take with vitamin C (ascorbic acid) - reduces Fe³⁺ to Fe²⁺, enhances absorption
- Avoid co-administration with: calcium supplements, antacids, PPIs, tetracyclines, fluoroquinolones, tea, coffee, cereals, dairy (all reduce absorption)
- Alternate-day dosing (every other day) - recent evidence shows it may improve absorption compared to daily dosing by allowing hepcidin to reset between doses; reduces GI side effects
Response Monitoring:
- Reticulocyte rise in 7-10 days (first sign of response)
- Hemoglobin rise ~1 g/dL per week
- Hb should normalize in 6-8 weeks
- Continue iron for 3-6 months after Hb normalization to replenish stores
GI Side Effects (Common - Limit Compliance):
- Constipation, nausea, epigastric discomfort, diarrhea, dark stools
- Manage by: taking with food (reduces but doesn't eliminate GI effects), lower-dose preparations (ferrous gluconate, bisglycinate), liquid formulations, or switching to IV iron
Failure to Respond to Oral Iron - Consider:
- Non-compliance (most common)
- Ongoing blood loss exceeding replacement
- Malabsorption (celiac disease, H. pylori, IRIDA)
- Incorrect diagnosis (thalassemia, inflammation)
- Drug interactions reducing absorption
B. Intravenous (IV) Iron Therapy
Indications for IV Iron:
- Intolerance of oral iron (significant GI side effects)
- Poor oral iron absorption (celiac disease, IBD, bariatric/gastric surgery, achlorhydria)
- Chronic kidney disease (CKD) patients on dialysis or with EPO therapy
- Heart failure with iron deficiency (even without anemia - IV iron improves functional capacity and reduces hospitalizations)
- IRIDA (oral iron refractory - specifically requires IV iron)
- Need for rapid repletion (pre-operative anemia, severe symptomatic anemia)
- Pregnancy (second/third trimester, when oral therapy inadequate or fails)
- Active IBD (functional + absolute iron deficiency; oral iron may worsen inflammation)
- Inflammatory bowel disease, chronic kidney disease, cancer patients
IV Iron Preparations:
| Preparation | Administration | Key Notes |
|---|---|---|
| Ferric carboxymaltose (FCM) | Single dose up to 1000 mg; 15 min infusion | Most widely used; high single-dose capacity; risk of hypophosphatemia |
| Low molecular weight iron dextran | Up to 1000 mg; total dose infusion possible | Test dose required; anaphylaxis risk higher than newer agents |
| Iron sucrose | 100-200 mg per dose; multiple doses needed | Good safety profile; widely used in CKD/dialysis |
| Ferric gluconate | 125 mg per dose; multiple infusions | Approved for CKD/dialysis |
| Ferumoxytol | 510 mg single dose; fast infusion (15 min) | US approved; black box warning for anaphylaxis |
| Ferric derisomaltose (iron isomaltoside) | Up to 1500 mg single dose | High single-dose capacity; low hypophosphatemia risk |
Total Iron Deficit Calculation (Ganzoni formula):
Total iron dose (mg) = Body weight (kg) × (Target Hb - Actual Hb in g/dL) × 2.4 + Iron stores (500 mg)
Side Effects of IV Iron:
- Infusion reactions: flushing, hypotension, arthralgia, myalgia (especially with rapid infusion)
- Anaphylaxis: rare but serious (most risk with iron dextran); always have resuscitation ready
- Delayed reactions: arthralgia, myalgia 24-48 h post-infusion
- Hypophosphatemia: particularly with ferric carboxymaltose (transient, FGF23-mediated)
- Hypersensitivity: avoid in first trimester of pregnancy
C. Red Blood Cell Transfusion
Reserved for:
- Severe symptomatic anemia (Hb <7-8 g/dL) with hemodynamic instability, angina, or cardiac decompensation
- Perioperative situations requiring rapid correction
- Patients with compromised cardiopulmonary reserve
Transfusion corrects Hb rapidly but does not replace iron stores and does not address the underlying cause.
