Emphysema for university exam for 2 proff patho for abvmu university from harsh mohna book
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
I have sufficient material now to write a comprehensive exam-oriented answer. Note that Harsh Mohan's textbook is not in the library, but the content from Robbins Basic Pathology and Robbins Cotran Pathologic Basis of Disease - which are the standard international pathology references and very closely aligned with Harsh Mohan's content - covers all the exam topics.
Emphysema - Complete Notes for ABVMU 2nd Prof Pathology Exam
(Based on standard pathology - aligned with Harsh Mohan's Textbook of Pathology)
DEFINITION
Emphysema is defined as permanent, irreversible enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of the alveolar walls, WITHOUT significant fibrosis.
- It is an anatomical diagnosis (unlike chronic bronchitis, which is a clinical diagnosis).
- It is classified by its anatomic distribution within the lobule/acinus.
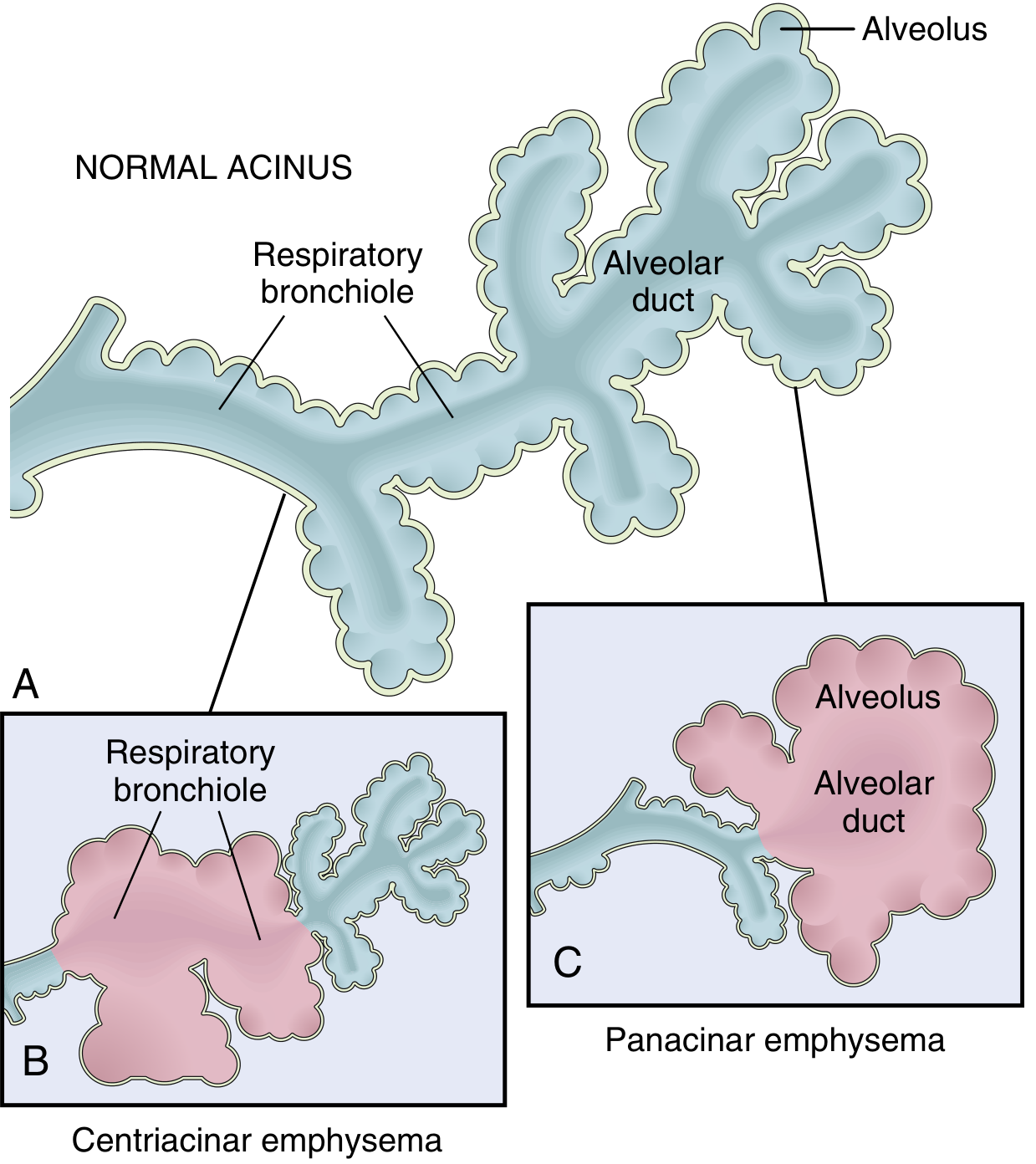
Remember: The acinus = structure distal to terminal bronchiole (respiratory bronchioles + alveolar ducts + alveoli). A cluster of 3-5 acini = lobule.
