Teach me ECG from 0
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG normal waveform P QRS T wave labeled diagram
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Searching Images
12-lead ECG electrode placement chest leads precordial
Searching Images
ECG heart rate calculation rhythm axis hypertrophy ischemia systematic approach
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Searching Images
ECG axis deviation hexaxial reference system leads I aVF
Loading Image
Searching Images
STEMI ST elevation myocardial infarction ECG changes leads
Loading Image
Searching Images
atrial fibrillation flutter heart block arrhythmia ECG strip
Loading Image
Loading Image
I now have comprehensive material to deliver a full ECG course from zero. Let me compile it all.
ECG from Zero — Complete Beginner's Guide
1. What Is an ECG?
An electrocardiogram (ECG/EKG) is a graphic recording of the heart's electrical activity over time. Each heartbeat is triggered by an electrical impulse that spreads through the heart in a predictable sequence. The ECG captures this as a waveform on paper (or screen), allowing you to assess rhythm, rate, conduction, and myocardial health.
The ECG does not measure mechanical contraction — it measures electrical events. But because electricity drives contraction, the two are tightly coupled.
2. The Cardiac Conduction System
Understanding what you're recording is essential before reading the paper.
SA Node (sinoatrial node)
↓ fires spontaneously ~60-100/min — the natural pacemaker
Atria depolarize → produce P wave
↓
AV Node (atrioventricular node) — DELAY (~0.12s) — protects ventricles
↓
Bundle of His
↓
Right bundle branch → Right ventricle
Left bundle branch (splits into anterior & posterior fascicles) → Left ventricle
↓
Purkinje fibers → Myocardium depolarizes → QRS complex
↓
Ventricles repolarize → T wave
Key principle: Normal conduction goes top → bottom, right → left. Any deviation from this path widens or distorts the QRS.
3. The ECG Waveform — Every Component Explained
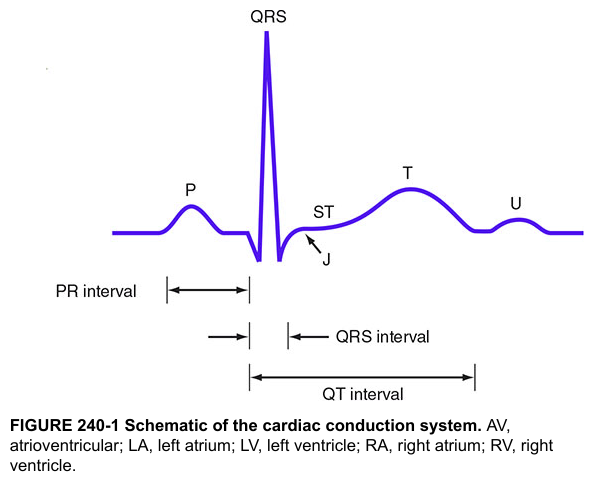
| Wave/Segment | What it represents | Normal duration |
|---|---|---|
| P wave | Atrial depolarization (SA node → atria) | < 120 ms, < 2.5 mm tall |
| PR interval | Time from atrial activation to ventricular activation (includes AV node delay) | 120–200 ms (3–5 small boxes) |
| QRS complex | Ventricular depolarization | < 120 ms (< 3 small boxes) |
| ST segment | Early ventricular repolarization — should be isoelectric | Flat (±1 mm) |
| J point | Junction of QRS and ST segment | |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | Total ventricular activity (depolarization + repolarization) | < 440 ms in men, < 460 ms in women |
| U wave | Thought to represent Purkinje fiber repolarization | Small, follows T wave |
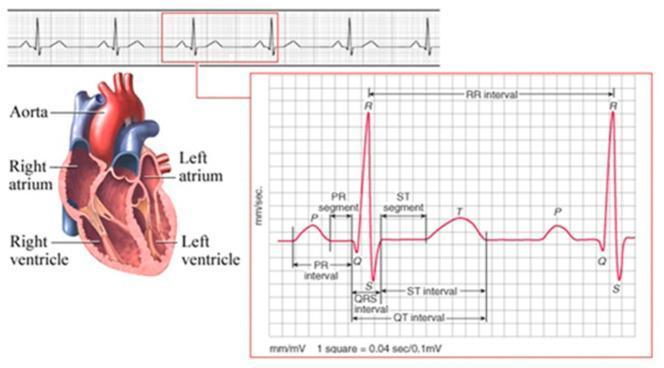
The ECG Grid
- 1 small box = 0.04 seconds (time) and 0.1 mV (voltage)
- 1 large box = 0.20 seconds (5 small boxes)
- Paper runs at 25 mm/second (standard)
4. The 12 Leads — The Heart's 12 Viewpoints
A standard ECG has 12 leads — each is a different "camera angle" on the heart's electrical activity. More leads = more information for localizing pathology.