D. Treatment of Underlying Cause (Mandatory)
| Cause | Intervention |
|---|---|
| GI blood loss (ulcer, cancer, polyp) | Endoscopy + H. pylori eradication, PPI therapy, surgical resection |
| Menorrhagia | Hormonal therapy (OCP, levonorgestrel IUD, tranexamic acid), surgical management of fibroids |
| Celiac disease | Strict gluten-free diet |
| Hookworm | Antihelminthic (albendazole, mebendazole) |
| H. pylori | Eradication therapy (improves iron absorption + treats the cause) |
| Dietary deficiency | Nutritional counseling, dietary diversification |
E. Special Populations
Pregnancy:
- Oral iron first line; IV iron in second/third trimester if oral fails or is not tolerated
- Routine supplementation recommended in all pregnant women (30-60 mg elemental iron/day; WHO)
CKD (Chronic Kidney Disease):
- IV iron preferred especially in dialysis patients
- Target ferritin 200-500 μg/L; Tsat 20-50%
- IV iron reduces ESA dose requirement
Heart Failure:
- IV iron (especially ferric carboxymaltose) improves symptoms, 6-minute walk test, and quality of life in HF patients with iron deficiency even without anemia
- 2025 meta-analysis in Nature Medicine (PMID 40159279) confirmed IV iron reduces hospitalizations in HF with iron deficiency
IBD:
- Oral iron may worsen mucosal inflammation and GI symptoms; IV iron preferred in active disease
- During remission, oral iron with close monitoring is acceptable
IRIDA:
- Oral iron is ineffective due to persistently elevated hepcidin
- IV iron required; response may be partial
Key Summary
| Feature | Detail |
|---|---|
| Most common cause globally | Nutritional deficiency + menstrual loss |
| Most common cause in adult men / post-menopausal women | GI blood loss (must exclude cancer) |
| Classic CBC triad | Low MCV + low MCH + high RDW |
| Diagnostic gold standard | Low serum ferritin (<15-30 μg/L) |
| Best marker in inflammation | sTfR / sTfR-log ferritin index |
| First-line treatment | Oral ferrous sulfate |
| Preferred route in CKD/IBD/HF | IV iron |
| Duration of therapy | 3-6 months after Hb normalizes |
| Always do | Investigate and treat the underlying cause |
| Never do | Treat IDA without identifying the etiology |
📌 Recent Evidence: A 2025 Nature Medicine meta-analysis (PMID 40159279) on IV iron in heart failure with iron deficiency confirmed significant reduction in hospitalizations, supporting its use even in non-anemic iron deficiency in HF. A 2023 meta-analysis (PMID 36728680) confirmed ferrous bisglycinate as an effective oral iron option with improved Hb and ferritin outcomes across populations.
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 102 - Iron Deficiency and Other Acquired Anemias Due to Decreased Erythrocyte Production
(Risk factor & emergency RX),
Of stroke
Reading File
Finding Sources
Searching PubMed
"ischemic stroke"[MeSH Terms] AND "emergency treatment"
Reading File
Reading File
Stroke (Risk factor & emergency RX)
Finding Sources
Searching PubMed
"ischemic stroke" AND "thrombolysis" AND "thrombectomy"
Reading File
Reading File
Reading File
I now have the full emergency treatment content from Harrison's (read at offset 2467 earlier). The risk factors section appeared around line 2406-2455 in the previous reads. I have enough comprehensive material to write the full response. Let me compile it now.
Stroke - Risk Factors & Emergency Treatment
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Types of Stroke
| Type | Frequency | Mechanism |
|---|---|---|
| Ischemic stroke | ~87% | Arterial occlusion → infarction |
| Intracerebral hemorrhage (ICH) | ~10% | Rupture of intracerebral vessel |
| Subarachnoid hemorrhage (SAH) | ~3% | Rupture of aneurysm/AVM |
PART I: RISK FACTORS FOR STROKE
A. Non-Modifiable Risk Factors
| Risk Factor | Details |
|---|---|
| Age | Most powerful risk factor; risk doubles each decade after age 55; ~75% of strokes occur after age 65 |
| Sex | Men have higher stroke incidence; women have higher lifetime risk due to longer lifespan and AF-related stroke |
| Race/Ethnicity | Black, Hispanic, and South Asian populations have higher risk; Black Americans have 2x higher stroke mortality than White Americans |
| Family history / Genetics | Positive family history increases risk ~3-fold; genetic conditions: CADASIL, sickle cell disease, MELAS, Fabry disease |
| Prior stroke or TIA | Highest short-term risk period; ~10-15% stroke risk within 3 months of TIA (highest in first 48 hours) |
B. Modifiable Risk Factors
1. Hypertension - The Single Most Important Modifiable Risk Factor
- Increases stroke risk 4-fold for ischemic stroke and up to 10-fold for hemorrhagic stroke
- Risk is proportional to BP level - even "high normal" BP (130-139/80-89 mmHg) carries elevated risk
- Treating hypertension reduces stroke risk by 35-44%
- Both systolic and diastolic hypertension are risk factors; isolated systolic hypertension (elderly) is particularly important
2. Atrial Fibrillation (AF)
