Can I get the explain from latest guidelines for osteoarthritis with pain relief with nsaids indication,doses,monitoring,duration of therapy ,x ray findings
Reading File
Finding Sources
Searching PubMed
osteoarthritis management NSAID guidelines
Searching the Web
osteoarthritis NSAID guidelines 2024 2025 ACR EULAR indications dose monitoring
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
NSAID osteoarthritis indication dose monitoring duration
Loading Image
Finding Sources
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full, structured response.
Osteoarthritis: NSAIDs for Pain Relief - Guidelines-Based Review
1. Background: Why NSAIDs Work in OA
OA pain is driven by synovial inflammation and subchondral bone marrow lesions (BMLs) that activate nociceptors via prostaglandin (PGE2) synthesis through COX-1 and COX-2 enzymes. NSAIDs inhibit both COX isoforms (non-selective) or primarily COX-2 (coxibs), reducing PGE2 production and thereby reducing pain and stiffness. A meta-analysis of 72 RCTs with >26,000 patients found NSAIDs produce moderate, statistically significant effects on pain and function that peak at 2 weeks and begin declining by 8 weeks in knee OA.
- Firestein & Kelley's Textbook of Rheumatology, p. 9015-9031
2. Indications
NSAIDs are indicated in OA when:
- Topical agents (first preference for localized knee/hand OA, especially in older adults or those with GI/CV risk) have failed or when disease is more widespread
- Moderate-to-severe joint pain unresponsive to acetaminophen, exercise, weight loss, or physical therapy
- Flares of OA pain requiring short-term systemic analgesia
- Patients with significant inflammatory component (morning stiffness, joint swelling)
Current ACR/EULAR and multiple guidelines place oral NSAIDs as a strongly recommended first-line pharmacologic therapy, while recommending topical NSAIDs preferentially for older adults due to equal efficacy but lower systemic risk. Oral NSAIDs are appropriate for more widespread or more severe symptoms at the lowest dose and shortest duration possible.
- ACR/AF 2019 OA Guidelines; Nonoperative Management Recommendations for Knee OA, PMC 2025
3. NSAID Selection & Doses
| NSAID | Usual Anti-inflammatory Dose | Maximum Daily Dose |
|---|---|---|
| Ibuprofen | 400-800 mg TID | 3200 mg/day |
| Naproxen | 250-500 mg BID | 1000-1500 mg/day |
| Diclofenac (oral) | 50 mg BID-TID | 150 mg/day |
| Diclofenac (topical 1%) | Apply to affected joint QID | - |
| Celecoxib (COX-2) | 100-200 mg OD or BID | 400 mg/day |
