Brachial plexus clinical correlations
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the material needed for a comprehensive, well-illustrated answer. Let me compile the full clinical correlations guide.
Brachial Plexus: Clinical Correlations
Anatomy Review
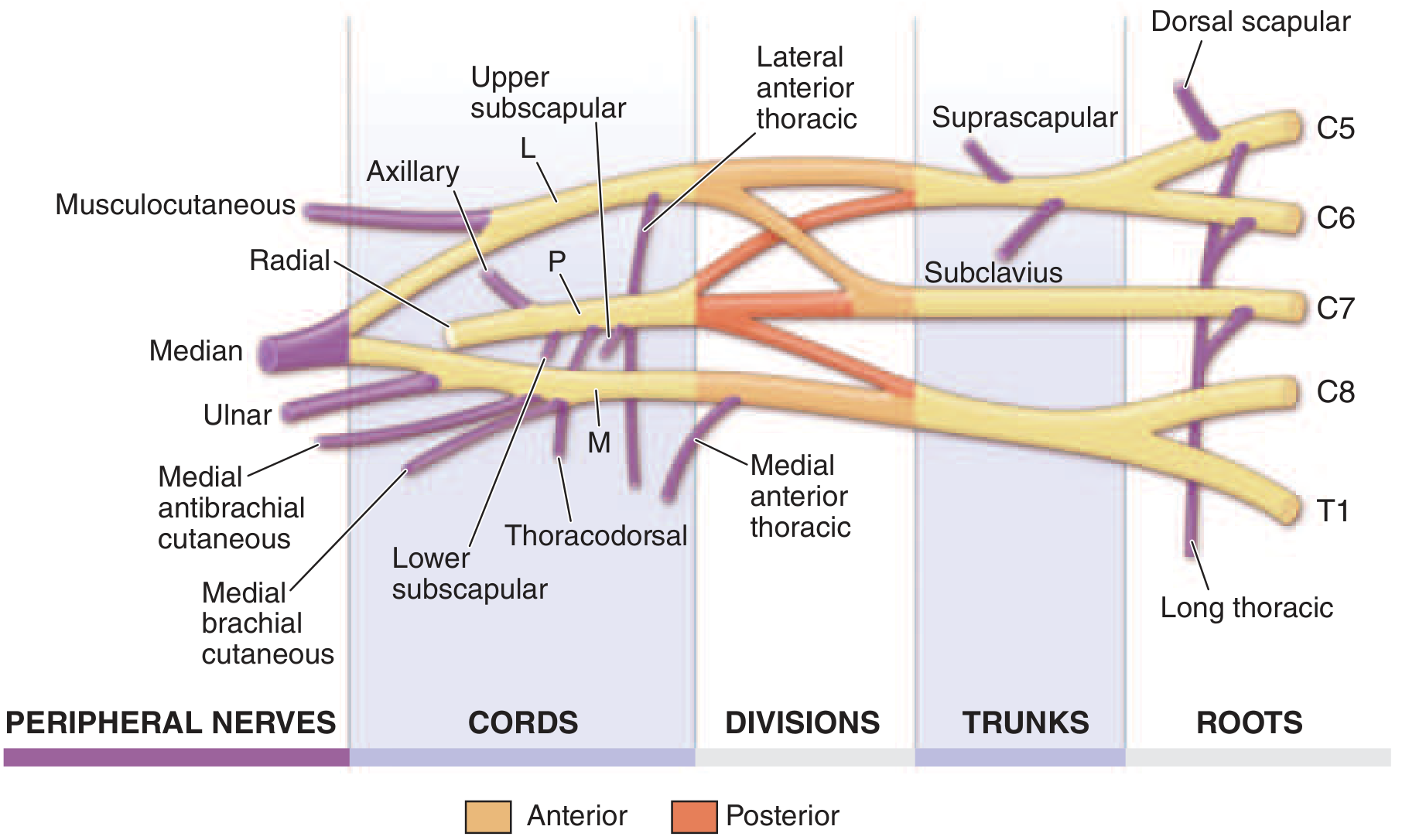
The brachial plexus is formed by the anterior rami of C5-T1, organized into:
Roots → Trunks → Divisions → Cords → Terminal nerves
| Level | Formation |
|---|---|
| Upper trunk | C5 + C6 |
| Middle trunk | C7 alone |
| Lower trunk | C8 + T1 |
| Lateral cord | Anterior divisions of upper + middle trunks |
| Medial cord | Anterior division of lower trunk |
| Posterior cord | All three posterior divisions |
The roots pass between the anterior and middle scalene muscles, posterior to the subclavian artery. In the axilla, the cords surround the axillary artery and give rise to terminal branches.