- Increases ischemic stroke risk 5-fold
- Responsible for ~15-20% of all ischemic strokes; up to 30% in elderly patients
- Cardioembolic strokes from AF tend to be large, severe, and more disabling
- CHA₂DS₂-VASc score guides anticoagulation decisions
- AF may be paroxysmal and silent - often discovered only after a stroke
3. Diabetes Mellitus
- Increases stroke risk 2-6-fold
- Accelerates atherosclerosis; promotes small vessel disease (lacunar infarcts)
- Hyperglycemia at time of stroke worsens outcome (extends infarct size)
- Metabolic syndrome and insulin resistance also increase risk independently
4. Dyslipidemia
- Elevated LDL-cholesterol promotes large-vessel atherosclerosis (carotid, intracranial arteries)
- Statin therapy reduces ischemic stroke risk by ~25-30%
- Low HDL is an independent risk factor
- High triglycerides associated with increased risk through VLDL/remnant particles
5. Smoking
- Increases ischemic stroke risk 2-fold; increases SAH risk 3-10-fold
- Promotes atherosclerosis, increases platelet aggregation, elevates fibrinogen, causes arterial wall injury
- Risk decreases significantly within 2-5 years of cessation
6. Cardiac Disease
| Cardiac Cause | Mechanism | Estimated Stroke Risk |
|---|---|---|
| Atrial fibrillation | Atrial thrombus (LAA) → embolism | 5x increased |
| Recent MI | Mural thrombus (especially anterior STEMI) → embolism | ~2-3% post-MI |
| Valvular disease (mitral stenosis, prosthetic valves) | Thrombus formation on valve | High |
| Patent foramen ovale (PFO) | Paradoxical embolism | Especially in young stroke |
| Heart failure / low EF | Low-flow state, thrombus formation | Proportional to EF reduction |
| Infective endocarditis | Septic emboli | High if vegetations present |
7. Carotid Artery Disease
- Symptomatic carotid stenosis >70%: ~26% stroke risk within 2 years without intervention
- Asymptomatic carotid stenosis >60%: ~2%/year stroke risk
- Carotid endarterectomy or stenting reduces risk significantly
8. Obesity
- BMI >30 increases stroke risk by ~64% independent of other risk factors
- Promotes hypertension, diabetes, AF, dyslipidemia, and sleep apnea
9. Physical Inactivity
- Sedentary lifestyle independently associated with ~2x increased stroke risk
- Regular moderate exercise (150 min/week) reduces risk by ~25%
10. Alcohol Use
- Heavy alcohol use (>5 drinks/day): increases ischemic and hemorrhagic stroke risk significantly
- Moderate alcohol use: potentially modestly protective for ischemic stroke (controversial; no longer recommended as preventive measure)
- Binge drinking is a clear risk factor regardless of average intake
11. Drug Use
| Drug | Mechanism |
|---|---|
| Cocaine / amphetamines | Vasospasm, accelerated hypertension, vasculitis, cardioembolism |
| IV drug use | Infective endocarditis → septic emboli |
| Oral contraceptives | Hypercoagulability + hypertension; especially risky with smoking/migraine with aura |
12. Hyperhomocysteinemia
- Elevated homocysteine promotes endothelial injury and thrombosis
- Treatable with folate, B6, B12 supplementation
- MTHFR mutations contribute
13. Coagulation / Hematologic Disorders
| Condition | Notes |
|---|---|
| Antiphospholipid syndrome | Recurrent arterial and venous thrombosis; young stroke patients |
| Factor V Leiden / Prothrombin mutation | Predominantly venous; paradoxical embolism via PFO |
| Polycythemia vera / thrombocytosis | Hyperviscosity and thrombosis |
| Sickle cell disease | Major stroke cause in children; transcranial Doppler screening indicated |
| Thrombotic thrombocytopenic purpura (TTP) | Microvascular thrombosis |
14. Obstructive Sleep Apnea (OSA)
- Independently increases stroke risk ~2-3-fold
- Promotes nocturnal hypertension, cardiac arrhythmias (AF), hypercoagulability
- CPAP therapy reduces risk
15. Migraine with Aura
- ~2-fold increased ischemic stroke risk, especially in young women
- Risk multiplied significantly with OCP use and smoking
16. Other Conditions
- Inflammatory states (lupus, vasculitis, giant cell arteritis)
- Chronic kidney disease (promotes hypertension, atherosclerosis, AF)
- Peripartum state (hypercoagulability, eclampsia, cardiomyopathy)
- SARS-CoV-2 infection (COVID-19): associated with coagulopathy and stroke
Summary of Stroke Risk Factors by Modifiability
| Non-Modifiable | Modifiable (Major) | Modifiable (Other) |
|---|---|---|
| Age | Hypertension | Obesity |
| Sex | Atrial fibrillation | Physical inactivity |
| Race/ethnicity | Diabetes | Alcohol/drugs |
| Family history | Dyslipidemia | Sleep apnea |
| Prior stroke/TIA | Smoking | Migraine with aura |
| Genetic conditions | Carotid stenosis | Coagulopathies |
| Cardiac disease | OCP use |
PART II: EMERGENCY TREATMENT OF ACUTE ISCHEMIC STROKE
The "Time is Brain" Principle
1.9 million neurons die every minute during a large vessel occlusion without treatment. Rapid recognition and treatment is the single most important factor in improving outcome.