| Meloxicam | 7.5-15 mg OD | 15 mg/day |
| Indomethacin | 25-50 mg TID | 150 mg/day (avoid in elderly) |
Key points:
- Naproxen is preferred when CV risk is a concern (most cardiovascular-neutral among oral NSAIDs), combined with a PPI
- Celecoxib (COX-2 selective) is preferred when GI risk is the main concern, though it increases CV risk
- Topical diclofenac (1% gel) is preferred in elderly and those with GI or renal concerns - equivalent efficacy, much lower systemic absorption
4. Risk-Stratified Prescribing (Firestein & Kelley Framework)
| Risk Category | Patient Profile | Recommended NSAID Strategy |
|---|---|---|
| Low | <65 yr, no CV risk factors, no chronic therapy needed, no concurrent aspirin/anticoagulants | Traditional NSAID at shortest duration and lowest dose possible |
| Intermediate | ≥65 yr, no history of complicated GI ulcer, low CV risk, possibly on low-dose aspirin, may need chronic/high-dose therapy | Traditional NSAID + PPI/misoprostol/high-dose H2RA; OR once-daily celecoxib + PPI if taking aspirin; if on aspirin, take traditional NSAID ≥2 hrs before aspirin |
| High | Elderly/frail, hypertension, renal/liver disease, history of complicated ulcer or multiple GI risk factors, on aspirin for secondary CV prevention, history of heart failure | Prefer acetaminophen <2 g/day; avoid chronic NSAIDs; if needed: intermittent dosing, low-dose short half-life NSAID; celecoxib + PPI if GI > CV risk; naproxen + PPI if CV > GI risk; monitor BP, creatinine, electrolytes |
- Firestein & Kelley's Textbook of Rheumatology, block 14, p. 141-168
5. Duration of Therapy
- Goal: shortest effective duration - use NSAIDs intermittently for pain flares rather than continuously
- Anti-inflammatory/analgesic effect peaks at 2 weeks, begins declining by 8 weeks
- GI adverse events increase significantly as early as 4 weeks after initiation
- For chronic OA: use intermittent "as-needed" dosing where possible; reassess need at each visit
- Do not use extended-release formulations in high-risk patients
- If ongoing pain control is needed despite multiple risk factors, consider alternative agents (duloxetine, tramadol) or intra-articular injections
6. Monitoring
Baseline (before starting)
- BP - NSAIDs cause sodium retention, fluid retention, and can raise BP or worsen heart failure
- Renal function (creatinine, eGFR) - NSAIDs reduce renal prostaglandins, can precipitate AKI especially in the elderly, dehydrated, or those with CKD
- Liver function - baseline ALT/AST
