Premalignant lesions of penis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Premalignant Lesions of the Penis
Penile premalignant lesions are divided into two broad categories based on their pathogenesis: HPV-related and non-HPV (inflammatory) related. In one large series, 42% of patients with penile squamous cell carcinoma had a history of pre-existing penile lesions.
Classification Overview
| Category | Lesions |
|---|---|
| HPV-related | Penile Intraepithelial Neoplasia (PeIN): Erythroplasia of Queyrat, Bowen's Disease, Bowenoid Papulosis |
| Non-HPV / Inflammatory | Cutaneous Horn, Leukoplakia, Balanitis Xerotica Obliterans (Lichen Sclerosus), Pseudoepitheliomatous Keratotic and Micaceous Balanitis (PKMB) |
I. Penile Intraepithelial Neoplasia (PeIN / PIN)
PeIN is the umbrella term for squamous carcinoma in situ of the penis. All forms share the histological features of CIS - confined to the epithelium with an intact basement membrane. HPV (especially HPV-16) is identified in ~90% of cases.
1. Erythroplasia of Queyrat (EQ)
- Definition: CIS involving the glans penis or prepuce of uncircumcised men
- Named after: Queyrat, who first described it in 1911
- Clinical: Red, velvety, well-marginated lesion; may ulcerate; may be associated with discharge and pain
- Histology:
- Normal mucosa replaced by atypical hyperplastic cells
- Disorientation, vacuolation, multiple hyperchromatic nuclei, mitotic figures at all levels
- Epithelial rete extended into submucosa - elongated, broadened, bulbous
- Submucosa: capillary proliferation and ectasia with inflammatory infiltrate rich in plasma cells (distinguishes from chronic balanitis)
- Malignant transformation: 10-33% progress to invasive carcinoma
- Note: No associated visceral malignancy
2. Bowen's Disease (BD)
- Definition: CIS involving the penile shaft or remainder of genitalia/perineal region
- Named after: Bowen (1912), who described it as an intraepithelial neoplasm associated with subsequent internal malignancy - however, subsequent case-control studies showed no association with internal tumors, so penile CIS does not warrant a search for internal malignancy
- Clinical: Sharply defined plaques of scaly erythema on the penile shaft; crusted or ulcerated variants; may mimic bowenoid papulosis, nummular eczema, psoriasis, or superficial BCC
- Histology: Dysplastic squamous cells with large hyperchromatic irregular nuclei, lacking orderly maturation; numerous mitoses (some atypical) (Fig. 21.13 from Robbins)
- Malignant transformation: Invasive carcinoma in ~5-10% of untreated patients; metastasis extremely rare but reported
3. Bowenoid Papulosis (BP)
- Definition: Histologically identical to CIS but a clinically benign course
- First described by: Kopf and Bart (1977)
- Clinical: Multiple reddish-brown papular lesions on the penis; affects younger, sexually active adults (peak incidence in the 3rd decade)
- Etiology: HPV-16 (now classified as HSIL - high-grade squamous intraepithelial lesion)
- Key distinction from Bowen's Disease:
- Multiple (not solitary) lesions
- Younger patients
- Virtually never progresses to invasive carcinoma
- Usually regresses spontaneously
- Histology: Indistinguishable from Bowen's disease (hence the importance of clinical context)
II. Non-HPV / Inflammatory Premalignant Lesions
4. Leukoplakia
- Appearance: White plaque typically involving the meatus; most common in diabetic patients
- Histology: Acanthosis, hyperkeratosis, parakeratosis
- Significance: May precede or occur simultaneously with penile carcinoma
5. Balanitis Xerotica Obliterans (BXO) / Male Lichen Sclerosus (LS)