Here is the full anatomical diagram from Gray's Anatomy for Students:

And the complete schematic from Harrison's 22e showing all branches:
1. Erb-Duchenne Palsy (Upper Trunk: C5, C6)
Mechanism: Forcible widening of the angle between the neck and shoulder - stretching the upper trunk. Classic causes:
- Birth injury - traction on the head while shoulder is arrested (shoulder dystocia)
- Fall on a load on the shoulder in adults
- Glenohumeral dislocation
Deformity: "Waiter's tip" / "Bellhop's tip"
- Arm hangs at the side, adducted and internally rotated
- Elbow extended, forearm pronated, wrist flexed
- This posture results from paralysis of: deltoid (abduction), supraspinatus, infraspinatus (external rotation), biceps (flexion and supination), and brachioradialis
Signs:
- Absent/diminished biceps reflex (C5, C6)
- Asymmetric Moro reflex in neonates
- Hand and finger movements are preserved (C8, T1 intact)
Prognosis (best of the three types): >90% of neonatal cases resolve without intervention. Recovery within 2-4 weeks after birth is a good prognostic sign. Lack of biceps function at 6 months and presence of Horner syndrome indicate poor prognosis.
Source: Bradley and Daroff's Neurology in Clinical Practice; Miller's Review of Orthopaedics 9th Ed; Neuroanatomy through Clinical Cases 3rd Ed.
2. Klumpke's Palsy (Lower Trunk: C8, T1)
Mechanism: Forcible hyperabduction of the arm (e.g., grabbing a fixed object while falling, or breech delivery with arm traction).
Deformity: "Claw hand"
- Weakness of intrinsic hand muscles (interossei, lumbricals, hypothenar, thenar)
- Fingers extended at MCPJs, flexed at IPJs (due to loss of lumbrical/interosseous balance)
- Resembles ulnar nerve palsy but involves the entire hand
Additional features:
- Horner syndrome (ptosis, miosis, enophthalmos, anhidrosis) - because T1 sympathetic fibers travel with this root before joining the sympathetic chain
- Absent grasp reflex in neonates
- Sensory loss on medial forearm and hand (T1 distribution)
Prognosis: Poor - presence of Horner syndrome is an especially bad sign.
Source: S Das Manual on Clinical Surgery 13th Ed; Miller's Review of Orthopaedics 9th Ed; Color Atlas of Human Anatomy.
3. Total Plexus Palsy (C5-T1)
Mechanism: Severe traction or avulsion injuries (high-speed motorcycle accidents, severe obstetric trauma).
Features:
- Complete flaccid paralysis of the entire upper limb ("flail arm")
- Global sensory loss
- Horner syndrome invariably present (T1 involvement)
- Worst prognosis of all three types
4. Summary Table: Three Palsy Types
| Feature | Erb-Duchenne | Klumpke | Total Plexus |
|---|---|---|---|
| Roots | C5, C6 | C8, T1 | C5-T1 |
| Trunk | Upper | Lower | All |
| Mechanism | Neck-shoulder traction | Arm hyperabduction | Severe traction/avulsion |
| Deformity | Waiter's tip | Claw hand | Flail arm |
| Hand spared? | Yes | No | No |
| Horner syndrome | No | Yes | Yes |
| Reflex lost | Biceps | Finger flexors/grasp | All |
| Prognosis | Best | Poor | Worst |
5. Pancoast Tumor (Superior Sulcus Tumor)
An apical lung tumor encroaching on the lower trunk of the brachial plexus from below.