- CBC - particularly if prolonged use anticipated
- GI history - prior peptic ulcer, GI bleed
- Cardiovascular history - prior MI, stroke, heart failure
Ongoing Monitoring
| Parameter | Frequency |
|---|---|
| Blood pressure | At each visit |
| Serum creatinine/electrolytes | 1-2 weeks after starting, then every 3-6 months if chronic use |
| CBC (for GI blood loss) | Every 3-6 months if chronic use |
| Symptoms of GI toxicity | Every visit (epigastric pain, melena) |
| Cardiovascular symptoms | Every visit (edema, dyspnea, chest pain) |
Special Populations Requiring Extra Caution
-
Elderly - substantially higher risk of GI bleed, renal impairment, and heart failure exacerbation; prefer topical NSAIDs or acetaminophen
-
CKD - avoid or use with great caution; monitor creatinine closely; NSAIDs can cause acute tubular necrosis and hyperkalemia
-
Heart failure - NSAIDs can worsen fluid retention and precipitate decompensation
-
Anticoagulant/antiplatelet users - significantly increased bleeding risk
-
Elderly (>65) on NSAIDs: PPI co-prescription is mandatory to reduce GI risk
-
Harrison's Principles of Internal Medicine 22E, p. 2239; Firestein & Kelley, p. 9015-9038
7. Contraindications to NSAIDs in OA
- Active peptic ulcer or recent GI bleed
- Severe renal impairment (eGFR <30 mL/min)
- Severe hepatic impairment
- History of aspirin/NSAID-induced asthma or urticaria
- Third trimester of pregnancy
- Severe heart failure (NYHA Class III-IV)
- Recent CABG (first 10-14 days post-op)
8. Radiographic (X-ray) Findings in OA
The classic plain film changes of OA represent a combination of destruction and repair. The four cardinal findings (mnemonic: LOSS):
1. Joint Space Narrowing (Loss of Cartilage)
Asymmetric narrowing of the joint space, occurring preferentially in areas of mechanical stress (e.g., medial compartment of knee leading to varus deformity). This asymmetry distinguishes OA from inflammatory arthritis (RA), which causes symmetric narrowing.
2. Osteophyte Formation
Marginal osteophytes (bone spurs) at joint margins represent the hypertrophic/repair component. They consist of trabeculated new bone and may form on one or both sides of the joint. Periarticular osteophytes are the most specific finding for OA.
3. Subchondral Changes
- Subchondral sclerosis (increased bone density adjacent to the joint surface due to osteoblastic activity)
- Subchondral cysts (geodes) - formed by synovial fluid entering the bone through damaged cartilage
4. Joint Deformity and Loose Bodies
