Wound healing ms ortho 20 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content. Let me compile the full 20-mark MS Ortho answer based on all the retrieved material.
Wound Healing
MS Orthopaedics - 20 Marks
Introduction
Wound healing is a complex, dynamic, and highly coordinated biological process that restores the structural and functional integrity of damaged tissue. It involves a cascade of cellular and biochemical events that overlap temporally, involving hemostasis, inflammation, proliferation, and remodeling. Understanding wound healing is fundamental to surgery, particularly orthopaedics, where wounds involving bone, cartilage, tendon, and soft tissue are commonly encountered.
Classification of Wounds
By Mechanism:
- Incised wounds - clean edges, heal by primary intention
- Lacerated wounds - ragged edges, higher infection risk
- Crush injuries - devitalized tissue, poor vascularity
- Avulsion injuries - loss of tissue
By Contamination (Surgical wound classification - CDC):
| Class | Type | Description |
|---|---|---|
| I | Clean | Non-traumatic, no break in sterile technique |
| II | Clean-contaminated | Minor break, hollow viscus entered |
| III | Contaminated | Open traumatic wound, gross contamination |
| IV | Dirty/infected | Perforated viscus, established infection |
By Depth:
- Superficial (epidermis only)
- Partial thickness (epidermis + superficial dermis)
- Full thickness (through all skin layers)
Types of Wound Healing
1. Primary Intention (Primary Union / First Intention)
- Wound edges are approximated by sutures, staples, or glue
- Minimal tissue loss, minimal scar
- Rapid epithelialization (<48 hours for incised wounds)
- Minimal granulation tissue formation
- Example: surgical incisions, clean lacerations repaired promptly
2. Secondary Intention (Secondary Union)
- Wound edges are NOT approximated; allowed to heal by granulation
- Occurs in large, infected, or contaminated wounds
- Extensive granulation tissue, wound contraction, and more scarring
- Prolonged healing time
- Example: open fracture wounds, pressure sores, abscess cavities
3. Tertiary Intention (Delayed Primary Closure)
- Wound is initially left open (due to contamination or infection)
- Closed surgically 4-5 days later after control of infection
- Intermediate scar formation
- Example: contaminated traumatic wounds, open fractures