- Definition: A genital variation of lichen sclerosus et atrophicus; non-HPV related
- Clinical:
- Whitish patch on the prepuce or glans, often involving the meatus and fossa navicularis
- Lesions may be multiple with a mosaic appearance
- Meatus appears white, indurated, edematous
- Glanular erosions, fissures, meatal stenosis
- Symptoms: pain, dyspareunia, pruritus, painful erections, urinary obstruction
- Most common in uncircumcised men, middle-aged (rarely in boys)
- Almost never occurs in males circumcised at birth
- Histology:
- Atrophic epidermis with loss of rete pegs
- Homogenization of collagen in upper third of dermis
- Zone of lymphocytic and histiocytic infiltration
- Malignant risk: Found in 28-50% of patients with penile cancer; penile cancer develops in 2.3-5.8% of men with LS
- Etiology: Unknown; autoimmunity, genetic factors, chronic inflammation, possibly Borrelia burgdorferi (identified in 63% of LS tissues in one study - causation unproven)
- Treatment: Clobetasol propionate cream for 2-3 months; meatal stenosis may require repeated dilations, corticosteroid injection, or reconstructive surgery
6. Cutaneous Horn
- Appearance: Animal horn-like protuberance from overgrowth and cornification of epithelium
- Histology: Extreme hyperkeratosis, dyskeratosis, acanthosis
- Key point: The horn itself is not the concern - the underlying lesion matters:
- Benign: seborrheic keratosis, viral warts
- Premalignant: solar keratosis, Bowen disease
- Malignant: SCC found at the base in up to 33% of penile horns
- Predisposing factors: Chronic inflammation, trauma, poor hygiene, viral infection
- Treatment: Surgical excision with a margin of normal tissue around the base; full histologic evaluation essential; close follow-up (may recur or transform)
7. Pseudoepitheliomatous Keratotic and Micaceous Balanitis (PKMB)
- Appearance: Hyperkeratotic, scaly, micaceous (mica-like, silver-white, layered) growth on the surface of the glans penis
- Histology: Marked hyperkeratosis, parakeratosis, pseudoepitheliomatous hyperplasia
- Differential diagnosis: Verrucous carcinoma, SCC, giant condyloma, penile horn, keratoacanthoma
- Staging (Krunic et al.):
- Initial plaque
- Late tumor stage
- Verrucous carcinoma
- Invasive squamous cell carcinoma
- Treatment: Topical 5-fluorouracil, surgical excision, laser ablation, or cryotherapy (based on stage); tends to recur as frank carcinoma with less invasive treatment - requires close follow-up and prompt excision
Histology Image: Condyloma Acuminatum (HPV-associated benign precursor)
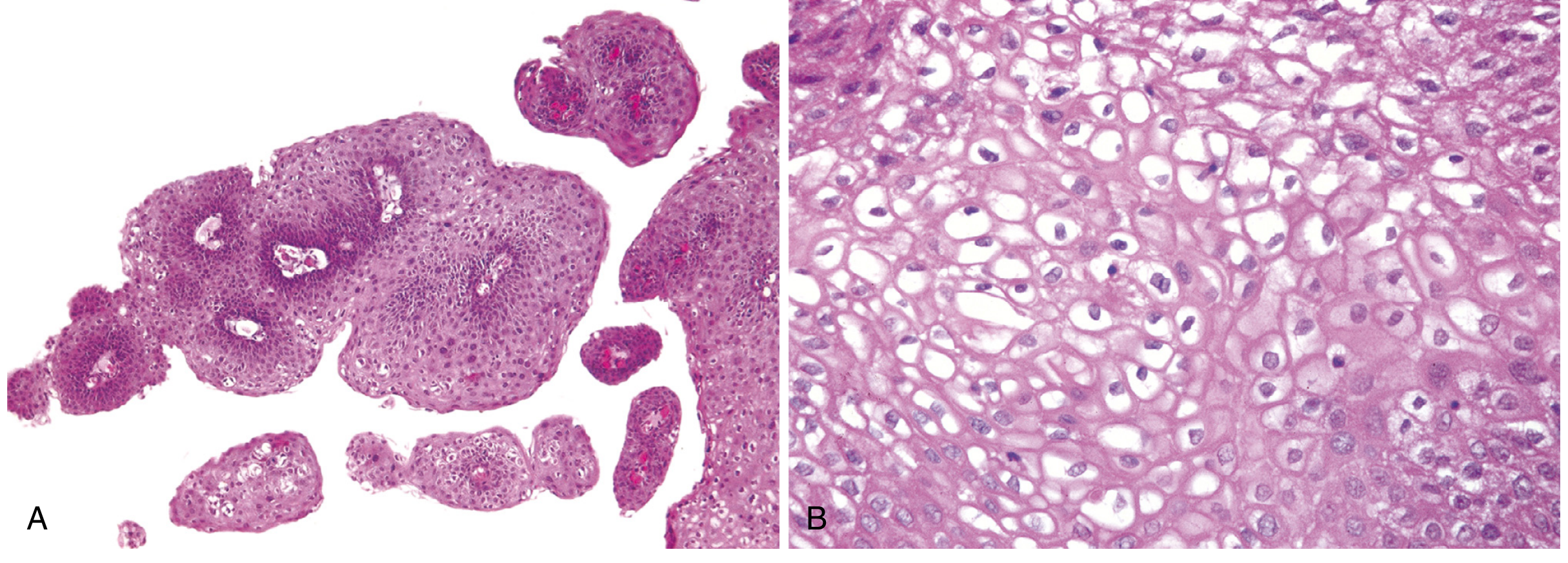
Condyloma acuminatum: (A) Papillary architecture and epidermal thickening; (B) Koilocytosis - perinuclear vacuolization characteristic of HPV infection (Robbins Pathology)
Treatment of PeIN (General Principles)
Treatment requires histopathologic confirmation with multiple biopsies of adequate depth to rule out invasion. Options include:
| Treatment | Notes |
|---|---|
| Circumcision / excision (5-mm margin) | For foreskin lesions |
| Glans resurfacing | Complete dissection of glans epithelium + subepithelial tissue; skin graft closure; low local recurrence |
| Topical 5-fluorouracil cream | Conservative; for superficial lesions |
| 5% imiquimod cream | Immunomodulatory; topical option |
| Nd:YAG / KTP / CO2 laser ablation | Excellent cosmetic and functional results |
| Radiation therapy | For lesions resistant to topical treatment; patients not fit for surgery |
Summary Table
| Lesion | Location | Key Feature | Malignant Risk | HPV |
|---|---|---|---|---|
