Mechanism of acceleration and deceleration injuries in brain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a detailed, textbook-grounded explanation of the mechanisms of acceleration and deceleration injuries in the brain.
Acceleration and Deceleration Injuries of the Brain
1. Fundamental Physics - Why the Brain Gets Injured
The brain and CSF have nearly identical specific gravity (within ~4% of each other), so under normal circumstances the brain "floats" in CSF and moves with the skull in unison. However, when forces are extreme, sudden, or applied without direct contact, a critical mismatch occurs between skull movement and brain movement due to inertia.
When linear and/or rotational forces are applied to the head, inertia causes the brain's movement to lag relative to that of the skull. The bony protuberances of the skull and the rigid fibrous dura (falx cerebri, tentorium cerebri) then deform and damage brain parenchyma. (Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
2. Coup and Contrecoup Injury
This is the classic pattern of acceleration-deceleration brain injury.
Coup Injury
A contusion at the site of impact. When the skull is struck, the CSF - being incompressible - pushes the brain in unison with the skull so the brain moves with the skull. The region directly under the impact is called the coup lesion.
Contrecoup Injury
The more counter-intuitive injury - occurring on the side opposite to the blow:
- When the skull is suddenly set in motion by a blow, it pulls away from the brain momentarily on the opposite side (due to the brain's inertia)
- This creates a transient vacuum space in the cranial vault opposite to the blow
- When the skull stops accelerating, this vacuum collapses and the brain strikes the inner surface of the skull on the opposite side
- This is the contrecoup contusion
"When a blow to the head is extremely severe, the sudden movement of the whole skull causes the skull to pull away from the brain momentarily because of the brain's inertia, creating for a split second a vacuum space in the cranial vault in the area opposite to the blow. Then, when the skull is no longer being accelerated by the blow, the vacuum suddenly collapses and the brain strikes the inner surface of the skull."
- Guyton and Hall Textbook of Medical Physiology
Without Physical Impact
Coup and contrecoup injuries can also be caused by rapid acceleration or deceleration alone in the absence of physical impact - the brain may bounce off the wall of the skull (coup injury) and then off the opposite side (contrecoup). Classic examples:
- Shaken baby syndrome
- High-speed vehicular accidents
Predilection Sites
The poles and inferior surfaces of the frontal and temporal lobes are most commonly injured, because these areas contact bony protuberances at the skull base. This explains why:
- A blow to the occiput causes contrecoup frontal/temporal injury
- Direct frontal impact causes frontal lobe injury with contrecoup occipital injury
- Traumatic hemorrhages are often multiple because both coup and contrecoup injuries occur simultaneously (Bradley and Daroff's Neurology in Clinical Practice)
3. Diffuse Axonal Injury (DAI)
DAI is a distinct and particularly devastating form of acceleration-deceleration injury, characterized by white matter disruption rather than focal contusion.
Mechanism
DAI results from rotational and tensile-shearing forces applied to the brain:
- Shearing, stretching, and angular forces pull on axons and small vessels
- Impaired axonal transport leads to focal axonal swelling and may result in axonal disconnection
- DAI does NOT require direct head impact - sudden rotational deceleration is sufficient
Pathophysiology
- Mechanical deformation of neurons causes ion homeostasis disruption
- Excessive release of glutamate and excitotoxic neurotransmitters
- Intracellular calcium influx
- Activation of cytotoxic cascades (calpains, caspases)
- Later: microglial activation and inflammatory cytokine release
Common Locations of DAI
| Location | Clinical Significance |
|---|---|
| Corticomedullary (gray-white) junction | Most common site; frontal and temporal areas |
| Corpus callosum | Highly sensitive - near the falx cerebri |
| Upper brainstem and diencephalon | Fixed structures; torsional injury is devastating |
| Internal capsule | Deep white matter injury |
| Parasagittal white matter | Near rigid dural reflection |
(Bradley and Daroff's Neurology; Kaplan & Sadock's; Mulholland & Greenfield's Surgery)
Clinical Features
- Rapid progression to coma without specific focal lesions
- Severity of DAI correlates with duration of coma
- Severe DAI: patient may remain unconscious, vegetative, or severely disabled
- Lesser degrees of DAI are seen even in mild TBI
Imaging
- CT scan may appear normal in DAI (key point!)