Electrode Placement
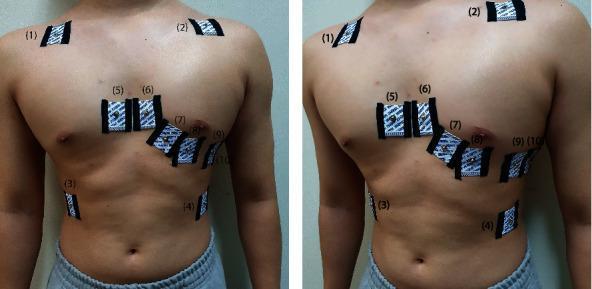
4 limb electrodes generate 6 frontal leads:
- Bipolar: Lead I (RA–LA), Lead II (RA–LL), Lead III (LA–LL)
- Augmented unipolar: aVR (right arm), aVL (left arm), aVF (left foot)
6 chest (precordial) electrodes generate 6 horizontal leads (V1–V6):
| Lead | Position |
|---|---|
| V1 | 4th ICS, right sternal border |
| V2 | 4th ICS, left sternal border |
| V3 | Between V2 and V4 |
| V4 | 5th ICS, mid-clavicular line |
| V5 | Anterior axillary line (same horizontal as V4) |
| V6 | Mid-axillary line (same horizontal as V4) |
What Each Group "Sees"
| Leads | View of the heart | Artery at risk |
|---|---|---|
| II, III, aVF | Inferior wall | RCA |
| I, aVL, V5, V6 | Lateral wall | LCx |
| V1–V4 | Anterior/septal wall | LAD |
| aVR | Cavity/right atrium, "global" | — |
5. The Electrical Axis
The mean QRS axis is the average direction of ventricular depolarization in the frontal plane. It's assessed using the hexaxial reference system.
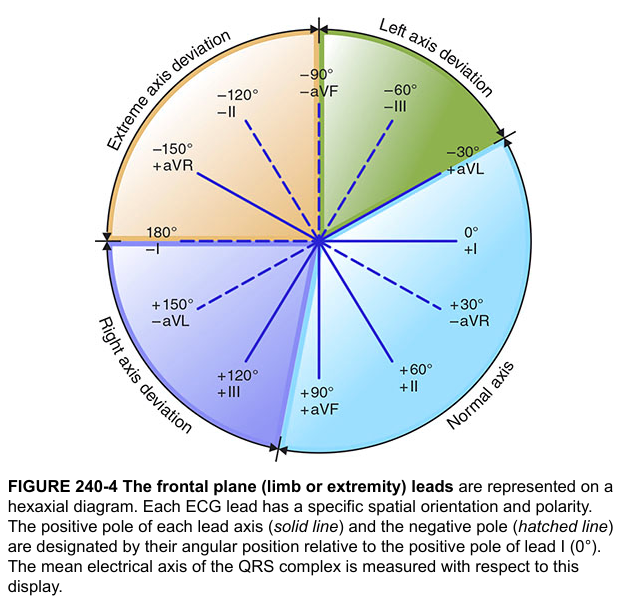
Quick axis determination (Lead I + aVF method):
| Lead I | aVF | Axis |
|---|---|---|
| + (upright) | + (upright) | Normal (0° to +90°) |
| + (upright) | − (negative) | Left axis deviation (LAD) |
| − (negative) | + (upright) | Right axis deviation (RAD) |
| − (negative) | − (negative) | Extreme axis deviation ("northwest") |
Causes of LAD: LBBB, left anterior fascicular block, inferior MI, LVH
Causes of RAD: RVH, RBBB, left posterior fascicular block, lateral MI, pulmonary embolism
Causes of RAD: RVH, RBBB, left posterior fascicular block, lateral MI, pulmonary embolism
6. The Systematic Approach to Reading an ECG
Never read an ECG randomly. Always follow the same order:
Step 1 — Rate
Rule of 300: Divide 300 by the number of large boxes between two R waves.
- 1 large box = 300 bpm
- 2 large boxes = 150 bpm
- 3 large boxes = 100 bpm
- 4 large boxes = 75 bpm
- 5 large boxes = 60 bpm
For irregular rhythms, count QRS complexes in a 10-second strip × 6.
Step 2 — Rhythm
Ask:
- Is it regular or irregular?
- Is there a P wave before every QRS?
- Is the P wave normal (upright in II, inverted in aVR)?
- Is the PR interval constant?
Step 3 — Axis (as above)
Step 4 — P Wave
- Present? Normal shape (< 120 ms, < 2.5 mm)?