| Erythroplasia of Queyrat | Glans/prepuce | Red, velvety plaque | 10-33% → invasive SCC | Yes (HPV-16) |
| Bowen's Disease | Penile shaft | Scaly erythematous plaque | ~5-10% → invasive SCC | Yes (HPV-16) |
| Bowenoid Papulosis | Penis (multiple) | Multiple papules, young adults | Virtually nil; regresses | Yes (HPV-16) |
| Leukoplakia | Meatus | White plaque, diabetics | Associated with SCC | No |
| BXO / Lichen Sclerosus | Glans/prepuce/meatus | White atrophic patch | 2.3-5.8% → SCC | No |
| Cutaneous Horn | Any | Horn-like protuberance | 33% underlying SCC | No |
| PKMB | Glans | Micaceous scaly growth | Progresses to SCC in stages | No |
Sources: Campbell-Walsh-Wein Urology (10th/11th ed.); Robbins, Cotran & Kumar Pathologic Basis of Disease; Smith and Tanagho's General Urology (19th ed.)
Difference between bowen and bowenoid papulosis
Based on what I just retrieved from the textbooks, I can answer this directly from the rich content already in context.
Bowen's Disease vs. Bowenoid Papulosis
These two conditions are histologically identical but clinically very different - this is the classic exam distinction.
Comparison Table
| Feature | Bowen's Disease (BD) | Bowenoid Papulosis (BP) |
|---|---|---|
| Age | Older males | Younger, sexually active adults (peak: 3rd decade) |
| Lesion number | Solitary | Multiple |
| Morphology | Single thickened, gray-white opaque plaque; velvety red if on glans | Multiple reddish-brown papular lesions |
| Location | Penile shaft, scrotum (less commonly glans) | Penis, vulva, perianal |
| Histology | Dysplastic squamous cells - large hyperchromatic irregular nuclei, disordered maturation, numerous mitoses (some atypical) | Identical to Bowen's disease - indistinguishable on biopsy alone |
| HPV type | HPV-16 (high risk) | HPV-16 (high risk) |
| Malignant potential | 5-10% progress to invasive SCC | Virtually nil - almost never progresses |
| Natural course | Does NOT regress spontaneously | Usually regresses spontaneously |
| Association with internal malignancy | Originally thought to be associated (Bowen, 1912) - but subsequent studies disproved this | None |
| Treatment | Active treatment required (excision, laser, 5-FU, imiquimod) | Often conservative / observation; spontaneous regression common |
The Key Paradox
Both BD and BP are:
- Caused by HPV-16
- Histologically indistinguishable (CIS-level changes, koilocytosis, disordered maturation, atypical mitoses)
Yet BP never becomes invasive and regresses spontaneously, while BD has a real risk of progression. The reason is not fully understood - it likely relates to host immune response differences, as BP occurs in younger, immunocompetent individuals.
Memory Hook
"Bowen = Big risk, Bowenoid = Benign course"
- Bowen: Solitary, Older, Shaft, 5-10% → SCC
- Bowenoid Papulosis: Multiple papules, Young adults, Regresses
Why Biopsy Alone Cannot Distinguish Them
Since the histology is identical, clinical context is essential for diagnosis:
- Multiple lesions in a young sexually active person → Bowenoid Papulosis
- Solitary plaque in an older man → Bowen's Disease
This makes clinical examination and patient history indispensable alongside pathology reports.
Sources: Campbell-Walsh-Wein Urology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Begingn tumours of penis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I have comprehensive content from the textbooks. Here is the full answer:
Benign Tumours of the Penis
Benign penile lesions can be broadly divided into epithelial (predominantly HPV-related) and non-epithelial (mesenchymal/vascular/inflammatory) types.
