Adenoid and Adenoid hypertrophy surgery
Reading File
Finding Sources
Searching PubMed
adenoid hypertrophy adenoidectomy
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative ENT textbooks. Let me compile the complete answer.
Adenoid and Adenoid Hypertrophy: A Comprehensive Overview
Anatomy
There is only one nasopharyngeal adenoid (despite the colloquial plural "adenoids"). It is a mass of lymphoid tissue situated on the posterior wall of the nasopharynx, forming part of Waldeyer's ring - the ring of lymphoid tissue encircling the upper aerodigestive tract. The adenoid sits in close proximity to the Eustachian tube orifices and the posterior choanae.
Physiology and Natural History
The adenoid is part of the immune system, involved in mucosal immunity of the upper airway. Key points regarding its natural history:
- Physiological hypertrophy is most common between ages 4 and 10
- The adenoid tissue normally undergoes spontaneous atrophy during puberty, though remnants may persist into adult life
- Adenoid hypertrophy in an adult should raise concern for a lymphoproliferative disorder or HIV infection
Adenoid Hypertrophy
Causes and Associations
- Physiological growth in childhood (most common)
- Recurrent/chronic upper respiratory infections
- Allergic rhinitis
- Laryngopharyngeal reflux (2025 meta-analysis, PMID 40958230, demonstrated a bidirectional risk association)
- Lymphoproliferative disease (in adults)
- HIV infection (in adults)
Clinical Features
Symptoms:
- Nasal obstruction (chronic or recurrent)
- Mouth breathing
- Rhinorrhoea
- Snoring
- Hyponasal speech
- Cough
- Otitis media with effusion (OME / "glue ear")
- Sleep disturbance
Signs:
- Adenoid facies: crowded teeth, high-arched palate, underdeveloped nostrils - from chronic mouth breathing
- Hyponasal voice
- Enlarged cervical lymph nodes
Endoscopic appearance:
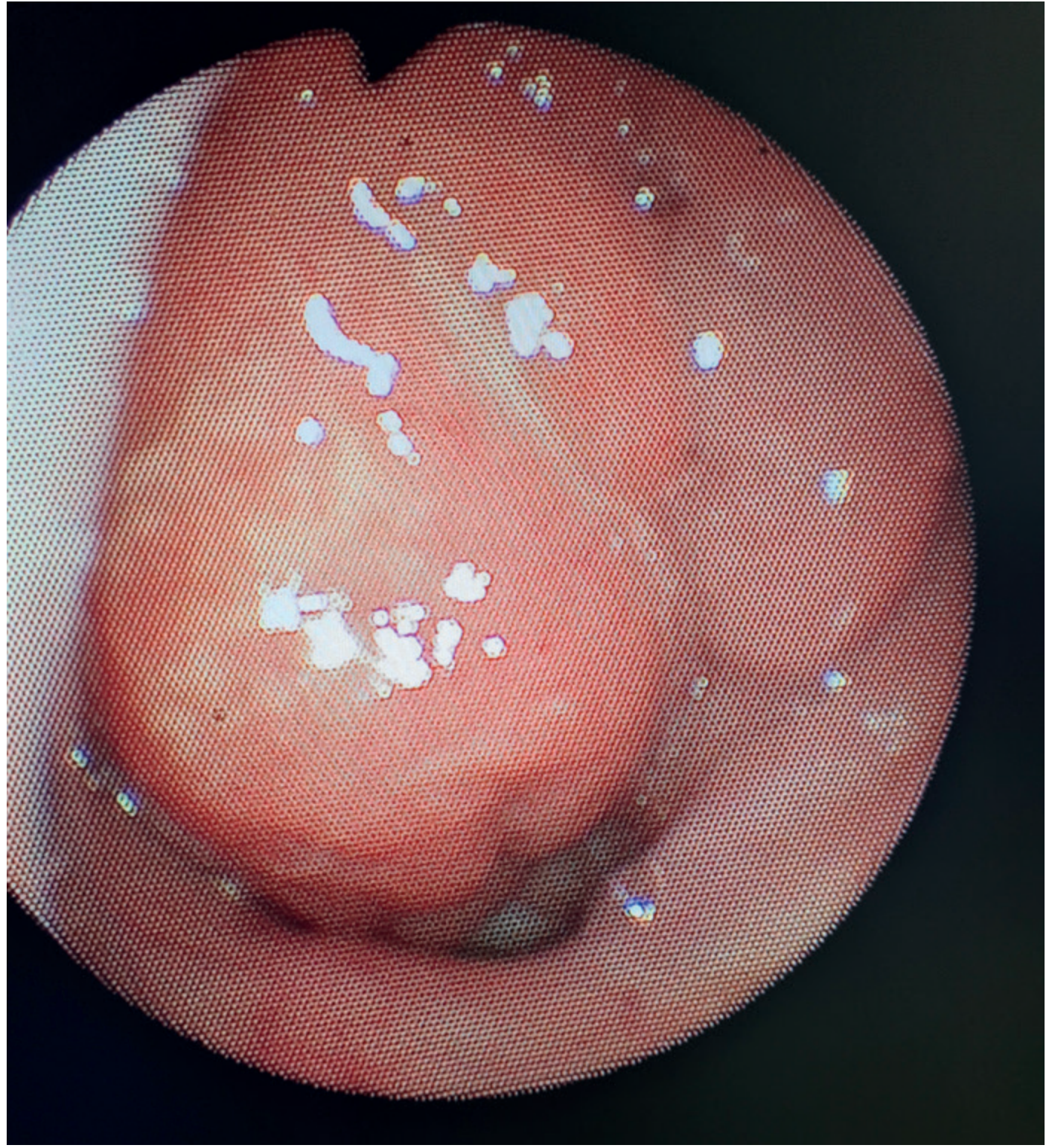
Endoscopic view of adenoid hypertrophy - Bailey and Love's Short Practice of Surgery
Grading of Adenoid Hypertrophy
Adenoid size is classified by the degree of choanal obstruction (Scott-Brown's Otorhinolaryngology):
| Grade | Description |
|---|---|
| Grade I | Adenoid tissue filling one-third of the vertical choanae |
| Grade II | One-third to two-thirds obstruction of the choanae |
| Grade III | Two-thirds to nearly complete obstruction |
| Grade IV | Complete obstruction of the choanae |
The size of the adenoid alone is not an indication for removal. What matters is the consequence of hypertrophy (e.g., nasal obstruction, OSA, OME). - Bailey & Love's, p. 803
Complications of Adenoid Hypertrophy
Obstructive Sleep Apnoea (OSA)
- Enlargement of the adenoid along with tonsillar hypertrophy can compromise the upper airway during sleep
- Symptoms: irregular snoring, apnoeic pauses, restlessness, abnormal sleep positions, daytime sleepiness
- Can cause sleep deprivation and secondary cardiac complications in children
- Has been implicated in some cases of sudden infant death syndrome
- Surgical removal of tonsils and adenoid is curative
Otitis Media with Effusion (OME)
- The adenoid acts as a bacterial reservoir in close proximity to the Eustachian tube
- Adenoids from children with chronic rhinosinusitis have a much larger portion of their surface area covered by biofilm (88-99%) compared to controls (0-6.5%)