Phases of Wound Healing
The wound healing process is traditionally divided into 4 overlapping phases. The diagram below illustrates the timeline:
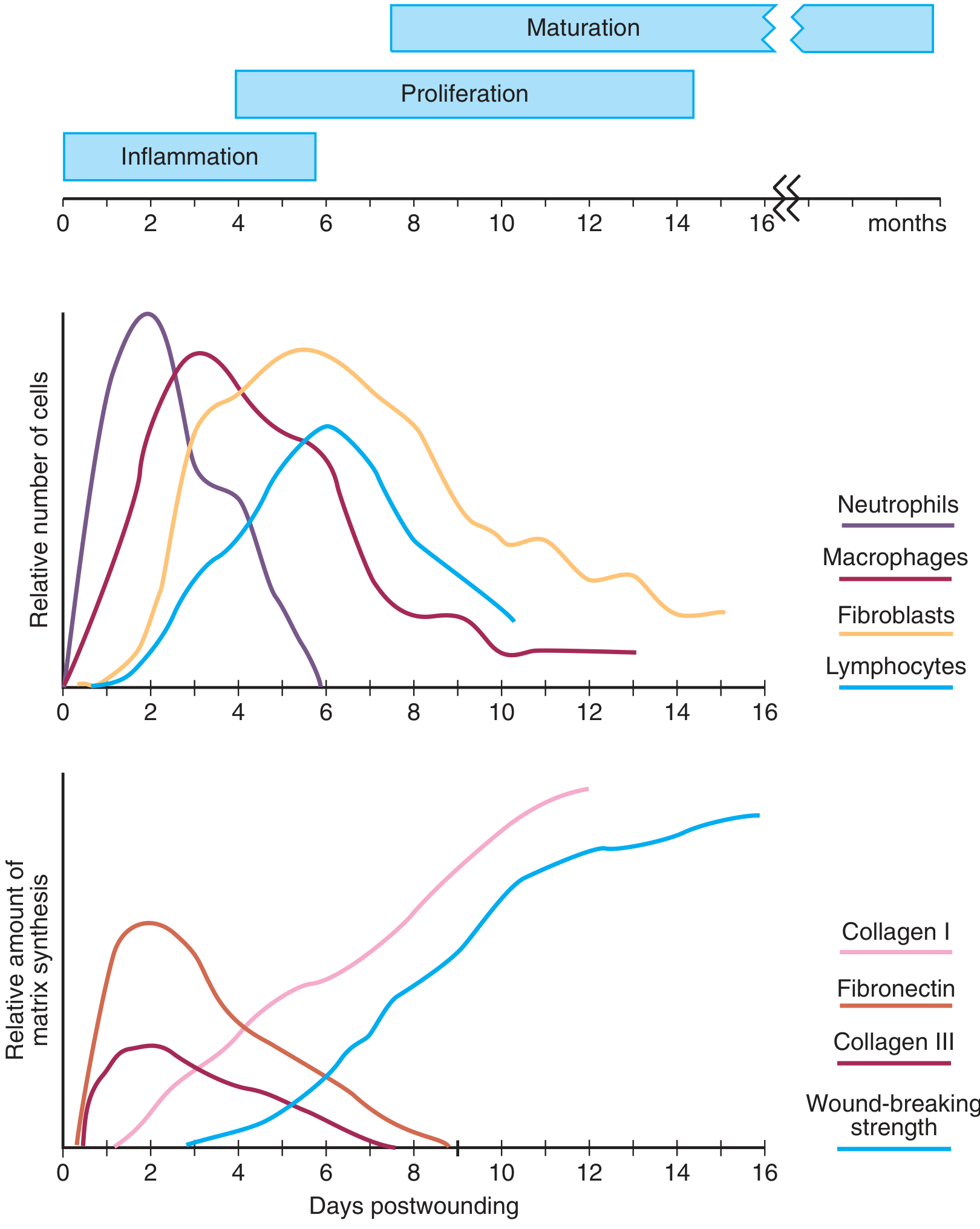
Phase 1: Hemostasis (Minutes to Hours)
Immediately after injury, severed blood vessels constrict (vasoconstriction, mediated by thromboxane A2 and endothelin). This is followed by:
- Platelet activation: Exposed subendothelial collagen triggers platelet aggregation and degranulation
- Coagulation cascade activation: Formation of fibrin clot
- Release of wound-active substances from platelet alpha granules:
- Platelet-Derived Growth Factor (PDGF)
- Transforming Growth Factor-beta (TGF-β)
- Platelet-Activating Factor (PAF)
- Fibronectin
- Serotonin
The fibrin clot achieves hemostasis AND serves as a scaffold for subsequent inflammatory cell migration into the wound.
Phase 2: Inflammation (Days 1-4)
Cellular infiltration after injury follows a characteristic, predetermined sequence:
Neutrophils (PMNs) - Days 1 to 2 (peak 24-48 hours)
- First cells to arrive at the wound
- Attracted by: complement factors, IL-1, TNF-α, TGF-β, platelet factor 4, bacterial products
- Primary role: phagocytosis of bacteria and tissue debris
- Release proteases (collagenases) for matrix debridement
- Release TNF-α which influences angiogenesis and collagen synthesis
- Important: neutrophils are NOT essential for collagen deposition or wound strength; their factors may actually delay epithelial closure
Macrophages - Days 2 to 4 (peak 48-96 hours)
- Derived from circulating monocytes - essential to successful healing
- Persist until wound healing is complete
- Functions:
- Phagocytosis and debridement
- Oxygen radical and nitric oxide synthesis (microbial stasis)
- Activation and recruitment of other cells via cytokines/growth factors
- Release TGF-β, VEGF, IGF, EGF, lactate
- Regulate cell proliferation, matrix synthesis, angiogenesis
- Macrophage depletion leads to severely impaired wound healing
T Lymphocytes - Days 5 to 7
- Arrive after macrophages
- Modulate fibroblast proliferation
- Regulate matrix synthesis through cytokine release
- Bridge inflammation and proliferation phases
Phase 3: Proliferation (Days 4 to 21)
This phase involves three key events: angiogenesis, fibroplasia/collagen synthesis, and epithelialization.