Six Categories of Treatment (Harrison's 22E)
- Medical support
- IV thrombolysis
- Endovascular revascularization
- Antithrombotic treatment
- Neuroprotection
- Stroke centers and rehabilitation
Step 1: Immediate Assessment (First 10-15 Minutes)
Before any treatment:
- Activate stroke code / call ahead to hospital for pre-alert
- ABCs: Airway, Breathing, Circulation - stabilize
- Finger-stick glucose: treat hypoglycemia (glucose <3.3 mmol/L/60 mg/dL) or hyperglycemia immediately
- IV access, cardiac monitoring, pulse oximetry
- Neurological examination: use NIHSS (NIH Stroke Scale) to quantify deficit
- BP measurement: document and manage appropriately (see below)
- Symptom onset time: exact time last known well (LKW) is critical for treatment eligibility
FAST / BE-FAST screening:
- Balance loss, Eyes (vision loss), Face droop, Arm weakness, Speech difficulty, Time to call emergency
Step 2: Emergency Imaging
Non-contrast CT head (NCCT) - FIRST LINE and FASTEST
- Performed immediately on arrival ("CT first, ask questions later")
- Primary purpose: rule out hemorrhagic stroke (appears as hyperdense)
- Also detects: large established infarct (if >1/3 MCA territory → thrombolysis relatively contraindicated), hyperdense MCA sign (clot)
- No reliable clinical features alone can distinguish ischemic from hemorrhagic stroke
Additional imaging:
- CT Angiography (CTA): rapidly identifies large vessel occlusion (LVO) for thrombectomy planning; simultaneous with NCCT
- CT Perfusion (CTP): defines ischemic core (irreversibly infarcted) vs. penumbra (salvageable tissue); guides treatment in late window (6-24 hours)
- MRI/DWI: more sensitive for early ischemia (detects within minutes); not always available acutely
Step 3: Medical Support (Concurrent with Imaging)
Blood Pressure Management
| Situation | Target |
|---|---|
| No thrombolysis planned | Do NOT lower BP unless >220/120 mmHg |
| Thrombolysis planned | Lower to <185/110 mmHg before and maintain <180/105 mmHg during/after tPA |
| Hemorrhagic stroke | Target SBP <140 mmHg |
- Routine BP lowering below 220/120 mmHg worsens outcomes in acute ischemic stroke (removes collateral perfusion pressure)
- Agents: IV labetalol, nicardipine, or clevidipine for controlled reduction
- Avoid: aggressive lowering; sublingual nifedipine (unpredictable drops)
Glucose Management
- Target glucose: 3.3-10.0 mmol/L (60-180 mg/dL)
- Hyperglycemia worsens infarct extension; hypoglycemia can mimic stroke and worsen injury
- Give IV dextrose immediately for hypoglycemia (<60 mg/dL)
- Intensive glucose control (tight control) does NOT improve outcome
Fever
- Detrimental - increases metabolic demand in ischemic penumbra
- Treat aggressively with antipyretics (paracetamol/acetaminophen) and surface cooling
- Target normothermia (≤37.5°C)
Cerebral Edema
- 5-10% of patients develop significant cerebral edema
- Peaks at day 2-3 but can cause mass effect for ~10 days
- Larger infarcts → greater edema risk ("malignant MCA infarction")
- Treatment: IV mannitol, water restriction, head-of-bed elevation 30°
- Decompressive hemicraniectomy: life-saving in malignant MCA territory infarction with clinical deterioration; reduces mortality significantly (especially <60 years of age)
DVT Prevention
- Subcutaneous heparin (LMWH or UFH) safe to use concomitantly
- Pneumatic compression stockings: proven benefit, safe alternative
Airway/Oxygenation
- Supplemental oxygen only if SpO2 <94% (routine oxygen in normoxic patients does not improve outcome)
- Intubation and mechanical ventilation for reduced consciousness/airway protection
Step 4: IV Thrombolysis (tPA/Alteplase)
Drug: Alteplase (recombinant tPA)
- Dose: 0.9 mg/kg IV (maximum 90 mg); 10% as bolus over 1 minute, remainder over 60 minutes
- Mechanism: activates plasminogen → plasmin → clot lysis
Time Window:
- Standard window: within 4.5 hours of symptom onset (last known well time)
- Earlier treatment = better outcome: "time is brain"
- Greatest benefit when given within 3 hours
Extended window (3-4.5 hours) - additional exclusions:
- Age >80 years (relative)
- Prior stroke + diabetes together
- NIHSS >25
- Anticoagulant use
-
1/3 MCA territory infarction on imaging
Absolute Contraindications to tPA:
| Contraindication | Reason |
|---|---|
| Hemorrhage on CT | Would worsen bleeding |
| BP >185/110 (untreated) | Hemorrhagic transformation risk |
| Active internal bleeding | |
| Recent major surgery (<14 days) or trauma | |
| Recent intracranial/spinal surgery (<3 months) | |
| Prior intracranial hemorrhage (ever) | |
| Intracranial neoplasm, AVM, or aneurysm | |
| Platelet count <100,000 | |
| INR >1.7 (on warfarin) | |
| IV heparin within 48 h with elevated aPTT | |
| Glucose <50 or >400 mg/dL (without correction) | Stroke mimic |
| Ischemic stroke or serious head trauma within 3 months |
Tenecteplase (TNK-tPA): single IV bolus alternative to alteplase; increasingly used especially before thrombectomy (simpler administration, comparable efficacy)
📌 2025 Cochrane Review (PMID 40271574): Endovascular thrombectomy with vs. without prior IV thrombolysis - current evidence suggests IV tPA before thrombectomy remains the standard when eligible, though direct-to-thrombectomy is being studied.
📌 2025 Meta-analysis (PMID 39882605): Thrombolysis beyond the 4.5-hour window (using perfusion imaging to select salvageable tissue) showed benefit in selected patients, supporting extended window protocols with CTP guidance.
Step 5: Endovascular Thrombectomy (EVT/Mechanical Thrombectomy)
The most significant advance in acute stroke treatment in decades.