- Notched P in II → P mitrale (left atrial enlargement)
- Peaked P in II > 2.5 mm → P pulmonale (right atrial enlargement)
Step 5 — PR Interval
- Short (< 120 ms) → accessory pathway (e.g., WPW), junctional rhythm
- Long (> 200 ms) → 1st degree AV block
Step 6 — QRS Complex
- Narrow (< 120 ms) = normal ventricular conduction
- Wide (> 120 ms) = bundle branch block, pacing, hyperkalemia, accessory pathway
- Q waves (pathological if > 40 ms wide or > 25% of QRS height) → prior infarction
Step 7 — ST Segment
- Elevation (> 1 mm in limb leads, > 2 mm in precordial leads) → STEMI, pericarditis, Brugada, early repolarization
- Depression (> 1 mm) → ischemia, NSTEMI, digitalis effect, LVH strain
Step 8 — T Wave
- Flat or inverted → ischemia, LVH, RBBB, hypokalemia, PE
- Peaked/hyperacute → hyperkalemia, early STEMI ("tombstoning" precursor)
Step 9 — QT Interval
- Corrected QT (QTc) = QT ÷ √(RR interval in seconds) — Bazett's formula
- Prolonged QTc > 440 ms (men) / 460 ms (women) → risk of Torsades de Pointes
- Causes: drugs (antiarrhythmics, antipsychotics, fluoroquinolones), hypokalemia, hypomagnesemia, hypocalcemia, congenital long QT syndrome
7. Common Arrhythmias
Sinus Tachycardia
- Rate > 100 bpm, normal P waves, regular, normal PR
- Causes: fever, pain, anxiety, dehydration, PE, thyrotoxicosis
Sinus Bradycardia
- Rate < 60 bpm, normal P waves, regular
- Causes: athletes, hypothyroidism, inferior MI, beta-blockers, increased vagal tone
Atrial Fibrillation (AFib)
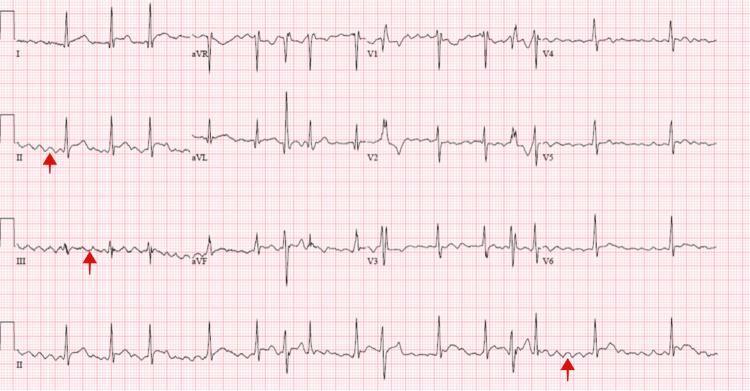
- Irregularly irregular rhythm
- No P waves — replaced by chaotic fibrillatory baseline
- Narrow QRS (unless aberrant conduction)
- Rate typically 100–160 bpm (uncontrolled)
AV Blocks
| Type | ECG Finding | Clinical significance |
|---|---|---|
| 1st degree | PR > 200 ms, every P conducts | Benign, monitor |
| 2nd degree Mobitz I (Wenckebach) | PR progressively lengthens until a P fails to conduct (dropped QRS) | Usually benign; can occur with inferior MI |
| 2nd degree Mobitz II | Constant PR, then sudden non-conducted P wave | More serious; can progress to 3rd degree |
| 3rd degree (complete) | P waves and QRS are completely independent (AV dissociation) | Emergency — pacemaker needed |
8. Bundle Branch Blocks
When the right or left bundle branch is blocked, the ventricle it supplies depolarizes late (via slow cell-to-cell spread), widening the QRS > 120 ms.