- The contribution of the adenoids to CRS may relate more to their bacterial reservoir function than to their physical size
Chronic Rhinosinusitis (CRS)
- Adenoids share similar bacteriology with the middle meatuses of children with CRS
- Common organisms: alpha-hemolytic streptococci, S. aureus, S. pneumoniae, H. influenzae, M. catarrhalis
Investigations
- Nasendoscopy: the gold standard for assessing adenoid size in the outpatient setting - highly accurate; mirror examination underestimates choanal occlusion
- Lateral soft-tissue neck radiograph: useful when endoscopy is not tolerated; correlates well with endoscopic assessment; shows the pad of adenoid tissue in the postnasal space
- Sleep study (polysomnography): for suspected OSA - measures sleep pattern and arterial oxygenation
Medical (Non-Surgical) Management
- Traditionally, surgery or watchful waiting were the only options
- Evidence now supports topical intranasal corticosteroids for reduction in adenoid size with improvements in OME, audiometric thresholds, nasal obstruction, rhinorrhoea, cough, snoring and sleep apnoea
- Two 2025 meta-analyses (PMID 40609250, PMID 41056645) confirm the effectiveness and safety of intranasal corticosteroids for adenoid hypertrophy in children, though earlier trial quality was noted as poor
- Other measures: treatment of allergic rhinitis, nasal saline irrigation, antibiotic therapy for acute superimposed infection
Adenoidectomy (Surgical Management)
Indications
Adenoidectomy is one of the most frequently performed surgical procedures in children. Indications include:
- Nasal airway obstruction from adenoid hypertrophy causing significant symptoms
- Obstructive sleep apnoea / sleep-disordered breathing (often combined with tonsillectomy)
- Otitis media with effusion - adjuvant adenoidectomy as part of surgical management
- Chronic or recurrent rhinosinusitis unresponsive to medical therapy
- Recurrent acute otitis media
Where the indication is OME rather than obstruction, the size of the adenoid is not relevant - the bacteriological reservoir role is the key mechanism. - Scott-Brown's
Pre-operative Assessment
- Positive exclusion of history or family tendency of unusual bleeding or bruising (routine clotting screen may miss mild von Willebrand disease)
- Mandatory palate examination - assess for submucous cleft palate or bifid uvula (bifid uvula is a marker in 59% of submucous cleft cases); adenoidectomy may unmask pre-existing palatal dysfunction leading to velopharyngeal insufficiency
- Children with Down syndrome: consider atlantoaxial instability and cardiac abnormalities
- Nasendoscopy or lateral neck X-ray to assess adenoid size and grade
Surgical Techniques
1. Blind Curettage (Traditional)
- Most commonly used technique in the UK historically (79.2% of surgeons use digital palpation + blind curettage)
- Disadvantages: blind procedure, unpredictable bleeding (mean blood loss ~50 mL), poor access to choanal adenoid, risk of trauma to Eustachian tube cushions
- Less preferred in modern practice
2. Suction Diathermy (Suction Coagulation) - Direct Vision
- Affords direct vision with minimal blood loss (mean ~4 mL vs 50 mL with curettage)
- Effective haemostasis, negligible risk of post-operative haemorrhage
