20 marks university answer clinical Cardiopulmonary conditions Q) Pneumonectomy Different types of incisions used
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed for a thorough 20-mark university answer. Let me compose the complete response.
Pneumonectomy - Different Types of Incisions Used
(20 Marks - Clinical Cardiopulmonary Conditions)
Definition and Introduction
Pneumonectomy is the surgical removal of an entire lung. It is indicated primarily for non-small cell lung cancer (NSCLC) that cannot be managed by a lesser resection (lobectomy or segmentectomy), for certain benign destructive lung diseases (bronchiectasis, destroyed lung from tuberculosis), and for mesothelioma (extrapleural pneumonectomy). The choice of incision is central to the procedure - it must provide adequate exposure, allow vascular and bronchial control, and minimize postoperative morbidity.
The standard rule: thoracotomy for pneumonectomy is usually performed through a standard posterolateral incision. (Miller's Anesthesia, 10e)
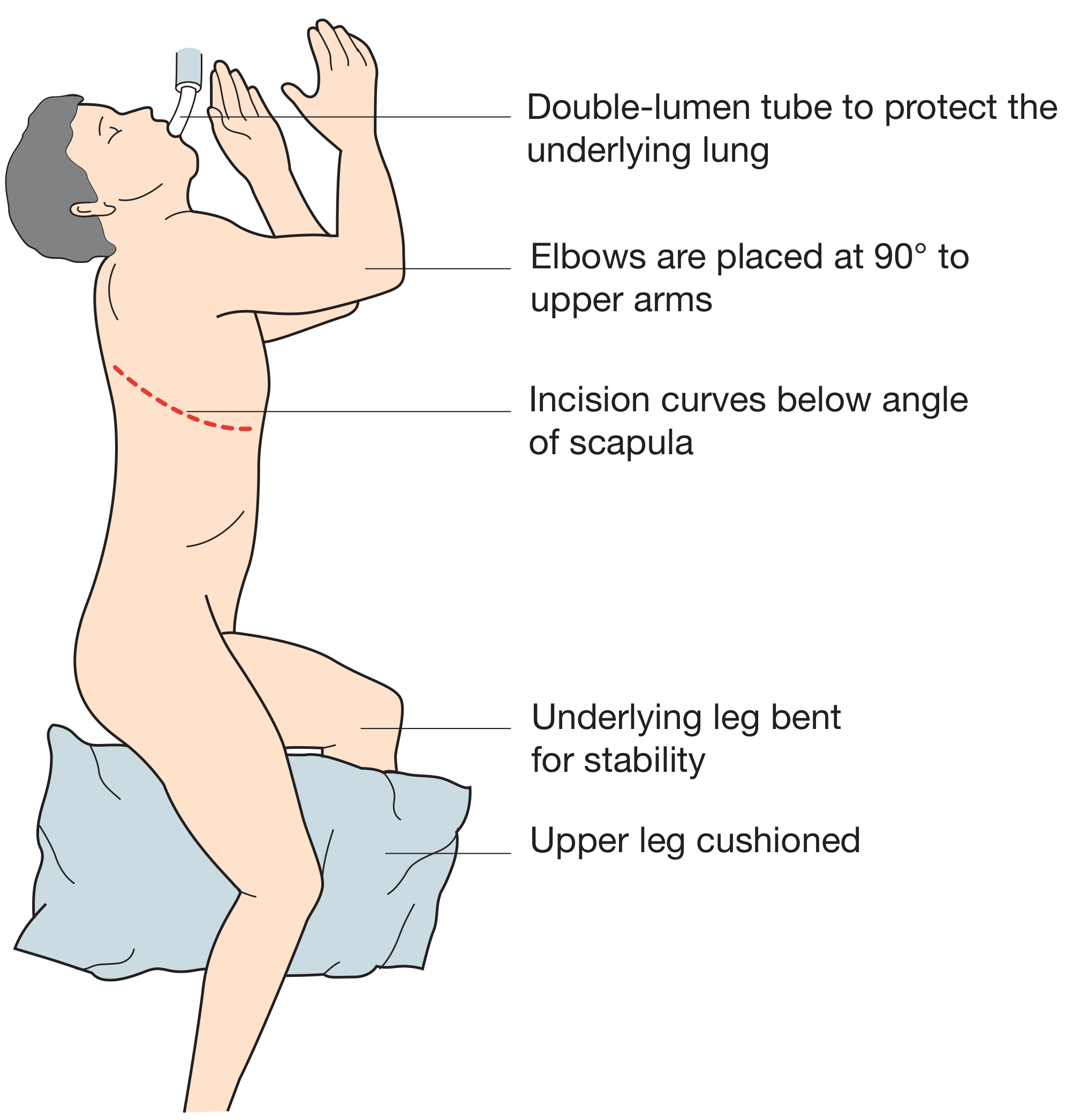
Patient Positioning
Before any incision, the patient is placed in the lateral decubitus position with the operative side uppermost. A double-lumen endobronchial tube is inserted to allow single-lung (one-lung) ventilation (OLV) of the contralateral lung during surgery. Elbows are placed at 90° to the upper arms, the underlying leg is bent for stability, and the upper leg is cushioned with a pillow (Bailey and Love's Short Practice of Surgery, 28e).