- Ligamentous laxity with joint malalignment (varus in medial knee OA)
- Intra-articular loose bodies (osteochondral fragments that may calcify and enlarge)
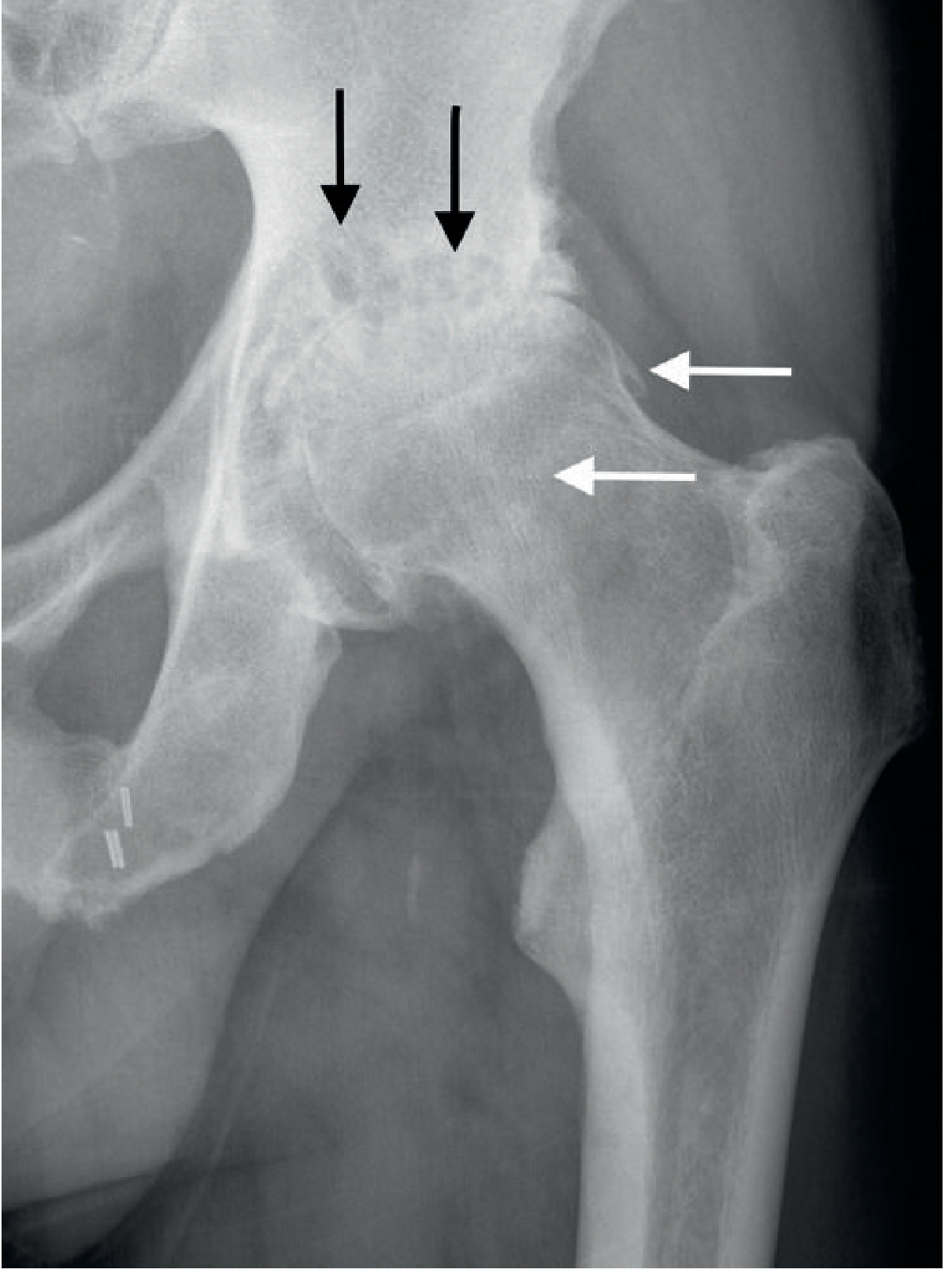
X-Ray: Severe Hip OA - note asymmetric superior joint space loss, subchondral cysts (black arrows), and rim osteophytes (white arrows):
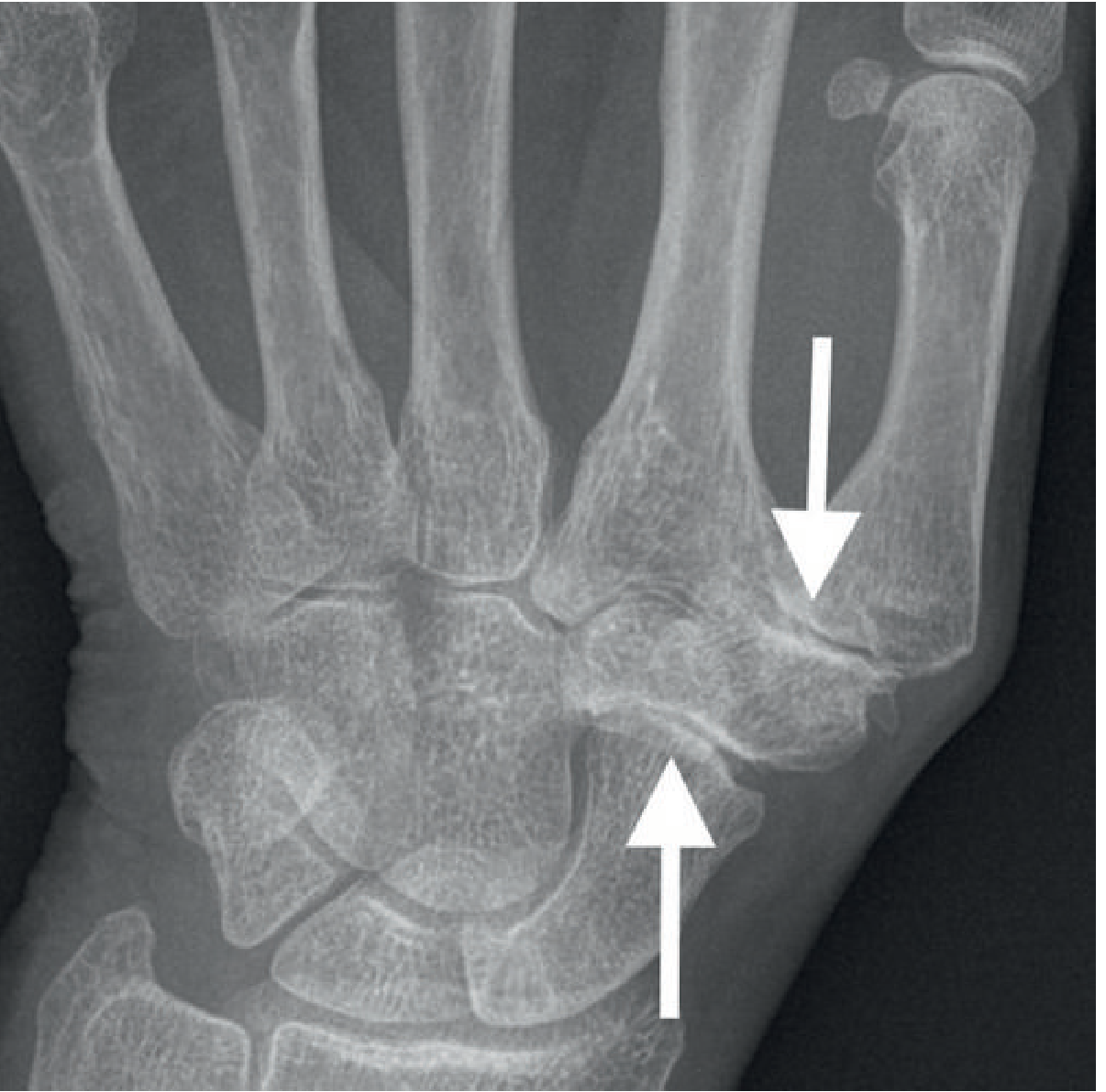
X-Ray: OA at Thumb Base (CMC joint) - loss of joint space, subchondral sclerosis, osteophyte formation at the 1st carpometacarpal and scaphotrapeziotrapezoid joints:
- Grainger & Allison's Diagnostic Radiology, p. 1113-1114
Site-Specific X-Ray Patterns
| Joint | Typical X-Ray Pattern |
|---|---|
| Knee | Medial compartment narrowing (varus) > lateral > patellofemoral; weight-bearing views essential; tibial spiking |
| Hip | Superior joint space narrowing (most common), superolateral or medial patterns |
| Hand (DIP/PIP) | Heberden's nodes (DIP) and Bouchard's nodes (PIP), osteophytes |
| Thumb base (1st CMC) | Pantrapezial pattern, "shelf" osteophyte |
| Spine | Disc space narrowing, vertebral osteophytes (spondylosis), facet joint OA |
9. Step-Up Treatment Ladder (Guideline Summary)
Step 1 (non-pharmacologic): Exercise, weight loss, physiotherapy, patient education
↓
Step 2 (topical): Topical NSAIDs (diclofenac 1% gel), topical capsaicin
↓
Step 3 (oral): Acetaminophen 500mg-1g TID (limited evidence but low risk)
↓
Step 4 (oral NSAID): Lowest effective dose, shortest duration, with GI/CV risk stratification
↓
Step 5 (adjuncts): Duloxetine (SNRi), tramadol (weak opioid)
↓
Step 6 (intra-articular): Corticosteroid injections (short-term flares), hyaluronic acid
↓
Step 7 (surgical): Joint replacement when conservative measures fail
10. Recent Evidence Update (PubMed 2023-2025)
A 2023 systematic review of clinical practice guidelines (PMID 37394226) covering hip and knee OA confirmed that oral NSAIDs remain strongly recommended across international guidelines (ACR, EULAR, OARSI, NICE) for symptom management. A recent umbrella review of celecoxib safety (PMID 40911151) confirmed celecoxib's favorable GI profile but noted cardiovascular caution applies to all COX-2 inhibitors.
Sources: Firestein & Kelley's Textbook of Rheumatology | Harrison's Principles of Internal Medicine 22E | Grainger & Allison's Diagnostic Radiology | Goldman-Cecil Medicine | ACR/AF 2019 OA Guidelines | PMC Nonoperative Management of Knee OA 2025
This is a shared conversation. Sign in to Orris to start your own chat.