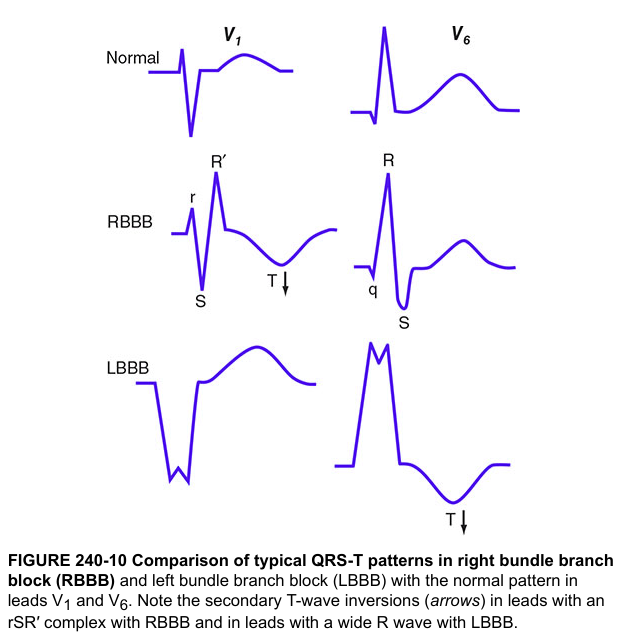
Right Bundle Branch Block (RBBB)
- QRS > 120 ms
- rSR' ("M shape") in V1 — classic rabbit ear pattern
- Wide S wave in I, V5, V6
- Secondary T-wave inversion in V1–V3
- Causes: PE, RVH, congenital (ASD), ischemia, or normal variant
Left Bundle Branch Block (LBBB)
- QRS > 120 ms
- Broad, notched R wave in I, V5, V6 ("M" in lateral leads)
- Deep S wave / QS in V1
- No septal Q waves in I, V6
- Secondary T-wave inversion in V5–V6
- Causes: always pathological — LVH, dilated cardiomyopathy, LAD disease, hypertension
Mnemonic: MaRRoW (M shape in V1 = RBBB, W shape in V1 = LBBB) / WiLLiaM MoRRoW
9. Ischemia and Infarction
This is the most critical clinical application of ECG.
Evolution of STEMI
- Hyperacute T waves (earliest, minutes) — tall, peaked, broad
- ST elevation (hours) — convex upward ("tombstone")
- T wave inversion (hours–days)
- Q waves (irreversible necrosis, days–weeks) — > 40 ms wide, > 25% of R height

Localization of MI by Lead Group
| Location | ST elevation leads | Reciprocal depression | Artery |
|---|---|---|---|
| Anterior | V1–V4 | II, III, aVF | LAD (proximal) |
| Inferior | II, III, aVF | I, aVL | RCA (usually) |
| Lateral | I, aVL, V5–V6 | II, III, aVF | LCx |
| Posterior | V1–V2 depression (tall R) | ST elevation in V7–V9 | RCA or LCx |
STEMI Criteria (ESC 2023)
- ≥ 2 mm ST elevation in ≥ 2 contiguous precordial leads
- ≥ 1 mm ST elevation in ≥ 2 contiguous limb leads
- New LBBB with symptoms = STEMI equivalent until proven otherwise
10. Ventricular Hypertrophy
Left Ventricular Hypertrophy (LVH)
Sokolow-Lyon criterion: S in V1 + R in V5 or V6 > 35 mm
Cornell criterion: R in aVL > 11 mm
Plus: ST depression and T-wave inversion in lateral leads ("LV strain pattern")
Cornell criterion: R in aVL > 11 mm
Plus: ST depression and T-wave inversion in lateral leads ("LV strain pattern")
Right Ventricular Hypertrophy (RVH)
- Right axis deviation
- Tall R in V1 (R > S)
- Deep S in V5–V6
- ST/T changes in V1–V3
- Causes: pulmonary hypertension, mitral stenosis, cor pulmonale, congenital heart disease
11. Electrolyte Abnormalities on ECG
| Electrolyte | Change | ECG findings |
|---|---|---|
| Hyperkalemia | ↑ K⁺ | Peaked T waves (early) → PR prolongation → wide QRS → sine wave → VF |
| Hypokalemia | ↓ K⁺ | Flat T waves, prominent U waves, QT prolongation |
| Hypercalcemia | ↑ Ca²⁺ | Short QT interval |
| Hypocalcemia | ↓ Ca²⁺ | Long QT interval |
12. Putting It All Together — The 9-Step Checklist
Every ECG you read, run through this checklist:
1. RATE → Tachycardia? Bradycardia? Normal (60–100)?
2. RHYTHM → Regular? Irregular? P before every QRS?
3. AXIS → Lead I & aVF method
4. P WAVES → Present, normal shape, one per QRS?
5. PR INTERVAL → 120–200 ms? Constant?
6. QRS → < 120 ms? Pathological Q waves?
7. ST SEGMENT → Elevation? Depression?
8. T WAVES → Peaked? Inverted? Flat?
9. QT INTERVAL → Correct for rate, < 440/460 ms?
Summary of Normal Values
| Parameter | Normal |
|---|---|
| Heart rate | 60–100 bpm |
| P wave duration | < 120 ms |
| PR interval | 120–200 ms |
| QRS duration | < 120 ms |
| QTc | < 440 ms (♂), < 460 ms (♀) |
| QRS axis | −30° to +90° |
Sources
- Harrison's Principles of Internal Medicine, 22nd Ed. — Figures 240-1, 240-4, 240-10
- Tintinalli's Emergency Medicine — ECG interpretation chapter
- Miller's Anesthesia, 10th Ed. — Electrical events and the ECG
This is a shared conversation. Sign in to Orris to start your own chat.