Acute rheumatic fever
Reading File
Finding Sources
Searching PubMed
"acute rheumatic fever"[MeSH Terms] AND ("diagnosis" OR "management")
Searching the Web
acute rheumatic fever 2024 2025 guidelines diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Searching Images
erythema marginatum acute rheumatic fever rash
I now have everything needed for a comprehensive answer. Let me compile it.
Acute Rheumatic Fever (ARF)
Overview
Acute rheumatic fever is a delayed, nonsuppurative, autoimmune complication of Group A streptococcal (GAS) pharyngitis, mediated by molecular mimicry between streptococcal antigens and human tissue proteins. It affects the heart, joints, skin, and CNS — and its cardinal long-term consequence is rheumatic heart disease (RHD), the leading cause of preventable cardiovascular death in low-income countries.
- Global prevalence: ~33 million cases; ~300,000 deaths/year
- Highest burden: Oceania, South Asia, sub-Saharan Africa
- Peak age: 5–15 years (equal sex incidence; RHD more common in women)
Pathogenesis
The driving mechanism is molecular mimicry — GAS pharyngeal infection triggers an immune response that cross-reacts with human tissues. Skin infections (impetigo) do not typically trigger ARF.
| Manifestation | Immune Mechanism |
|---|---|
| Carditis | Cross-reactive antibodies + CD4⁺ T-cell infiltration |
| Arthritis | Immune complex deposition in synovium |
| Chorea | Antibody binding to basal ganglia neuronal cells |
| Skin lesions | Delayed hypersensitivity reaction |
Pathologic hallmark: Aschoff Body
The Aschoff body (nodule) is a perivascular granuloma found in the myocardium — the pathognomonic lesion of rheumatic carditis. It consists of Anitschkow cells (activated macrophages with characteristic "caterpillar" nuclei) surrounded by lymphocytes and plasma cells.
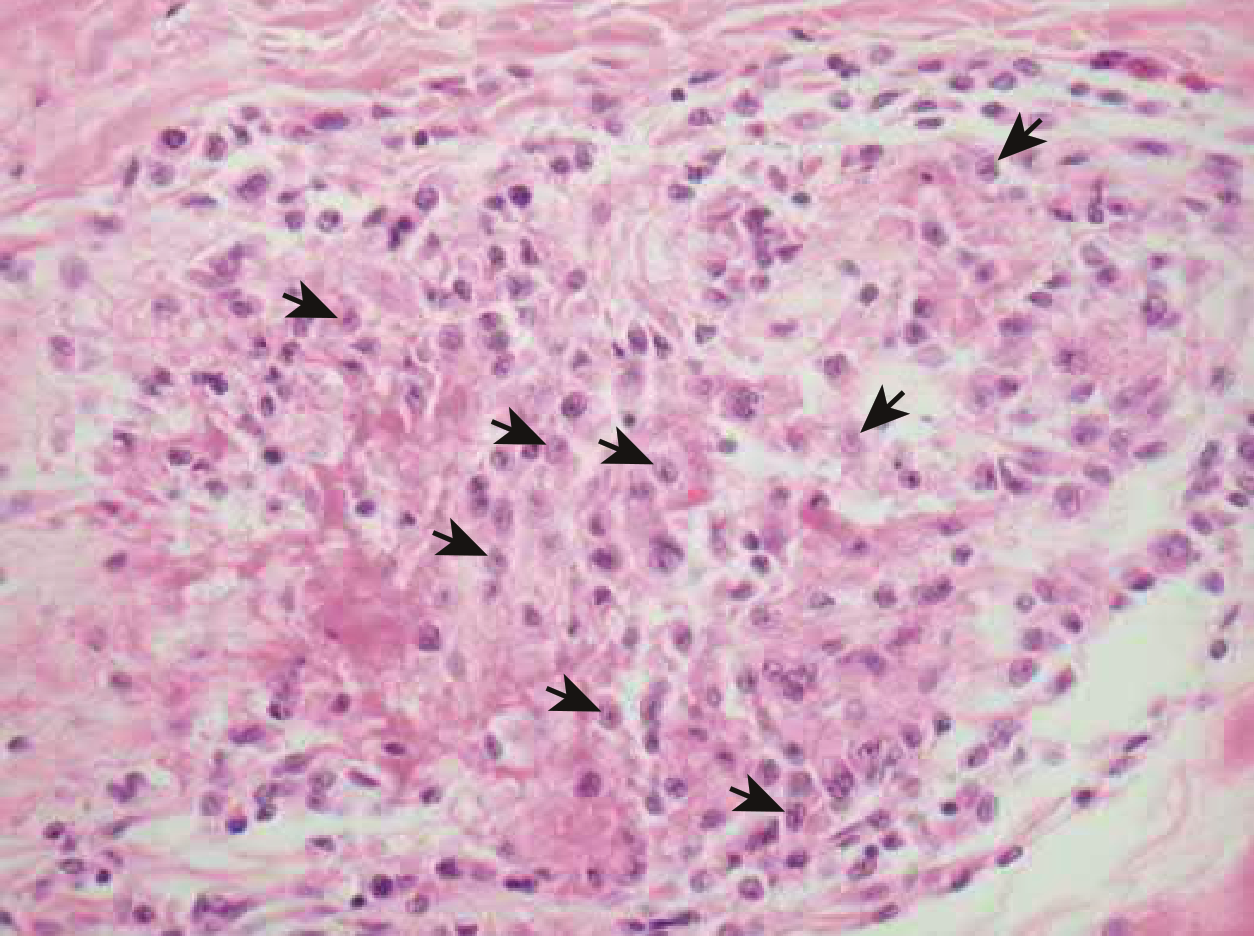
Photomicrograph of an Aschoff nodule from the heart in acute rheumatic fever (Braunwald's Heart Disease, Fig. 81.2). Arrows indicate Anitschkow cells.
Clinical Manifestations
ARF develops 2–4 weeks after GAS pharyngitis (latent period with no signs of active inflammation). Up to one-third of cases follow asymptomatic GAS infection.
Major Manifestations (Jones Criteria)
| Feature | Frequency | Key Details |
|---|---|---|
| Fever | >90% | ≥38.5°C |
| Migratory polyarthritis | 60–75% | Large joints (knees, ankles, elbows, wrists); sterile joint fluid, lymphocyte-predominant; exquisitely responsive to NSAIDs |