- Allows partial adenoidectomy (leaving a ridge of tissue at the inferior nasopharynx) to reduce risk of velopharyngeal insufficiency
- Meta-analysis confirmed: reduced intra-operative bleeding, reduced operative time, lower overall complication rate vs curettage
- Only 8.1% of UK surgeons currently use this approach, despite its advantages
3. Microdebrider (Powered Shaver) - Direct Vision
- 20% faster than curettage in RCT
- More expensive than suction coagulator; high unit cost is a disadvantage
4. Coblation - Direct Vision
- Less blood loss and more complete adenoid removal
- Cost limits application as a sole procedure
- Cost-effective when combined with tonsillectomy using the same Coblation wand
5. Laser (KTP / Gold)
- KTP laser: associated with high risk of nasopharyngeal stenosis - not recommended
- Gold laser: small series suggest a lower complication profile
Anaesthesia and Post-operative Care
- Majority of children can be safely discharged same day with appropriate surgical/anaesthetic technique, pre-emptive fluid replacement, antiemetics and analgesia
- Avoid sedative premedications and opiate analgesics post-operatively in children with OSA (risk of further respiratory depression)
- Continuous positive airway pressure (CPAP) may be required in adults with residual obstruction
Complications of Adenoidectomy
| Complication | Details |
|---|---|
| Primary haemorrhage | Risk reduced with direct-vision techniques |
| Secondary haemorrhage | Rare; can be delayed 5-10 days post-op |
| Nasopharyngeal blood clot | Must suction clear before removing the gag - risk of "coroner's clot" causing acute airway obstruction |
| Velopharyngeal insufficiency (VPI) | Estimated 1:1500 to 1:10,000; hypernasal speech, nasal regurgitation; risk increases if submucous cleft undetected |
| Infection / Foetor | Clinically uncommon; post-op antibiotics (e.g., azithromycin 10 mg/kg x3 days) reduce odour especially after suction adenoidectomy |
| Grisel syndrome | Non-traumatic atlantoaxial subluxation (C1-C2); rare but recognized; presents as post-op torticollis; higher risk in Down syndrome |
| Retropharyngeal abscess | Rare complication from trauma and secondary infection of the adenoid bed |
| Recurrence | Adenoid regrowth can occur, especially in younger children |
Key Clinical Notes
- Combining adenoidectomy with tonsillectomy is no longer appropriate unless there is a specific indication for adenoidectomy (Scott-Brown's, p. 6487)
- Behavioural and cognitive changes related to OSA are reversible with adenoidectomy
- The adenoid regresses spontaneously with puberty - this should factor into the decision to operate in younger adolescents
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 803
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
- Cummings Otolaryngology Head and Neck Surgery
- K.J. Lee's Essential Otolaryngology
- Textbook of Family Medicine, 9th Ed.
- Recent evidence: Alqutub A et al. (2025) PMID 40609250 - intranasal corticosteroids effective for adenoid hypertrophy; Ripp AT et al. (2025) PMID 41056645 - topical nasal steroids meta-analysis; Li C et al. (2025) PMID 40958230 - bidirectional association with laryngopharyngeal reflux
This is a shared conversation. Sign in to Orris to start your own chat.