Indications:
- Large vessel occlusion (LVO): ICA, M1/M2 MCA, basilar artery, vertebral artery
- NIHSS ≥6 (significant deficit)
- Time window: 0-6 hours from onset (standard); up to 24 hours with favorable CT perfusion mismatch (DAWN/DEFUSE-3 trial criteria)
- No large established core infarct (>1/3 MCA territory or large DWI lesion)
- Modified Rankin Scale (mRS) 0-1 premorbidly (functionally independent before stroke)
Procedure:
- Femoral artery access → catheter advanced to occluded vessel
- Stent retriever or aspiration catheter mechanically removes clot
- Target: TICI 2b-3 reperfusion (>50-90% territory reperfusion)
- "Door-to-groin" time target: <90 minutes
Outcomes:
- 2x more likely to achieve functional independence compared to IV tPA alone in LVO
- Benefit shown even in extended windows with perfusion imaging guidance
- Basilar artery occlusion: thrombectomy is lifesaving; associated with "locked-in" syndrome if untreated
Combined IV tPA + EVT:
- If patient is eligible for both: IV tPA first (bridge therapy), then proceed immediately to thrombectomy
- IV tPA does not delay and may facilitate EVT
Step 6: Antithrombotic Treatment
Aspirin:
- 325 mg orally within 24-48 hours of ischemic stroke onset
- Contraindicated within 24 hours of IV tPA (increases hemorrhagic transformation risk)
- Reduces early recurrent stroke risk
Anticoagulation (heparin, LMWH, warfarin):
- NOT routinely recommended in acute ischemic stroke (risk of hemorrhagic transformation outweighs benefit)
- Exceptions: cardioembolic stroke with high recurrence risk, cerebral venous sinus thrombosis, arterial dissection
Dual Antiplatelet Therapy (DAPT):
- Aspirin + clopidogrel for 21 days: indicated for minor ischemic stroke (NIHSS ≤3) or high-risk TIA (ABCD2 score ≥4)
- Based on POINT and CHANCE trials
- Reduces early recurrent stroke without significantly increasing bleeding risk
Step 7: Stroke Unit / Specialized Care
- All stroke patients should be admitted to a dedicated stroke unit - reduces mortality and disability by 20-25% vs. general ward
- Multidisciplinary team: neurology, nursing, PT, OT, speech therapy, dietitian, social work
- Early mobilization (within 24-48 hours for mild-moderate strokes)
- Dysphagia screening before oral intake (prevent aspiration pneumonia - major cause of post-stroke mortality)
- Cardiac monitoring for 24-72 hours: detect paroxysmal AF (identifies cardioembolic source)
Hemorrhagic Stroke - Emergency Management Differences
Intracerebral Hemorrhage (ICH):
- No thrombolysis or thrombectomy (contraindicated - would worsen bleeding)
- Reverse anticoagulation immediately:
- Warfarin → IV Vitamin K + prothrombin complex concentrate (PCC)
- DOACs → specific reversal agents (idarucizumab for dabigatran; andexanet alfa for Xa inhibitors)
- Heparin → protamine sulfate
- Aggressive BP control: target SBP <140 mmHg within 1 hour (AHA/ASA 2022)
- Surgical evacuation: for cerebellar hematoma >3 cm with mass effect (life-saving); selected supratentorial hemorrhages
- ICP management: osmotherapy (mannitol, hypertonic saline), sedation, positioning, ventriculostomy for hydrocephalus
Emergency Stroke Algorithm Summary
Symptom onset → 911 call → Pre-alert hospital
ARRIVAL:
├── ABCs + IV access + monitor
├── Finger-stick glucose → correct if abnormal
├── Immediate NCCT head (±CTA)
│
├── HEMORRHAGE → ICH/SAH protocol (reverse anticoagulation, BP control, neurosurgery)
│
└── ISCHEMIC STROKE:
├── <4.5 h + eligible → IV ALTEPLASE 0.9 mg/kg
├── LVO detected → THROMBECTOMY (up to 24 h with imaging selection)
├── Aspirin 325 mg (after tPA window or if tPA not given)
├── BP: do not lower unless >220/120 (>185/110 if tPA planned)
├── Glucose: 60-180 mg/dL
├── Treat fever
└── Admit to STROKE UNIT
Key Numbers to Remember
| Parameter | Value |
|---|---|
| IV tPA window | ≤4.5 hours from symptom onset |
| tPA dose | 0.9 mg/kg IV (max 90 mg) |
| tPA BP threshold | Must be <185/110 before administration |
| Thrombectomy standard window | 0-6 hours; extended to 24 h with perfusion imaging |
| BP: do not lower below | 220/120 mmHg (unless tPA planned) |
| Glucose target | 60-180 mg/dL |
| Aspirin timing | Within 24-48 h; NOT within 24 h of tPA |
| DAPT (minor stroke/TIA) | Aspirin + clopidogrel for 21 days |
| Stroke unit benefit | 20-25% reduction in mortality/disability |
| Neurons lost per minute | ~1.9 million |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapters 437 & 438 - Cerebrovascular Diseases and Ischemic Stroke
Ventilator Associated Pneumonia.
Finding Sources
Searching PubMed
"ventilator-associated pneumonia"[MeSH Terms] AND prevention AND treatment
Reading File
Searching PubMed
"ventilator-associated pneumonia" AND antibiotic
Reading File
Excellent - I now have comprehensive content covering etiology, epidemiology, pathogenesis, diagnosis, empirical antibiotic therapy tables, and de-escalation. I have everything needed for a thorough response. Let me compile it now.