"Pancoast Syndrome" comprises:
- Horner syndrome (ptosis, miosis, enophthalmos, anhidrosis) - pressure on the sympathetic chain
- Shooting pain down the arm + later lower brachial plexus paralysis - pressure on lower trunk (C8, T1)
- Sensory disturbance on medial forearm and hand
- Weakness and atrophy of intrinsic hand muscles
- Distension of veins of face/neck/thorax - from SVC compression
- Rib and vertebral body destruction may be visible on imaging
Key point: Insidious onset, often misdiagnosed as cervical disc disease or shoulder pathology. Chest CT/MRI shows extension of tumor into the plexus. The lower trunk is preferentially affected because it is closest to the lung apex.
Source: S Das Manual on Clinical Surgery 13th Ed; Harrison's Principles of Internal Medicine 22e (2025).
6. Thoracic Outlet Syndrome (TOS)
Compression of the brachial plexus (and subclavian vessels) as they pass through the thoracic outlet. Three anatomic spaces are involved:
- Interscalene triangle (between anterior and middle scalene, above rib I) - artery and nerves
- Costoclavicular space (between clavicle and rib I) - vein
- Subcoracoid area (beneath pectoralis minor) - artery, vein, nerves
Three types:
| Type | Involved Structure | Features |
|---|---|---|
| Neurogenic (>90%) | Lower brachial plexus | Medial forearm/hand numbness + weakness of intrinsic hand muscles; most common in middle-aged females |
| Arterial | Subclavian artery | Hand/arm fatigue, weakness, pallor, claudication, paresthesias; thrombosis/distal embolization |
| Venous | Subclavian vein | Arm edema, cyanosis, effort-induced thrombosis (Paget-Schroetter syndrome) |
Causes: Cervical rib (articulating with the first rib), anomalous scalene muscles, repetitive trauma, chronic inflammatory changes.
Diagnosis: Clinical + chest/cervical spine X-ray (to detect cervical rib) + CT/MRI + duplex ultrasound + electrophysiologic evaluation.
Positional maneuvers (Adson's, Roos test) can provoke symptoms in clinic.
Source: Sabiston Textbook of Surgery 11th Ed; Bradley and Daroff's Neurology in Clinical Practice.
7. Parsonage-Turner Syndrome (Neuralgic Amyotrophy / Immune-Mediated Brachial Plexus Neuropathy)
Pathogenesis: Immune-mediated (post-infectious, post-vaccination, post-surgical, idiopathic).
Presentation:
- Acute onset of severe shoulder/arm pain lasting days to weeks - often so severe the patient cannot move the arm
- As pain subsides, weakness and atrophy become apparent (often involving deltoid, serratus anterior, supraspinatus/infraspinatus)
- Sensory loss in a patchy distribution
- Upper trunk most commonly involved - but single terminal nerves (long thoracic, suprascapular, axillary, anterior interosseous, phrenic) can be affected in isolation
Diagnosis: Clinical - EMG/NCS confirms and localizes. MRI may show nerve signal changes.
Treatment: Empirical glucocorticoids for severe pain in the acute period; recovery over months to years.
Source: Harrison's Principles of Internal Medicine 22e (2025).
8. Birth Injury - Obstetric Brachial Plexus Palsy
Incidence: 0.4-4 per 1000 live births; approximately 2 per 1000 births still sustain brachial plexus injury.
Risk factors: Large neonate, shoulder dystocia, forceps delivery, breech position, prolonged labor.
Additional associations: Diaphragmatic paralysis (C3-C5 phrenic nerve involvement), fractured clavicle/humerus, cervical cord injury, facial palsy.