CLASSIFICATION / TYPES
There are 4 major morphological types:
1. Centriacinar (Centrilobular) Emphysema - Most Common
- Most common type - >95% of clinically significant cases
- Central/proximal parts of the acinus (respiratory bronchioles) are affected; distal alveoli are spared
- Both normal and emphysematous spaces coexist within the same acinus
- Predominantly affects upper lobes, apical segments
- Strongly associated with cigarette smoking
- Most common form of COPD-related emphysema
2. Panacinar (Panlobular) Emphysema
- Uniform enlargement of the entire acinus - from respiratory bronchiole to terminal alveoli
- Predominantly affects lower lung zones and anterior margins
- Associated with α1-antitrypsin (AAT) deficiency
- Occurs earlier and more severely in smokers with AAT deficiency
3. Distal Acinar (Paraseptal) Emphysema
- Proximal part of acinus is spared; distal part is predominantly involved
- Located near the pleura, lobular septa, and margins adjacent to fibrosis/scarring
- More severe in the upper half of lungs
- Enlarged air spaces 0.5 mm - >2 cm, can form bullae
- Commonly presents as spontaneous pneumothorax in young adults
- Cause is unknown
4. Irregular (Paracicatricial) Emphysema
- Acinus is irregularly involved, almost always associated with scarring
- Usually occurs as small foci and is clinically insignificant
PATHOGENESIS
The central mechanism is the protease-antiprotease imbalance + oxidant-antioxidant imbalance.
Step-by-step Mechanism:
1. Toxic Injury and Inflammation
- Cigarette smoke + noxious particles damage respiratory epithelium
- Triggers inflammation - releases mediators: LTB4, IL-8, TNF
- Macrophages and epithelial cells recruit neutrophils into the lung
2. Protease-Antiprotease Imbalance (Key Mechanism)
- Neutrophils and macrophages release elastases and other proteases
- These break down elastin and other connective tissue components
- Normally, α1-antitrypsin (α1-AT) inhibits elastase
- When α1-AT is deficient (genetic - Z allele on chromosome 14, Pi locus) OR overwhelmed by smoking, elastin destruction proceeds unchecked
- Loss of elastic tissue → loss of radial traction → airway collapse on expiration → functional airflow obstruction
3. Oxidative Stress
- Tobacco smoke + inflammatory cells generate oxidants (reactive oxygen species)
- Oxidants cause tissue damage, endothelial dysfunction, amplify inflammation
- NRF2 (encoded by NFE2L2) is a protective transcription factor - inactivation increases susceptibility to smoke damage
4. Infection
- Does NOT initiate emphysema
- But may maintain and acutely exacerbate existing disease
α1-Antitrypsin Deficiency - Important Detail:
- Encoded by Pi locus on chromosome 14
- ~0.01% of US population homozygous for Z allele → markedly decreased serum AAT
-
80% of ZZ individuals develop symptomatic panacinar emphysema
- Worsened significantly by smoking
- About 1% of all emphysema patients have this defect
MORPHOLOGY
Gross Appearance:
- Panacinar emphysema: Pale, voluminous lungs, often overlap the heart anteriorly, diaphragm is flattened
- Centriacinar emphysema: Less impressive grossly; deeper pink, less voluminous; upper 2/3 more severely affected
- Large alveoli visible on cut surface
- Apical blebs or bullae in advanced disease (bullae = spaces >1 cm)
Microscopic Appearance:
- Abnormally large alveolar spaces separated by thin septa
- Destruction of alveolar walls WITHOUT fibrosis (key distinguishing feature)
- Focal centriacinar fibrosis
- Loss of attachments between alveoli and outer wall of small airways