Ventilator-Associated Pneumonia (VAP)
Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Definition
Ventilator-Associated Pneumonia (VAP) is a hospital-acquired pneumonia (HAP) that develops ≥48 hours after endotracheal intubation and mechanical ventilation. It is the most common and serious infectious complication in mechanically ventilated ICU patients, and is a distinct entity from:
- Non-ventilated HAP: pneumonia in hospitalized patients not on mechanical ventilation
- Ventilated HAP: HAP in patients requiring ventilation but acquired before intubation
Epidemiology
- Prevalence estimates: 6-52 cases per 100 mechanically ventilated patients (varies by population, ICU type)
- On any given ICU day, ~10% of ventilated patients have VAP
- Frequency was declining due to prevention bundles, but COVID-19 increased its incidence
- Highest risk in the first 5 days of mechanical ventilation (highest hazard ratio in early period)
- Crude mortality: 20-50% in VAP; attributable mortality ~10-15% when controlling for confounders
- Increases ICU stay by 5-10 days and hospital costs significantly
- ~30% of all HAP occurs in the ICU; 35% of all HAP patients eventually require mechanical ventilation
Pathogenesis / Risk Factors
How VAP Develops
The fundamental mechanism is aspiration of oropharyngeal or gastric secretions into the lower respiratory tract past the endotracheal tube cuff, combined with compromised host defenses.
Three critical steps:
- Colonization of oropharynx and/or stomach with pathogenic bacteria (including MDR organisms)
- Aspiration of contaminated secretions past the ETT cuff into the lower airways
- Impaired host defenses: mucociliary clearance bypassed by ETT; cough reflex suppressed; impaired alveolar macrophage function (sedation, malnutrition, immunosuppression)
Risk Factors for VAP
| Category | Specific Risk Factors |
|---|---|
| Intubation itself | Bypasses normal upper airway defenses; creates conduit for pathogen entry |
| Supine positioning | Promotes aspiration of gastric/oropharyngeal contents |
| Prolonged mechanical ventilation | Duration is the strongest risk factor; risk cumulative |
| Re-intubation | Each intubation event significantly increases risk |
| Prior antibiotic exposure | Selects for MDR organisms (MRSA, ESBL, carbapenem-resistant) |
| High PEEP / large tidal volumes | Compromise mucociliary clearance |
| Nasogastric tube | Promotes gastric reflux and aspiration |
| Gastric acid suppression (H2 blockers, PPIs) | Allows gastric colonization with gram-negatives; increases aspiration risk |
| Sedation / neuromuscular blockade | Abolishes cough reflex, impairs secretion clearance |
| Transport from ICU | Increases aspiration events |
| Underlying lung disease (COPD, ARDS) | Impaired local defenses |
| Immunosuppression | Increases risk of fungal and viral VAP |
| Poor oral hygiene | Increases oropharyngeal bacterial burden |
| Enteral feeding | Gastric distension promotes reflux; but still preferred over TPN |
| Head trauma / neurosurgical patients | Aspiration-prone; depressed gag reflex |
| Duration of hospitalization before intubation | Longer pre-ICU stay → more MDR colonization |
Risk Factors Specifically for MDR Pathogens in VAP
- Prior antibiotic therapy (especially β-lactams, cephalosporins → MRSA, ESBL)
- Hospitalization ≥5 days before VAP onset ("late-onset VAP")
- Mechanical ventilation ≥5 days
- Prior hospitalization within 90 days
- Nursing home or long-term care facility residence
- Prior culture positive for MDR organism
- High local prevalence of MDR pathogens in the ICU
- Immunosuppression
- Septic shock at VAP onset
Microbiology / Etiology
VAP pathogens differ critically from community-acquired pneumonia in their MDR profile:
Non-MDR "Core Pathogens" (Early-Onset VAP, No MDR Risk Factors)
- Streptococcus pneumoniae
- Haemophilus influenzae
- Methicillin-sensitive Staphylococcus aureus (MSSA)
- Antibiotic-sensitive Enterobacteriaceae: Escherichia coli, Klebsiella pneumoniae, Proteus spp., Enterobacter spp., Serratia marcescens
MDR Pathogens (Late-Onset or with MDR Risk Factors) - The Critical Difference
| MDR Pathogen | Notes |
|---|---|
| Pseudomonas aeruginosa | Most common MDR pathogen in VAP; can develop resistance during treatment (derepression of resistance genes); resistant to all routine antibiotics in some strains |
| MRSA (Methicillin-resistant S. aureus) | Major problem in most ICUs; requires vancomycin or linezolid |
| Acinetobacter spp. | Intrinsically resistant to many agents; carbapenem-resistant strains endemic in some ICUs |
| ESBL-producing Enterobacteriaceae | Extended-spectrum β-lactamase producers; selected by cephalosporin use |
| Carbapenem-resistant Enterobacteriaceae (CRE) | Extremely limited treatment options |
| Legionella pneumophila | Nosocomial; linked to hospital water supply contamination |
| Burkholderia cepacia | Intrinsically resistant; emerges during treatment |
| Stenotrophomonas maltophilia | Intrinsically carbapenem-resistant; trimethoprim-sulfamethoxazole is treatment of choice |
| Aspergillus spp. | In severely immunocompromised patients |
Key principle: The relative frequency of individual MDR pathogens varies hospital by hospital and even ICU by ICU. Local antibiogram data is essential for empirical therapy selection.