| Carditis (pancarditis) | >50% | Valvulitis most significant — mitral > aortic; presents as new murmur, cardiomegaly, CHF, or pericarditis; can be subclinical (Doppler-only) |
| Sydenham's chorea | ~30% | Involuntary, non-rhythmic, purposeless movements; unilateral predominance; stops during sleep; may present in isolation weeks after other symptoms resolve |
| Erythema marginatum | <10% | Pink, non-pruritic, blanching macules with serpiginous spreading margins on trunk/proximal limbs; migratory |
| Subcutaneous nodules | <10% | 0.5–2 cm, painless, over bony prominences/extensor tendons; resemble JIA nodules histologically |
Erythema Marginatum

Erythema marginatum: classic "smoke-ring" annular plaques with central clearing, serpiginous borders, on trunk/proximal limbs. A major Jones criterion.
Cardiac involvement
ARF is a pancarditis, affecting:
- Endocardium/valves (most important clinically) → mitral regurgitation ± aortic regurgitation
- Myocardium → Aschoff bodies, reduced contractility
- Pericardium → fibrinous pericarditis ± effusion (only with endocardial involvement; usually no permanent damage)
Diagnosis: 2015 Revised Jones Criteria (AHA)
No definitive test exists. Diagnosis requires evidence of antecedent GAS infection PLUS fulfillment of Jones criteria.
Criteria differ by population risk
Initial ARF: 2 major OR 1 major + 2 minor criteria
Recurrent ARF: 2 major, OR 1 major + 2 minor, OR 3 minor criteria
Recurrent ARF: 2 major, OR 1 major + 2 minor, OR 3 minor criteria
| Criteria | Low-Risk Populations (ARF <2/100,000 school-age children/year) | Moderate/High-Risk Populations |
|---|---|---|
| Major — Carditis | Clinical ± subclinical (echo) valvulitis | Same |
| Major — Arthritis | Polyarticular only | Monoarticular OR polyarticular |
| Major — Chorea | ✓ | ✓ |
| Major — Erythema marginatum | ✓ | ✓ |
| Major — Subcutaneous nodules | ✓ | ✓ |
| Minor — Arthralgia | Polyarthralgia | Monoarthralgia |
| Minor — Fever | ≥38.5°C | ≥38.5°C |
| Minor — Acute phase reactants | ESR ≥60 mm/hr AND/OR CRP ≥3.0 mg/dL | ESR ≥30 mm/hr AND/OR CRP ≥3.0 mg/dL |
| Minor — ECG | Prolonged PR interval | Prolonged PR interval |
Key rule: Arthralgia cannot be a minor criterion if arthritis is already counted as a major criterion. Similarly, prolonged PR cannot be minor if carditis is major.