Fibroplasia (Fibroblast Activity)
- Fibroblasts are recruited from local connective tissue by PDGF, FGF, TGF-β
- Begin arriving at 48-72 hours; peak activity at day 5-7
- Fibroblasts are the principal source of extracellular matrix (ECM) proteins
- Produce collagen (initially Type III, later replaced by Type I), proteoglycans, fibronectin
- Fibroplasia produces granulation tissue: a highly vascularized tissue with loose collagen framework
Collagen Synthesis
- The main structural protein of healed wounds
- Type III collagen predominates initially (fetal type, more flexible)
- Gradually replaced by Type I collagen (stronger, less flexible) during remodeling
- Collagen synthesis requires: adequate oxygen, vitamin C (ascorbic acid for hydroxylation of proline/lysine), zinc, iron
Angiogenesis (Neovascularization)
- Stimulated by VEGF, FGF, low pO2, lactate, macrophage-derived factors
- New capillary buds grow into the wound, providing oxygen and nutrients
- Critical for granulation tissue formation
Granulation Tissue
- Characterized by new capillaries (appear as red granules on wound surface), fibroblasts, and loose collagen matrix
- Fills the wound defect; provides the scaffold for epithelialization
Myofibroblasts and Wound Contraction
- Fibroblasts differentiate into myofibroblasts (express alpha-smooth muscle actin)
- Responsible for wound contraction - reducing wound size
- Contraction is distinct from contracture (permanent shortening leading to deformity)
- Maximum contraction: days 5-15
- Clinically important: excessive contraction over joints causes contractures
Epithelialization
- Begins within 24 hours of injury at wound edges
- Marginal basal cells lose dermal attachment, enlarge, and migrate across provisional matrix
- Fixed basal cells undergo rapid mitotic divisions - cells migrate in "leapfrog" fashion
- Stimulated by: EGF, TGF-β, bFGF, PDGF, IGF-1, fibronectin
- Reepithelialization complete in <48 hours for approximated wounds
Phase 4: Maturation and Remodeling (Days 21 to Months-Years)
- Begins at ~day 21 and continues for months to years (up to 2 years)
- Hallmark: replacement of Type III collagen by Type I collagen
- This is mediated by matrix metalloproteinases (MMPs) and their inhibitors (TIMPs)
- TGF-β increases new collagen transcription AND decreases collagen breakdown
- Collagen fibers reorient along lines of stress (from random to parallel arrangement)
- Wound tensile strength increases progressively:
- Day 7: ~10% of original strength
- Day 21: ~20%
- 3 months: ~55%
- Final strength: ~70-80% of original tissue (never reaches 100%)
- Wound vascularity decreases, granulation tissue matures into scar tissue
Growth Factors in Wound Healing
| Growth Factor | Source | Action |
|---|---|---|
| PDGF | Platelets, macrophages | Fibroblast proliferation, collagen synthesis, chemotaxis |
| TGF-β | Platelets, macrophages, fibroblasts | Collagen synthesis, inhibits degradation, scar formation |
| EGF | Platelets, macrophages | Epithelialization, fibroblast proliferation |
| VEGF | Macrophages, endothelium | Angiogenesis |
| FGF (bFGF) | Macrophages, mast cells | Angiogenesis, fibroblast proliferation |
| IGF-1 | Liver, fibroblasts | Collagen synthesis, cell proliferation |
Healing in Specific Tissues (Orthopaedic Relevance)
Bone Healing
- Hematoma formation (0-3 days): fracture site bleeds, clot forms
- Inflammatory phase (1-7 days): cytokines attract osteoprogenitor cells
- Soft callus (1-3 weeks): fibroblasts and chondrocytes produce fibrocartilaginous callus
- Hard callus (3-12 weeks): osteoblasts replace cartilaginous callus with woven bone
- Remodeling (months-years): woven bone replaced by lamellar bone along lines of stress (Wolff's law)
Tendon Healing
- Intrinsic healing (from tenocytes within the tendon itself) - produces stronger repair
- Extrinsic healing (from surrounding paratenon/peritenon) - produces adhesions
- Three phases: inflammation (0-5 days), proliferation (5 days to 6 weeks), remodeling (6 weeks+)
- Full tensile strength takes 6-12 months
Cartilage Healing
- Poor intrinsic healing capacity due to avascularity
- Hyaline cartilage does NOT regenerate; replaced by fibrocartilage
- Full thickness defects reaching subchondral bone may partially heal via marrow elements
Nerve Healing
- Wallerian degeneration occurs distal to injury
- Regeneration rate: 1 mm/day (proximal progressing distally)
- Classified by Seddon (neurapraxia, axonotmesis, neurotmesis) and Sunderland
Factors Affecting Wound Healing
Local Factors
| Factor | Effect |
|---|---|
| Infection | Most common cause of impaired healing; >10^5 organisms/gram tissue prevents healing |
| Blood supply / Ischemia | Impairs oxygen delivery; essential for collagen synthesis and bacterial killing |
| Foreign bodies | Perpetuate inflammation, prevent healing |