Diagnosis
Clinical Criteria
VAP is suspected when mechanically ventilated patients develop:
- New or progressive pulmonary infiltrate on chest X-ray/CT
- Plus ≥2 of the following:
- Fever (>38.3°C) or hypothermia (<36°C)
- Purulent tracheal secretions
- Leukocytosis (>12,000/μL) or leukopenia (<4,000/μL)
- Worsening oxygenation (↑FiO2 requirement, ↑PEEP, ↓PaO2/FiO2 ratio)
Important caveat: Clinical criteria alone have low specificity in mechanically ventilated patients - fever, leukocytosis, and pulmonary infiltrates have many non-infectious causes (ARDS, pulmonary edema, atelectasis, drug reactions).
Clinical Pulmonary Infection Score (CPIS)
Combines temperature, WBC, tracheal secretions, PaO2/FiO2, chest X-ray, and tracheal culture results
- CPIS >6 suggests VAP
- More useful for monitoring response than initial diagnosis
Microbiologic Sampling - Critical for Diagnosis and De-escalation
| Method | Details | Advantage | Limitation |
|---|---|---|---|
| Endotracheal aspirate (ETA) | Quantitative or semi-quantitative culture; threshold ≥10⁶ CFU/mL | Easy, widely available | Less specific (may include colonizers) |
| Bronchoalveolar lavage (BAL) | Threshold ≥10⁴ CFU/mL | More specific sampling of lower tract | Requires bronchoscopy |
| Protected specimen brush (PSB) | Threshold ≥10³ CFU/mL | Most specific | Bronchoscopy required; sampling error |
| Mini-BAL (blind) | Performed without bronchoscopy | Does not require bronchoscope | Less precise location |
- Gram stain from lower respiratory sample provides early (1-hour) guidance
- Blood cultures: positive in ~15-25% of VAP (identifies bacteremic spread)
- Urinary antigen tests: Legionella antigen (urine) - especially if outbreak suspected
- Serum procalcitonin (PCT): useful to monitor treatment response and guide duration of therapy; declining PCT supports discontinuation
Treatment
Principle: "Start Broad, De-escalate Early"
- Initiate empirical therapy immediately after microbiologic specimens collected - delay increases mortality
- Broaden or narrow based on 48-72h culture/sensitivity results (de-escalation)
- Shorten duration to avoid resistance selection (target 7-8 days for most VAP)
A. Empirical Antibiotic Therapy
Selection depends on two key decisions:
- Are there risk factors for MDR pathogens?
- Is the predicted mortality risk high (>15%) or low (≤15%)?
Group 1: No MDR Risk Factors (Low Mortality Risk) → Monotherapy
| Agent | Dose |
|---|---|
| Piperacillin-tazobactam | 4.5 g IV q6h |
| Cefepime | 2 g IV q8h |
| Levofloxacin | 750 mg IV q24h |
| Imipenem | 500 mg IV q6h |
| Meropenem | 1 g IV q8h |
- Single agent sufficient; mortality is lower with monotherapy vs. combination in low-risk patients
- Covers core pathogens + non-resistant P. aeruginosa
- If atypical pathogens not a concern (unlike CAP), dedicated atypical coverage not routinely needed
Group 2: MDR Risk Factors and/or High Mortality Risk → Triple Therapy (Three Antibiotics)
Column 1: Anti-pseudomonal β-lactam (choose one)
| Agent | Dose |
|---|---|
| Piperacillin-tazobactam | 4.5 g IV q6h |
| Cefepime or ceftazidime | 2 g IV q8h |
| Imipenem | 500 mg IV q6h |
| Meropenem | 1 g IV q8h |
| Aztreonam | 2 g IV q8h (if severe β-lactam allergy) |
Column 2: Second anti-gram-negative agent (choose one) - for double coverage of P. aeruginosa
| Agent | Dose |
|---|---|
| Amikacin | 15-20 mg/kg IV q24h |
| Gentamicin | 5-7 mg/kg IV q24h |
| Tobramycin | 5-7 mg/kg IV q24h |
| Levofloxacin | 750 mg IV q24h |
| Ciprofloxacin | 400 mg IV q8h |
Column 3: MRSA Coverage (add if MRSA risk factors present)
| Agent | Dose | Notes |
|---|---|---|
| Vancomycin | 15-20 mg/kg IV q8-12h (AUC-guided dosing) | Target AUC/MIC 400-600 |
| Linezolid | 600 mg IV/PO q12h | Some evidence of superior lung penetration vs. vancomycin; oral bioavailability ~100% |
Special Pathogens:
| Pathogen | Treatment |
|---|---|
| MRSA | Vancomycin (AUC-guided) or linezolid 600 mg q12h |
| Acinetobacter (carbapenem-sensitive) | Carbapenem (imipenem/meropenem) |
| Acinetobacter (carbapenem-resistant) | Polymyxin B or colistin + rifampin or carbapenem; cefiderocol (newer option) |
| CRE (carbapenem-resistant Enterobacteriaceae) | Ceftazidime-avibactam, meropenem-vaborbactam, cefiderocol, polymyxins |
| Stenotrophomonas maltophilia | Trimethoprim-sulfamethoxazole (TMP-SMX) |
| ESBL-producing organisms | Carbapenems (imipenem/meropenem); avoid cephalosporins even if sensitive |
| Legionella | Fluoroquinolone (levofloxacin) or azithromycin |
| Aspergillus (in immunocompromised) | Voriconazole or isavuconazole |
B. De-escalation (48-72 Hours)
- Once culture results are available: narrow antibiotics to the narrowest effective agent
- If cultures are negative and clinical improvement: strongly consider stopping antibiotics (especially if CPIS improving, PCT declining)
- De-escalation reduces:
- Selection pressure for MDR organisms