Evidence of GAS infection
- Positive throat culture for GAS
- Positive rapid GAS antigen test
- Elevated/rising antistreptolysin O (ASO) titer
- Elevated anti-DNase B titer
- History of scarlet fever
Investigations
- Always: ECG, echocardiogram, CBC, CRP/ESR, ASO + anti-DNase B
- As indicated: throat/skin swab, blood cultures, synovial fluid aspirate, pregnancy test, renal function (if NSAIDs planned), autoantibodies (to exclude alternatives)
Treatment
1. Antibiotics (eradicate GAS)
All patients, regardless of culture results:
- Benzathine penicillin G 1.2 MU IM (single dose; 600,000 U if <27 kg) — preferred
- OR Phenoxymethylpenicillin 500 mg PO BD × 10 days (250 mg if ≤27 kg)
- OR Amoxicillin 50 mg/kg (max 1 g) daily × 10 days
- Penicillin allergy: erythromycin or azithromycin
2. Anti-inflammatory therapy
| Indication | Drug | Dose |
|---|---|---|
| Arthritis/arthralgia/fever | Aspirin (first-line traditional) | 50–100 mg/kg/day in 4–5 divided doses (max 4–8 g/d adults) |
| Same (preferred by many) | Naproxen | 10–20 mg/kg/day BD (safer profile) |
| Severe carditis with CHF | Prednisone/prednisolone | 1–2 mg/kg/day (max 80 mg) × up to 3 weeks |
NSAIDs are not proven to prevent or reduce the severity of RHD. They are purely symptomatic. The benefit of corticosteroids over salicylates for carditis is not established by older RCTs, though some newer data suggest short-term echocardiographic improvement.
3. Chorea
- Mild: calm environment, reassurance
- Severe: carbamazepine or sodium valproate (preferred over haloperidol)
- Consider corticosteroids in severe/refractory chorea (prednisone 0.5 mg/kg/day)
- IVIg: may reduce chorea duration in small studies; not standard
4. Heart failure
- Standard CHF management
- Bed rest while symptomatic; gradual mobilization once controlled
Secondary Prophylaxis
The most critical intervention — prevents recurrent GAS pharyngitis and cumulative valvular damage.
Drug of choice: Benzathine penicillin G 1.2 MU IM every 4 weeks
(every 3 weeks in high-risk settings or if breakthrough infections occur)
(every 3 weeks in high-risk settings or if breakthrough infections occur)
Alternatives (less effective): Oral penicillin V 250 mg BD, or oral macrolide (e.g., azithromycin 250 mg daily)
Duration (Harrison's 22E, AHA guidelines)
| Patient Category | Duration |
|---|---|
| ARF without carditis | 5 years after last attack OR until age 21 (whichever is longer) |
| ARF with carditis, no residual valve disease | 10 years after last attack OR until age 21 (whichever is longer) |
| ARF with persistent valvular disease | 10 years after last attack OR until age 40 (whichever is longer); sometimes lifelong |
Prognosis
- The acute episode resolves in 2–4 weeks in most patients
- Carditis at the initial attack is the strongest predictor of RHD
- Recurrent ARF causes cumulative valvular damage — hence the critical importance of secondary prophylaxis
- Arthritis and chorea resolve completely without residual damage
- Subclinical carditis on echocardiography carries prognostic significance even without clinical signs
Prevention
| Level | Strategy |
|---|---|
| Primary | Prompt diagnosis and 10-day antibiotic treatment of GAS pharyngitis |
| Primordial | Reduce household crowding, improve hygiene, sanitation, nutrition |
| Secondary | Long-term BPG prophylaxis post-ARF |
A GAS vaccine is under active development but not yet available.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Braunwald's Heart Disease 12E; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart 15E. 2015 AHA Jones Criteria revision: Gewitz MH et al, Circulation 131:1806.
This is a shared conversation. Sign in to Orris to start your own chat.