Sequelae (when persistent):
- Progressive glenoid hypoplasia in 70% of children with significant internal rotation contracture
- Posterior subluxation of humeral head with glenoid erosion
Surgical options:
- Microsurgical nerve grafting
- L'Episcopo procedure (latissimus dorsi + teres major transfer for external rotation)
- Steindler flexorplasty / Clark pectoral transfer (elbow flexion)
- Subscapularis release for internal rotation contracture (best before age 2)
- Proximal humerus rotational osteotomy (after age 5)
Source: Miller's Review of Orthopaedics 9th Ed; Bradley and Daroff's Neurology in Clinical Practice.
9. Neoplastic Brachial Plexopathy
| Tumor Type | Typical Level Involved | Features |
|---|---|---|
| Pancoast lung tumor | Lower trunk (C8, T1) | Pain + Horner + intrinsic hand weakness |
| Breast cancer (axillary lymph nodes) | Variable | Metastatic spread into nearby nerves |
| Lymphoma (cervical/axillary nodes) | Can infiltrate any level | Depends on location |
| Primary nerve tumors (schwannoma, neurofibroma, neurinoma) | Any | Slow-growing, less aggressive |
Key distinction - radiation plexopathy vs. metastatic plexopathy:
- Radiation plexopathy: Upper trunk, myokymic discharges on EMG, painless
- Neoplastic plexopathy: Lower trunk, painful, no myokymia
Source: Harrison's Principles of Internal Medicine 22e (2025).
10. Perioperative Brachial Plexopathy
Occurs in up to 5% of patients after median sternotomy (open-heart surgery, thoracotomy).
Mechanism: Stretch of the lower trunk during sternal retraction.
Features: Sensory disturbance on medial forearm + hand, weakness of intrinsic hand muscles. Most recover within a few months as it is a traction neurapraxia.
Source: Harrison's Principles of Internal Medicine 22e (2025).
11. "Stinger" / "Burner" Injury (Sports)
Common in contact sports (football, wrestling). Transient traction neurapraxia of the brachial plexus from neck or shoulder injury. Produces a brief burning sensation and weakness radiating down the arm. Usually resolves within minutes, but repetitive injuries can cause cumulative damage.
12. Key Branches and Their Individual Clinical Correlates
| Nerve | Origin | Clinical Lesion |
|---|---|---|
| Long thoracic (C5-C7) | Roots | Serratus anterior palsy → winged scapula |
| Dorsal scapular (C5) | Root | Rhomboid + levator scapulae weakness |
| Suprascapular (C5, C6) | Upper trunk | Supraspinatus + infraspinatus weakness; suprascapular notch entrapment |
| Axillary (C5, C6) | Posterior cord | Deltoid paralysis → shoulder abduction loss; after shoulder dislocation or surgical neck of humerus fracture |
| Musculocutaneous (C5-C7) | Lateral cord | Biceps + brachialis weakness; sensory loss lateral forearm |
| Median (C6-T1) | Lateral + Medial cord | "Hand of oath" (proximal lesion); carpal tunnel syndrome (distal) |
| Ulnar (C8, T1) | Medial cord | Claw hand (ring and little fingers); cubital tunnel syndrome |
| Radial (C5-T1) | Posterior cord | Wrist drop (spiral groove); Saturday night palsy |
Quick Clinical Pearl
Horner syndrome + arm involvement = always think brachial plexus at the T1 root level. The T1 root carries both the sympathetic fibers to the superior cervical ganglion (affecting the eye and face) and motor fibers to intrinsic hand muscles. Its presence indicates lower trunk involvement - pointing to Klumpke's palsy, Pancoast tumor, or total plexus avulsion.
Sources: Gray's Anatomy for Students (4th Ed); Schwartz's Principles of Surgery 11th Ed; Harrison's Principles of Internal Medicine 22e (2025); Bradley and Daroff's Neurology in Clinical Practice; Miller's Review of Orthopaedics 9th Ed; S Das Manual on Clinical Surgery 13th Ed; Sabiston Textbook of Surgery 11th Ed; Neuroanatomy through Clinical Cases 3rd Ed; Color Atlas of Human Anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.