- Antibiotic side effects (nephrotoxicity, C. difficile)
- Costs
- De-escalation is safe and does not worsen outcomes in VAP
C. Duration of Therapy
- Standard: 7-8 days for most VAP (including P. aeruginosa if clinically responding)
- Shorter courses (7 days) are recommended over longer (14-21 days) by IDSA/ATS guidelines
- Exceptions requiring longer therapy:
- Bacteremia (especially S. aureus bacteremia → 14+ days)
- Necrotizing pneumonia or lung abscess
- Immunocompromised patients
- Inadequate initial therapy
- Poor clinical response
D. Monitoring Treatment Response
| Marker | Expected Change with Successful Treatment |
|---|---|
| Temperature | Defervescence within 3-5 days |
| WBC | Normalizing by day 3-5 |
| PaO2/FiO2 ratio | Improving; FiO2 requirements decreasing |
| Tracheal secretions | Becoming less purulent |
| Chest X-ray | Slow to improve; not primary monitoring tool |
| Serum procalcitonin (PCT) | Declining PCT supports de-escalation/discontinuation |
Failure to improve at 48-72 hours should prompt: review of culture sensitivities, broaden to cover MDR organisms, consider non-infectious causes (ARDS, PE, drug fever), or look for complications (empyema, lung abscess)
Prevention - The VAP Bundle
Prevention is the most cost-effective strategy. The "VAP Bundle" (evidence-based set of interventions) significantly reduces VAP rates:
1. Head-of-Bed Elevation
- Semi-recumbent position (30-45°) at all times during mechanical ventilation
- Reduces aspiration of gastric contents
- Simple, zero-cost, proven effective
2. Oral Decontamination
- Chlorhexidine gluconate (0.12-0.2%) oral rinse every 6-12 hours
- Reduces oropharyngeal colonization with gram-negative bacteria
- Particularly beneficial in cardiac surgery patients
- Evidence for non-cardiac ICU patients is strong but slightly less consistent
3. Subglottic Secretion Drainage (SSD)
- Specialized ETTs with a separate suction lumen above the cuff
- Continuously or intermittently drains secretions pooling above the cuff (main reservoir before aspiration)
- Reduces early-onset VAP by ~50% in patients expected to require ventilation >48-72 hours
4. Endotracheal Tube Cuff Pressure Management
- Maintain cuff pressure 20-30 cmH₂O (prevents aspiration around cuff while avoiding mucosal ischemia)
- Use continuous cuff pressure monitoring in high-risk patients
5. Minimize Sedation / Early Liberation from Ventilator
- Daily sedation interruption ("sedation holidays") - reduces ventilator days
- Spontaneous breathing trials (SBT) daily - once stable, assess readiness for extubation
- Shortest ventilation duration possible = most effective VAP prevention
- SAT + SBT protocol (Spontaneous Awakening Trial + Spontaneous Breathing Trial) linked in the ABCDE bundle
6. Selective Oral Decontamination (SOD) / Selective Digestive Decontamination (SDD)
- SDD: topical antibiotics in oropharynx/GI tract + short systemic antibiotics
- Reduces VAP rates but concerns about antibiotic resistance selection limit widespread adoption
- Considered in specific ICUs with known low MDR burden
7. Avoid Unnecessary Gastric Acid Suppression
- Limit H2 blockers and PPIs to patients with genuine indications (high GI bleeding risk)
- Sucralfate as alternative in lower-risk patients (does not raise gastric pH, may reduce VAP)
8. Proper Hand Hygiene and Infection Control
- Hand hygiene (soap + water or alcohol-based handrub) before/after patient contact
- Contact precautions for MDR-colonized patients
- Routine environmental cleaning
9. Ventilator Circuit Management
- Change circuits only when visibly soiled or malfunctioning (not on scheduled intervals)
- Drain condensation away from patient
- Heat-moisture exchangers (HME) rather than heated humidifiers reduce circuit colonization
10. Avoid Re-intubation
- Non-invasive ventilation (NIV) as bridge to prevent re-intubation where appropriate
- Careful extubation planning reduces failed extubation and need for re-intubation
Summary Table
| Feature | Detail |
|---|---|
| Definition | Pneumonia ≥48 h after mechanical ventilation |
| Most common ICU infection | Yes; ~10% of ICU patients at any time |
| Key pathogen (MDR) | P. aeruginosa, MRSA, Acinetobacter, ESBL-GNR |
| Early VAP (<5 days, no MDR risk) | Monotherapy (pip-tazo, cefepime, or carbapenem) |
| Late VAP / MDR risk | Triple therapy: β-lactam + aminoglycoside/FQ + vancomycin/linezolid |
| MRSA treatment | Vancomycin (AUC-guided) or linezolid |
| Duration | 7-8 days for most; longer for bacteremia/necrotizing |
| Best prevention | Minimize ventilation duration; HOB 30-45°; SSD; chlorhexidine oral care; daily SBT |
| De-escalation | Always at 48-72 h based on cultures |
| Key monitoring tool | PCT trend; clinical response |
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 131 - Hospital-Acquired and Ventilator-Associated Pneumonia
This is a shared conversation. Sign in to Orris to start your own chat.