Types of Incisions Used for Pneumonectomy
1. Standard Posterolateral Thoracotomy (Most Common - Gold Standard)
This is the classic and most commonly used incision for pneumonectomy.
Position: Lateral decubitus (affected side up)
Incision line:
- Begins anteriorly below the level of the nipple (or inframammary fold in females)
- Passes 1-2 cm below the tip of the scapula
- Extends posteriorly and superiorly between the medial border of the scapula and the spine
Layers divided (deep to superficial):
- Skin and subcutaneous tissue
- Latissimus dorsi muscle - divided in line with the skin incision using coagulating diathermy
- Serratus anterior muscle - if divided, it should be cut close to its attachment to ribs 6, 7, and 8; alternatively it can be mobilized along its inferior border and left intact
- Trapezius and rhomboid fibers (partially)
- Sixth rib periosteum - scored near its upper border with diathermy; periosteal elevator is used to lift the periosteum off the superior border of the rib
- Intercostal muscles - cut just above the rib upper border
- Pleura - entered by blunt dissection
The chest is entered through the fifth or sixth intercostal space. A rib spreader (Finochietto retractor) is inserted gently to prevent fracture.
Advantages:
- Excellent exposure of the entire lung, hilum, and mediastinal structures
- Best access for lymph node dissection (stations 7, 10, 11)
- Optimal control of pulmonary vessels and main bronchus
- Allows conversion to more extensive procedures if needed
Disadvantages:
- Requires division of major chest wall muscles (latissimus dorsi, serratus anterior)
- Significant postoperative pain
- Total respiratory compliance may fall by up to 75%; work of breathing increases; lung volumes decline dramatically due to chest wall trauma, rib retraction/resection, and muscle transection (Fishman's Pulmonary Diseases and Disorders, 2-Volume Set)
- Longer recovery time
Sources: Bailey and Love's, 28e; Miller's Anesthesia, 10e; Fishman's Pulmonary Diseases
2. Anterolateral Thoracotomy
Position: Supine or slight lateral tilt
Incision line:
- Curvilinear incision underneath the inferior border of the pectoralis major muscle at the inframammary fold
- In females, follows the inframammary crease
- Extends from the lateral edge of the sternum to the posterior axillary line over the fourth or fifth intercostal space
Layers divided:
- Subcutaneous tissue
- Pectoralis major and minor muscles
- Intercostal muscles
- Pleura
Advantages:
- Rapid access - does not require major muscle division posteriorly
- Used for emergency thoracotomy (e.g., penetrating chest wounds, cardiac arrest, massive hemothorax)
- Can be quickly converted to a clamshell incision by extending to the contralateral side
- Good access to the left ventricle, anterolateral walls of the right ventricle, both atria, and allows aortic cross-clamping
Disadvantages:
- Limited posterior and mediastinal exposure compared to posterolateral approach
- Not ideal for elective pneumonectomy unless combined with other approaches
- Posterolateral wall of the right ventricle and posterior walls of both ventricles are harder to access
Use in pneumonectomy: Used when urgent access is required or as part of the clamshell approach. For elective pneumonectomy, the posterolateral approach is preferred.