- Pores of Kohn are so enlarged that septa appear to float / protrude blindly into spaces (club-shaped ends)
- Decrease in capillary bed (due to alveolar wall loss)
- Inflammatory changes in small airways (bronchiolar inflammation + submucosal fibrosis) in advanced disease

CLINICAL FEATURES
| Feature | Emphysema ("Pink Puffer") |
|---|---|
| Onset | Insidious, dyspnea on exertion |
| Build | Thin, cachexic |
| Cough | Mild, often absent |
| Sputum | Scanty |
| Dyspnea | Severe, prominent early |
| Cyanosis | Absent (hence "pink") |
| Barrel chest | Present (increased AP diameter) |
| Breath sounds | Diminished |
| Percussion | Hyperresonant |
| Pursed lip breathing | Characteristic |
| Accessory muscles | Used during breathing |
| Cor pulmonale | Late complication |
Pulmonary Function Tests (PFT):
- FEV1/FVC ratio decreased (obstructive pattern)
- Total Lung Capacity (TLC) increased (air trapping)
- Residual Volume (RV) increased
- Diffusing capacity (DLCO) decreased (loss of alveolar surface area)
Complications:
- Pulmonary hypertension → Cor pulmonale (right heart failure)
- Respiratory failure (superimposed infection)
- Spontaneous pneumothorax (rupture of bullae - especially in paraseptal type)
- Secondary polycythemia (chronic hypoxemia)
- Death from respiratory failure or right heart failure
OTHER FORMS OF EMPHYSEMA (Harsh Mohan classifies these separately)
| Type | Description |
|---|---|
| Compensatory hyperinflation | Dilation of remaining alveoli after lung resection/lobe removal - NOT true emphysema |
| Obstructive overinflation | Air trapping due to ball-valve obstruction (tumor, foreign body, congenital lobar) - can be life-threatening |
| Bullous emphysema | Large subpleural blebs/bullae (>1 cm) in any form; rupture → pneumothorax |
| Interstitial emphysema | Air enters connective tissue/mediastinum/subcutaneous tissue (via alveolar tears during coughing or chest wounds) |
COMPARISON: PINK PUFFER vs BLUE BLOATER (Important Exam Table)
| Feature | Emphysema (Pink Puffer) | Chronic Bronchitis (Blue Bloater) |
|---|---|---|
| Definition | Anatomical | Clinical |
| Build | Thin | Obese |
| Cough | Mild/absent | Productive cough |
| Cyanosis | Absent | Present |
| Dyspnea | Severe | Mild early |
| Cor pulmonale | Late | Early |
| Hypoxia | Mild | Severe |
| DLCO | Decreased | Normal/near normal |
SUMMARY - HIGH-YIELD EXAM POINTS
- Definition: Permanent enlargement of air spaces DISTAL to terminal bronchioles + wall destruction WITHOUT fibrosis
- Most common type: Centriacinar (upper lobes, smoking)
- Alpha-1 antitrypsin deficiency → Panacinar emphysema (lower lobes)
- Spontaneous pneumothorax in young adults → Paraseptal (distal acinar) emphysema
- Pathogenesis: Protease-antiprotease imbalance (neutrophil elastase vs α1-AT)
- Pi locus, chromosome 14 - ZZ genotype = severe AAT deficiency
- Morphology: Voluminous pale lungs, destroyed alveolar walls, NO fibrosis
- Pink puffer = thin, pursed lips, severe dyspnea, no cyanosis
- DLCO decreased (distinguishes from simple asthma)
- Bullae rupture → Pneumothorax
Note: Harsh Mohan's Textbook of Pathology is not available in the digital library, but the above content is sourced from Robbins Basic Pathology and Robbins & Cotran Pathologic Basis of Disease - both are the international standard references that Harsh Mohan's book is based upon, and the content is essentially identical for university exam purposes.
This is a shared conversation. Sign in to Orris to start your own chat.