I. Epithelial / HPV-Related Benign Tumours
1. Condyloma Acuminatum (Genital Warts / Venereal Warts)
The most common benign penile tumour.
- Cause: HPV types 6 and 11 (low-risk, non-oncogenic)
- Sites in males: Glans, penile shaft, prepuce, meatus (most common sites). About 5% have urethral involvement, which may extend to the prostatic urethra. Rarely, bladder involvement occurs.
- Clinical appearance: Soft, papillomatous, friable growths. May be:
- Solitary on a pedicle, OR
- Multiple in a moruloid cluster on a broad base
- "Cauliflower-like" appearance
- Histology:
- Outer layer of keratinized tissue covering papillary fronds
- Fronds supported by connective tissue stroma
- Well-ordered rows of squamous epithelial cells
- Dermal lymphocytic infiltrate
- Koilocytes - pathognomonic for HPV: cells with an empty perinuclear cavity (halo) surrounding an atypical nucleus; prominent keratohyalin granules
- Diagnosis: Subclinical lesions detected by applying 5% acetic acid to penis - lesions turn white (acetowhite); flat lesions invisible on inspection become apparent. Biopsy confirms diagnosis.
- Malignant potential: Condylomata acuminata are not precancerous per se. However, malignant transformation to SCC has been reported, and they are associated with penile SCC.
Histology:
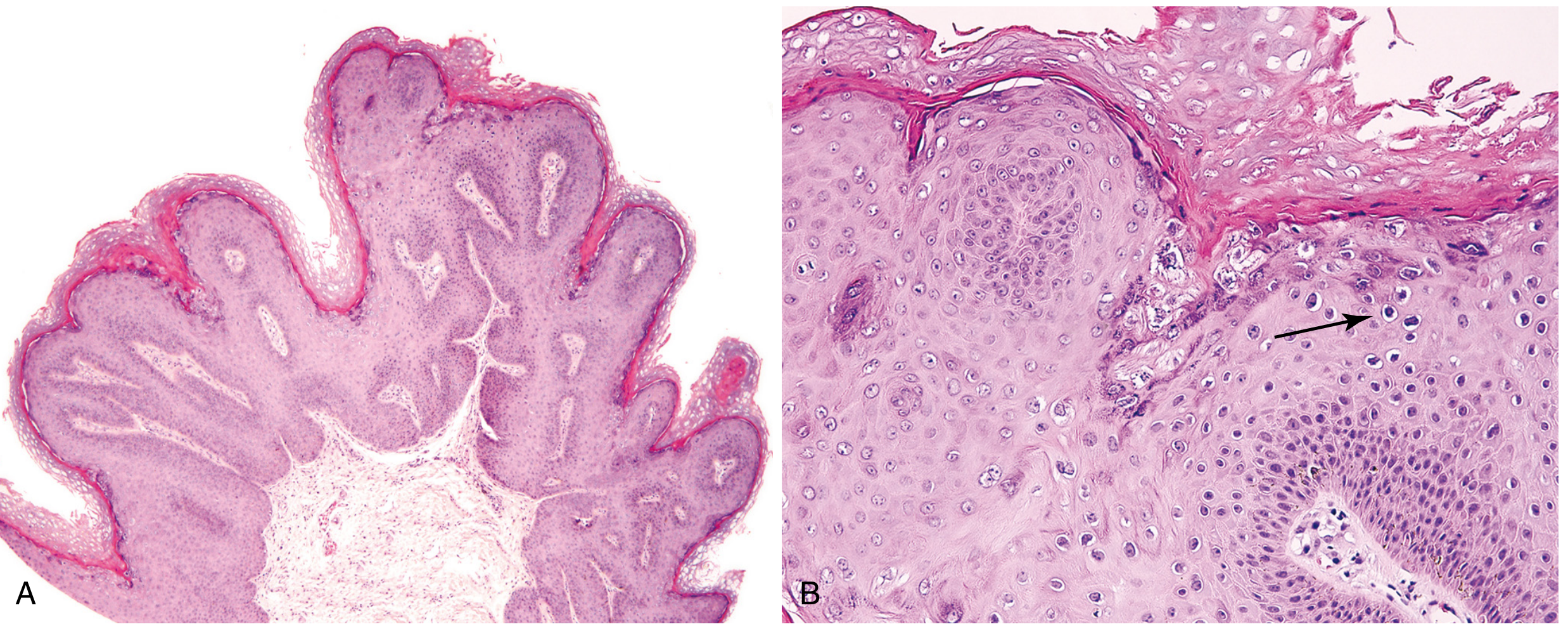
Fig: Condyloma acuminatum. (A) Exophytic papillary architecture. (B) Koilocytic atypia - perinuclear halos (arrow) characteristic of HPV infection. (Robbins Pathology)
Treatment options:
| Method | Notes |
|---|---|
| Imiquimod 5% cream | Treatment of choice - immune modulator, enhances NK cell activity |
| Podophyllotoxin 0.5% | Traditional topical agent |
| Trichloroacetic acid (35-85%) | Chemical destruction |
| Cryotherapy (liquid nitrogen) | Standard ablative therapy |
| CO2 laser | Good for extensive lesions |
| Electrofulguration | Surgical ablation |
| 5-FU cream (intraurethral) | Applied weekly x 3 weeks for urethral lesions |
| Cidofovir 1% gel | Antiviral; 47% complete response in trial |
| Interferon | Reserved for extensive, recalcitrant lesions |
| Circumcision | Removes preputial lesions and improves access |
Important: No treatment has been proven to reduce transmission to sexual partners or prevent progression to dysplasia/cancer. Recurrence is common after any treatment.