| Wound tension / Movement | Impairs epithelialization; over joints can cause failure |
| Hematoma / Dead space | Nidus for infection, physical barrier |
| Radiation | Obliterative endarteritis, impairs vascularity |
Systemic Factors
| Factor | Effect |
|---|---|
| Malnutrition / Hypoproteinemia | Serum albumin <2 g/dL causes wound dehiscence and impaired healing; protein supplements reverse this |
| Vitamin C deficiency | Impairs collagen hydroxylation; classic example: scurvy |
| Vitamin A deficiency | Impairs epithelialization and fibroplasia |
| Zinc deficiency | Cofactor for multiple metalloenzymes; impairs fibroplasia |
| Iron deficiency / Anemia | Impairs oxygen delivery |
| Diabetes mellitus | Impairs neutrophil function, vascularity, growth factor activity, collagen synthesis |
| Corticosteroids | Suppress all phases of healing; anti-inflammatory effect reduces fibroplasia |
| Immunosuppression (HIV, chemotherapy) | Increased infection risk, impaired cellular responses |
| Age (elderly) | Decreased collagen synthesis, impaired immune response, comorbidities |
| Smoking | Nicotine causes vasoconstriction; CO reduces O2 delivery; impairs neutrophil function |
| Jaundice / Uremia | Metabolic impairment of fibroblast function |
| Malignancy | Catabolic state, immunosuppression |
Abnormal (Pathological) Wound Healing
Hypertrophic Scar
- Excessive collagen deposition WITHIN wound boundaries
- Raised, red, pruritic scar
- Regresses spontaneously over months to years
- Treatment: pressure garments, silicone gel, intralesional steroids
Keloid
- Collagen deposition EXTENDS BEYOND original wound margins ("finger-like" projections)
- Does NOT regress spontaneously
- More common in darker skin types (African descent)
- Common sites: face, earlobes, deltoid, presternal region
- More resistant to treatment
- Treatment: repeated excision + adjuvant radiotherapy, intralesional steroids, compression
- Key difference from hypertrophic scar: extends beyond wound margins, does not regress
Wound Dehiscence
- Separation of wound edges, typically at 5-10 days
- Causes: infection, poor nutritional status, obesity, technical failure, excessive tension
- Management: reclose surgically (if clean) or allow healing by secondary intention
Chronic Non-Healing Wounds
- Failure to proceed through normal healing sequence
- Stuck in prolonged inflammatory phase
- Causes: diabetes, peripheral vascular disease, pressure, infection, biofilm
- Examples: diabetic foot ulcers, venous ulcers, pressure sores
Contracture
- Excessive wound contraction causing functional disability
- Particularly problematic over joints in burns
- Prevention: early skin grafting, splinting, physiotherapy
Summary Table: Key Events and Timeline
| Phase | Timing | Key Cells | Key Events |
|---|---|---|---|
| Hemostasis | Minutes | Platelets | Vasoconstriction, clot, PDGF/TGF-β release |
| Inflammation | Days 1-4 | Neutrophils (peak 24-48h), Macrophages (48-96h) | Debridement, cytokine release, chemotaxis |
| Proliferation | Days 4-21 | Fibroblasts, endothelium, epithelium | Collagen III, granulation tissue, neovascularization, epithelialization, wound contraction |
| Remodeling | Day 21 to years | Fibroblasts, myofibroblasts | Collagen III → I, MMP activity, tensile strength to 70-80% |
Wound Management Principles
- Control hemorrhage - direct pressure, tourniquet if needed
- Irrigation - copious saline lavage reduces bacterial load
- Debridement - remove devitalized tissue (biological, surgical, or chemical)
- Dead space elimination - layered closure
- Appropriate dressing:
- Maintain moist wound environment (increases epithelialization by 50%)
- Absorb exudate, protect from infection
- Nutritional optimization - protein, vitamins A & C, zinc supplementation
- Control infection - antibiotics when indicated, wound cultures
- Negative Pressure Wound Therapy (NPWT/VAC): promotes granulation, reduces edema
- Hyperbaric oxygen - for refractory wounds, particularly in diabetics
Conclusion
Wound healing is a precisely regulated process fundamental to surgical practice. In orthopaedics, the principles apply to skin wounds, fracture healing, tendon, cartilage, and nerve repair. A thorough understanding of the four phases (hemostasis, inflammation, proliferation, remodeling), the cellular and molecular mediators, factors that impair healing, and pathological outcomes (keloids, hypertrophic scars, chronic wounds, contractures) allows the orthopaedic surgeon to optimize outcomes and prevent complications.
Sources:
- Schwartz's Principles of Surgery, 11th ed., Chapter 9 - Wound Healing
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Sabiston Textbook of Surgery - The Biological Basis of Modern Surgical Practice
- Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.