Sources: Fischer's Mastery of Surgery, 8e; Bailey and Love's, 28e
3. Muscle-Sparing Thoracotomy (Axillary / Muscle-Sparing Variant)
This is a modification of the standard approach designed to reduce chest wall morbidity.
Types:
- Vertical axillary (muscle-sparing) incision: Made anterior to the latissimus dorsi muscle; enters the chest through the fourth intercostal space; the latissimus dorsi is retracted rather than divided
- Lateral muscle-sparing thoracotomy: The latissimus dorsi is retracted posteriorly; serratus anterior is split (not transected) along its fiber direction
Position: Lateral decubitus
Advantages:
- Significantly less postoperative pain
- Preservation of shoulder girdle function
- Faster recovery
- Less respiratory dysfunction postoperatively (less reduction in vital capacity and FEV1)
- Cosmetically superior scar
Disadvantages:
- Exposure may be more limited, particularly for large tumors or extensive hilar dissection
- Requires a skilled surgical team to optimize retraction for adequate visualization
Note: Although a posterolateral thoracotomy is the classic incision for lobectomies and pneumonectomies, anterolateral and muscle-sparing thoracotomies are increasingly used (Miller's Anesthesia, 10e).
4. Median Sternotomy
Position: Supine
Incision line:
- Vertical midline skin incision from the suprasternal notch to just below the tip of the xiphoid process
- Sternum divided in the midline using an oscillating/sternal saw
- Sternal retractor spreads the sternum approximately 8-10 cm
Layers divided:
- Skin and subcutaneous tissue
- Periosteum
- Sternum (divided by saw)
- Pericardium can be opened; pleura on either side can be opened to access the hemithorax
Closure: Stainless steel wires re-approximate the sternum.
Advantages:
- Excellent exposure of the heart, superior vena cava, aortic root, pulmonary vessels, and pulmonary hilae bilaterally
- Incision can be extended into the anterior cervical region or supraclavicular fossa to enhance exposure of the great vessels
- Avoids major chest wall muscles
- Good access to the mediastinum
- Traditionally used for bilateral pulmonary metastasectomy, mediastinal tumors, and cardiac surgery
Disadvantages:
- Takes longer to open than anterolateral thoracotomy
- Access to the left and right lung is more limited than posterolateral thoracotomy
- Descending aorta, trachea, and esophagus cannot be reached through a sternotomy
- Risk of sternal dehiscence and mediastinitis
Use in pneumonectomy: Occasionally used for pneumonectomy when combined cardiac/pulmonary procedures are needed, or for bilateral resection planning.
Sources: Sabiston Textbook of Surgery; Fischer's Mastery of Surgery, 8e; Miller's Anesthesia, 10e
5. Clamshell (Bilateral Anterior Thoracotomy + Transverse Sternotomy)
Position: Supine
Incision line:
- Two anterior thoracotomy incisions made bilaterally in the inframammary fold
- Connected by a transverse division of the sternum at the fourth intercostal space
- Both internal mammary arteries (LIMA and RIMA) are ligated
Advantages:
- Largest single incision for thoracic access - provides excellent bilateral exposure
- Ideal for accessing both lung hila, the entire heart, and great vessels
- Preferred for bilateral lung transplantation in many centers
- Allows management of large mediastinal tumors or bilateral hilar dissections
- Can be rapidly created from a left anterolateral thoracotomy by extending to the right
Disadvantages:
- Larger than median sternotomy - typically more painful postoperatively
- Requires ligation of both internal mammary arteries
- Higher wound morbidity and postoperative complications
- Reserved for specific indications
Use in pneumonectomy: Used for extrapleural pneumonectomy for mesothelioma in selected centers, bilateral procedures, and as an emergency extension of anterolateral thoracotomy.