2. Buschke-Löwenstein Tumour (Giant Condyloma Acuminatum)
A distinct entity - not simply a large condyloma.
- First described: Buschke and Löwenstein (1925)
- Cause: HPV types 6 and 11 (same as condyloma)
- Key distinction from ordinary condyloma:
- Ordinary condylomata, regardless of size, remain superficial and never invade adjacent tissue
- Buschke-Löwenstein tumour displaces, invades, and destroys adjacent structures by compression
- Does not metastasize (unlike true carcinoma)
- Location: Glans, prepuce, perineum; also perianal region
- Histology:
- Luxuriant mass of broad, rounded rete pegs extending deep into tissue
- Composed of well-differentiated squamous cells with no cellular anaplasia
- Dense band of acute and chronic inflammatory cells surrounding epithelial pegs
- Malignant risk: In the perianal region, 30-56% are associated with an existing carcinoma; mortality ~20%
- Diagnosis: Excisional biopsy or multiple deep biopsies required to distinguish from true penile carcinoma
- Treatment:
- Complete surgical excision (optimal) - may require skin graft reconstruction in extensive cases
- Recurrence is common; close follow-up essential
- Podophyllin, 5-FU, and radiation therapy are ineffective (thickened stratum corneum impervious to topical agents)
- Systemic interferon + Nd:YAG laser: reported success in lower-volume disease
II. Non-Epithelial Benign Penile Tumours
These are mesenchymal and miscellaneous benign tumours. They are much less common than epithelial tumours.
| Tumour | Notes |
|---|---|
| Haemangioma | Vascular malformation/benign tumour; may bleed; usually on glans or prepuce |
| Lymphangioma | Lymphatic vessel tumour; rare |
| Neurofibroma | Nerve sheath tumour; may be part of NF-1 (von Recklinghausen disease) |
| Lipoma | Benign adipose tissue tumour; usually on penile shaft |
| Leiomyoma | Smooth muscle tumour arising from dartos or vascular smooth muscle |
| Fibroma | Rare; fibrous tissue origin |
All are treated by local excision.
III. Other Benign / Inflammatory Lesions Sometimes Grouped with Benign Tumours
Peyronie's Disease
- Hard penile plaques in the connective tissue between corpora cavernosa and tunica albuginea
- Results from collagen deposition secondary to microvascular trauma and organizing sclerosing chronic inflammation
- Not neoplastic - reactive
- Clinical: penile curvature toward the lesion + pain during intercourse
- Treatment: surgery or collagenase (Xiaflex) injection to lyse fibrous plaques
HPV Vaccination (Prevention)
- Gardasil (quadrivalent): Protects against HPV types 6, 11, 16, 18
- FDA approved for females (2006) and males (2010), ages 9-26 years
- Provides excellent protection against low-risk HPV (types 6 & 11) - prevents condylomata
- Also protects against high-risk HPV (16 & 18) - prevents PeIN and SCC
Summary
| Lesion | HPV type | Malignant risk | Key feature |
|---|---|---|---|
| Condyloma acuminatum | 6, 11 | Low (rare transformation) | Koilocytes; acetowhite |
| Buschke-Löwenstein | 6, 11 | High in perianal form (30-56% associated carcinoma) | Locally invasive, no metastasis |
| Haemangioma / Lipoma / Fibroma | None | None | Rare; excision curative |
| Peyronie's disease | None | None | Plaque, curvature; reactive |
Sources: Campbell-Walsh-Wein Urology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.