What is headache?
Reading File
Finding Sources
Searching PubMed
headache classification diagnosis
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a comprehensive overview of headache based on authoritative medical textbooks.
Headache
Definition
A headache is pain referred to the surface of the head from deep head structures. The source may be intracranial (inside the skull) or extracranial (outside the skull, e.g., nasal sinuses, muscles, or eyes). Importantly, brain tissue itself is almost entirely insensitive to pain — the headache arises from pain-sensitive structures around the brain, not the brain parenchyma itself.
— Guyton and Hall Textbook of Medical Physiology
Pain-Sensitive Structures Inside the Skull
The brain cortex, when stimulated, does not produce pain. The following structures are genuinely pain-sensitive:
- Venous sinuses and surrounding dura
- Meninges (especially at the base of the brain)
- Meningeal and cerebral blood vessels (especially the middle meningeal artery)
- The tentorium cerebelli when stretched or damaged
Intracranial Causes of Headache
| Type | Mechanism |
|---|---|
| Meningitis | Inflammation of meninges causes the most severe headaches; pain is referred over the entire head |
| Low CSF pressure | Removing even ~20 mL of CSF reduces buoyancy of the brain, stretching dural surfaces |
| Migraine | Activation of the trigeminovascular system releases CGRP, substance P, and nitric oxide → vasodilation + neurogenic inflammation |
| Alcoholic headache | Direct meningeal irritation by alcohol; dehydration contributes |
Referred Pain Patterns (Intracranial)
- Above the tentorium → pain conducted via CN V (trigeminal) → referred to the front half of the head
- Below the tentorium → pain via glossopharyngeal, vagal, and C2 nerves → referred to the occiput and posterior head
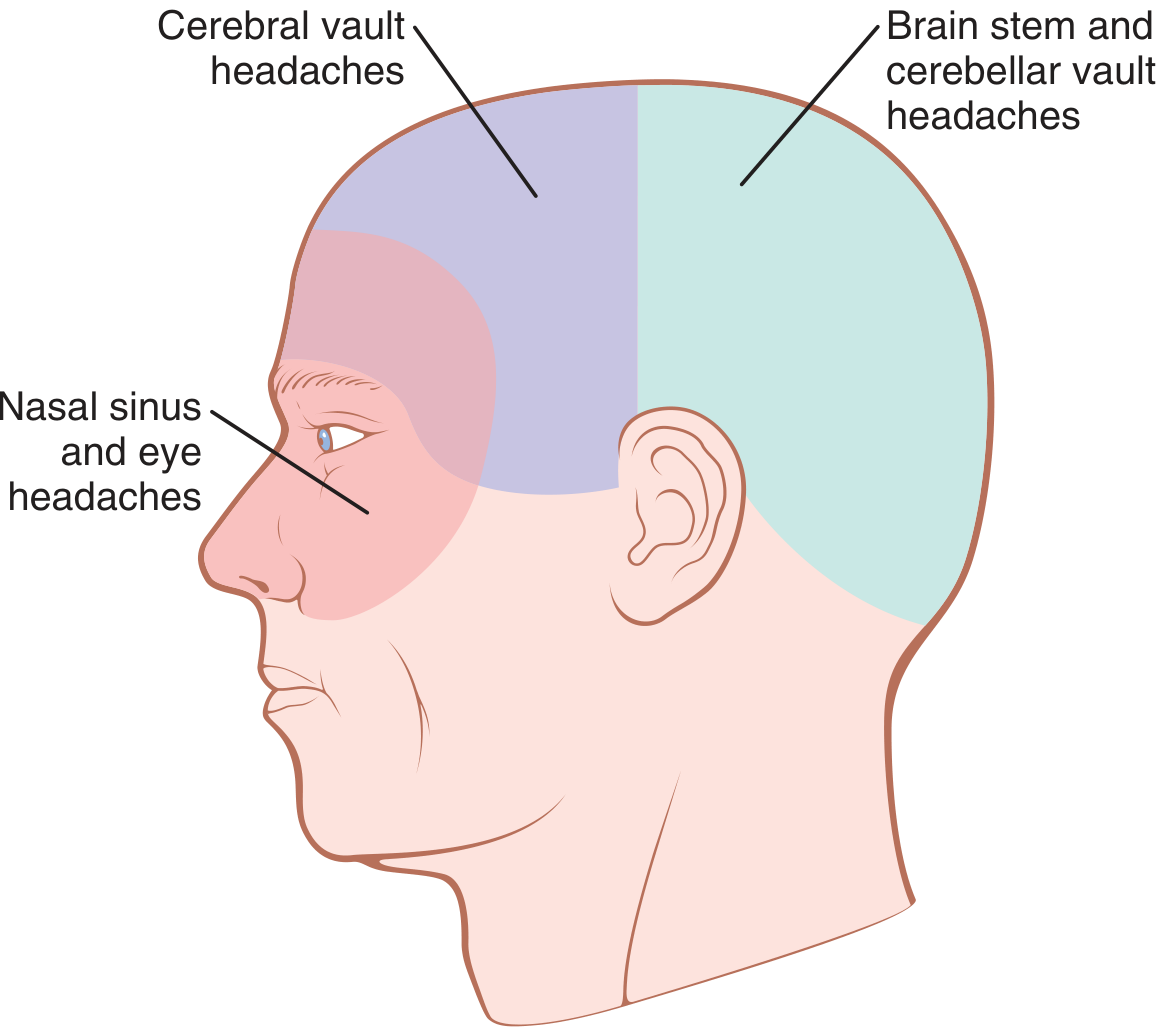
Extracranial Causes of Headache
- Tension-type / muscle spasm: Emotional tension causes scalp and occipital neck muscles to become spastic, referring pain across the scalp. This is the most common type of headache.
- Nasal sinus irritation/infection: Sinus mucosa pain is referred behind the eyes (ethmoid/sphenoid), to the forehead (frontal sinuses), or the face (maxillary sinuses).
- Eye disorders: Excessive ciliary muscle contraction (refractive errors) or UV light exposure → retro-orbital headache.
Migraine — Key Details
- Prevalence: ~15% of the population; ~3× more common in women
- Duration: 4–72 hours per episode; moderate to severe intensity
- Prodrome/Aura: Nausea, visual disturbances, or sensory hallucinations 30–60 minutes before pain onset, driven by cortical spreading depression
- Mechanism: Trigeminovascular activation → CGRP + substance P release → intracranial vasodilation + local inflammation → pain signals relayed to somatosensory cortex
- Genetics: Positive family history in 65–90% of cases
Red Flag Features Requiring Urgent Imaging (MRI)
According to Bradley and Daroff's Neurology in Clinical Practice, the following warrant immediate investigation:
- Thunderclap headache (new-onset severe headache, possible aneurysm rupture)
- Progressive increase in frequency or severity
- "Worst headache of my life"
- Headache always localized to one side
- Unresponsive to treatment
- Headache in a cancer patient
- Associated fever, altered mental status, or focal neurological deficit
MRI (with gadolinium if non-enhanced study is negative) is the imaging modality of choice.
Summary of Types
| Category | Examples |
|---|---|
| Primary headaches | Tension-type, migraine, cluster headache |
| Secondary headaches | Meningitis, SAH (subarachnoid hemorrhage), raised ICP, sinusitis, hypertension, eye disorders |
Sources: Guyton and Hall Textbook of Medical Physiology; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.