Sources: Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11e; Harrison's, 22e
6. Video-Assisted Thoracoscopic Surgery (VATS) Approach
Incision type: Minimally invasive - multiple small (1-2 cm) port incisions
Incision placement:
- A utility incision (approximately 3-4 cm) placed at one intercostal space
- 2-3 additional port sites (each 1-2 cm) for camera and instruments
- Careful placement is relative to the patient's ribs, arm, diaphragm, and scapula
- Ribs are NOT spread
Technique:
- A high-definition camera and long thoracoscopic instruments are used
- Improved lighting and optics create excellent visualization, often superior to open approaches
Advantages:
- Reduced postoperative pain
- Shorter length of hospitalization
- Faster recovery and return to activity
- Less chest wall trauma - no major muscle division
- Better cosmetic outcome
Disadvantages:
- Technically demanding - requires specialized training and equipment
- Limited access in cases of dense adhesions or difficult hilar anatomy
- Conversion to open thoracotomy may be required
Note: VATS is increasingly used for pneumonectomy, and robotic-assisted thoracoscopic surgery (RATS) has emerged as a minimally invasive extension of VATS in the last two decades. (Miller's Anesthesia, 10e; Sabiston Textbook of Surgery)
Comparative Summary Table
| Incision | Position | Intercostal Space | Key Muscles Divided | Best Use |
|---|---|---|---|---|
| Posterolateral thoracotomy | Lateral decubitus | 5th or 6th | Latissimus dorsi, serratus anterior | Standard elective pneumonectomy |
| Anterolateral thoracotomy | Supine/slight lateral | 4th or 5th | Pectoralis major | Emergency, rapid access |
| Muscle-sparing thoracotomy | Lateral decubitus | 4th | None divided (retracted) | Elective with less morbidity |
| Median sternotomy | Supine | N/A (bone) | None (sternum divided) | Cardiac + pulmonary, mediastinal |
| Clamshell | Supine | 4th bilateral | None + IMA ligation | Bilateral procedures, transplant |
| VATS | Lateral decubitus | Multiple small ports | None | Minimally invasive pneumonectomy |
Bronchial Stump Management Post-Incision
Regardless of incision type, after the lung is mobilized and vessels are divided and stapled, the main bronchus is stapled and divided:
- Right main bronchus: divided at approximately the third cartilage counted from the carina
- Left main bronchus: also divided at the third cartilage; a longer bronchial stump must be avoided as it creates a pocket for secretion accumulation
- A TA stapler is placed in the "Sweet direction" and fired orthogonally to the longitudinal axis of the bronchus
- Bronchial stump is tested for air leaks at 20 cmH2O positive pressure (Fischer's Mastery of Surgery, 8e)
Key Postoperative Consideration Related to Incision
The type of incision directly impacts postoperative respiratory function:
- The standard posterolateral thoracotomy causes up to 75% fall in total respiratory compliance
- Work of breathing increases substantially
- Lung volumes (FRC, VC, FEV1) decline dramatically
- Muscle-sparing and VATS approaches significantly reduce this morbidity
- Post-pneumonectomy space management (mediastinal balancing, drainage systems) is mandatory regardless of incision type (Miller's Anesthesia, 10e)
Conclusion
The standard posterolateral thoracotomy remains the classic incision for elective pneumonectomy, offering superior exposure and control of hilar structures. The choice of incision, however, must be individualized based on the surgical indication (elective vs. emergency), extent of disease, patient physiologic reserve, need for bilateral access, and surgeon expertise. Minimally invasive approaches (VATS, RATS) are increasingly favored for select patients due to reduced morbidity, while median sternotomy and clamshell incisions serve specific indications requiring bilateral or mediastinal access.
References:
- Miller's Anesthesia, 10e - Pneumonectomy section
- Bailey and Love's Short Practice of Surgery, 28e - Thoracotomy chapter
- Fischer's Mastery of Surgery, 8e - Left Pneumonectomy and Surgical Technique: Incisions
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice - Thoracic Incisions
- Schwartz's Principles of Surgery, 11e - Operative Approaches and Exposure
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set - Lung Resection
- Harrison's Principles of Internal Medicine, 22e - Recipient Operation (transplant incisions)
This is a shared conversation. Sign in to Orris to start your own chat.