- Classic CT finding: punctate hemorrhages at the gray-white junction and deep brain structures
- MRI is more sensitive - gradient echo (GRE) MRI detects hemorrhagic lesions; FLAIR is best for non-hemorrhagic lesions
- Diffusion Tensor Imaging (DTI) is the most sensitive modality - detects disrupted white matter tracts by measuring diffusion anisotropy
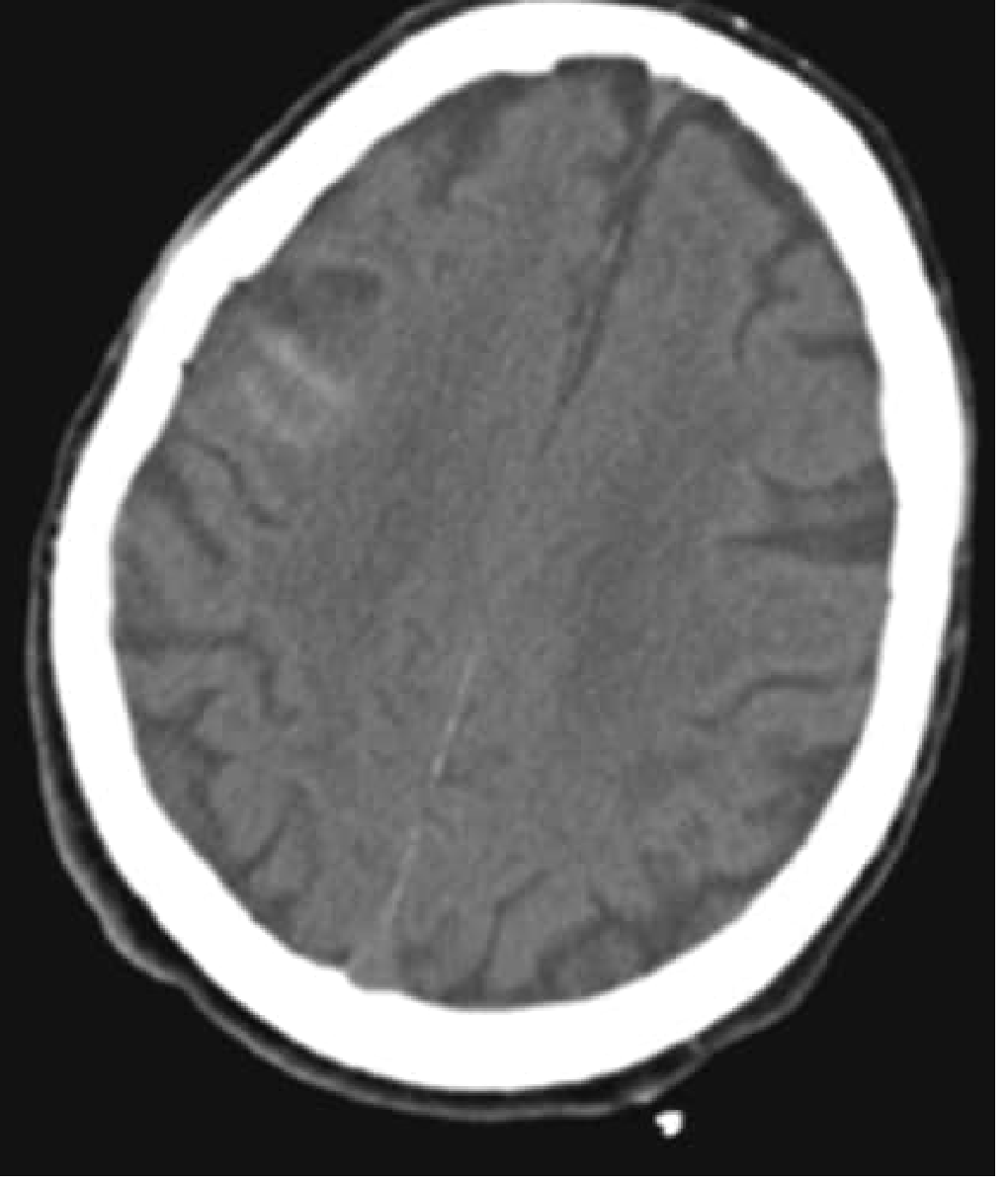
Axial CT scan of a trauma patient showing traumatic subarachnoid hemorrhage - a consequence of the vascular shearing that accompanies acceleration-deceleration injury. (Bradley and Daroff's Neurology)
4. Vascular Injuries from Shearing Forces
In addition to axonal disruption, shearing forces damage blood vessels:
- Deformation and stretching of blood vessels may lead to intracranial hemorrhages that can expand over hours to days after injury
- Bridging vein rupture causes subdural hematoma - particularly vulnerable because these veins traverse the subdural space across a distance that is stressed by relative movement between brain and skull
- Middle meningeal artery tear (from skull fracture) - epidural hematoma
- Intracerebral hemorrhage - from deeper vascular shearing
- Traumatic subarachnoid hemorrhage - from disruption of small surface vessels
5. Special Considerations
Pediatric Brain
The pediatric brain is less myelinated with higher water content, which predisposes it to shearing forces and a higher risk for DAI and post-traumatic seizures. (Rosen's Emergency Medicine)
Olfactory Nerve Injury
Rapid acceleration-deceleration causes shearing of the olfactory nerve filaments as they pass through the cribriform plate, producing post-traumatic anosmia. Blunt trauma to the occiput (with contrecoup frontal injury) is a particularly common cause. (Scott-Brown's Otorhinolaryngology)
Brainstem Torsion
The brainstem is the most fixed portion of the brain. Rotational and torsion injuries at this site (where it is anchored at the tentorium) can be immediately devastating, causing loss of consciousness and autonomic failure.
Summary Table
| Injury Type | Force Mechanism | Location | Key Feature |
|---|---|---|---|
| Coup contusion | Direct impact site | Ipsilateral cortex | Under point of impact |
| Contrecoup contusion | Inertial rebound | Opposite cortex | Frontal/temporal poles most common |
| Diffuse Axonal Injury | Rotational shearing | White matter, CC, brainstem | Coma without focal CT lesion |
| Subdural hematoma | Bridging vein shearing | Subdural space | Crescent shape; elderly at risk |
| Epidural hematoma | Middle meningeal artery | Epidural space | Biconvex; temporal skull fracture |
| Traumatic SAH | Surface vessel disruption | Subarachnoid space | Often accompanies DAI |
Sources:
- Guyton and Hall Textbook of Medical Physiology - CSF cushioning and coup/contrecoup mechanism
- Mulholland and Greenfield's Surgery, 7e - Primary brain injury and DAI
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Mechanisms of TBI, cellular cascades
- Bradley and Daroff's Neurology in Clinical Practice - DAI pathology and imaging
- Tintinalli's Emergency Medicine - DAI clinical features
- Rosen's Emergency Medicine - Pediatric vulnerability
- Scott-Brown's Otorhinolaryngology - Olfactory injury in coup/contrecoup
This is a shared conversation. Sign in to Orris to start your own chat.