# Pathophysiological Compendium & Complete Case Analysis This comprehensive analysis systematically connects this patient's lifetime exposures, past oncology treatments, genetic anatomy variants, and hemodynamic variables to construct a unified pathophysiological explanation of his entire clinical presentation. ## 1. Longitudinal Timeline & The "Dual-Hit" Vascular Injury The severe Peripheral Arterial Disease (PAD) presenting as a diffuse, leaking groin aneurysm and a downstream acute-on-chronic embolic crisis is the product of a distinct "dual-hit" pathological process. ``` +-------------------------------------------------------------------------+ | HIT 1 | | 62-Pack-Year Tobacco Toxins + Chronic Mechanical Hypertension (150mmHg)| +-------------------------------------------------------------------------+ │ ▼ Chronic Endothelial Shear Injury │ ▼ Subendothelial LDL Infiltration & Macrophage Activation │ ▼ Foam Cell & Fatty Streak Formation │ ▼ Smooth Muscle Proliferation & Fibrous Cap │ ▼ Atherosclerotic Plaque Calcification (Crescentic Shells on CT) │ │ +--------------------------------───┴─────────────────────────────────────+ | HIT 2 | | Historic High-Dose Pelvic Radiotherapy (4500 cGy Pelvis / 6900 cGy) | +-------------------------------------------------------------------------+ │ ▼ Obliterative Endarteritis of the Microscopic Vasa Vasorum │ ▼ Total Microvascular Occlusion -> Hypoxic Starvation of Vessel Wall │ ▼ Coagulative Ischemic Necrosis of Tunica Media │ ▼ Permanent Structural Erasure of Elastic and Muscular Fibers │ ▼ Brittle, Rigid, Non-Compliant, Unstable Inflow Network (PAD) ``` ### Hit 1: Lifestyle & Metabolic Atherogenesis For 30 years, the patient smoked one pack of cigarettes daily, followed by 32 years of pipe-smoking, accumulating a **62-pack-year history of tobacco exposure**. * **Endothelial Shearing:** Inhaled nicotine and polycyclic aromatic hydrocarbons act as potent circulating chemical toxins. These compounds directly sheared the delicate inner endothelial monolayer of his large and medium-sized arteries. This chemical trauma was compounded by chronic, poorly controlled **hypertension** (150/80\text{ mmHg}), which applied continuous, raw mechanical stress to the vessel walls. * **The Lipid Cascade:** Endothelial injury breached the blood-artery barrier, allowing circulating Low-Density Lipoprotein (LDL) cholesterol to infiltrate the subendothelial space of the tunica intima. These lipids underwent chemical oxidation, transforming into highly immunogenic molecules. * **Foam Cell and Plaque Formation:** Circulating monocytes migrated into the vessel wall, differentiating into macrophages to engulf the oxidized LDL. These cells became bloated, fat-filled **foam cells**, forming foundational fatty streaks. Over decades, smooth muscle cells migrated from the media to the intima, secreting collagen to lock this fatty core beneath a fibrous cap, establishing advanced atherosclerotic plaques. * **Dystrophic Calcification:** As these plaques aged, cellular death (necrosis) occurred within their cores. Intracellular calcium pumps failed, causing a massive release of calcium ions into the necrotic tissue debris. These ions bound to negatively charged phosphate groups on broken cell membrane fragments, precipitating as **calcium phosphate** and reorganizing into rock-hard **hydroxyapatite crystals**. On his pelvic CT scan, this process is visible as the **"scattered crescentic calcifications present adjacent to the arterial lumen."** These rigid, crescent-shaped shells are the calcified structural outlines of his underlying atherosclerotic plaques. ### Hit 2: Iatrogenic Radiation-Induced Vascular Obliteration Ten years prior to this admission, the patient received a massive dose of ionizing radiation to treat an aggressive stage \text{B}_1 adenocarcinoma of the prostate gland: **4500 cGy to the wider pelvis**, followed by a localized booster dose of **6900 cGy straight to the prostatic bed**, delivered via a 4-MeV linear accelerator. * **Endarteritis Obliterans:** Large, thick conduits like the external iliac and common femoral arteries cannot absorb oxygen directly from the high-velocity blood rushing through their main channels. Instead, they rely on a network of microscopic capillaries looping through their outer walls called the **Vasa Vasorum** ("the vessels of the vessels"). The high-energy radiation beams blasted through these groin tissues, causing acute DNA damage to the endothelial cells of these tiny feeder capillaries. This sparked chronic, localized cellular proliferation and extensive swelling of the micro-vessel linings, completely blocking and destroying their microscopic channels (**Obliterative Endarteritis**). * **Ischemic Necrosis of the Media:** With the vasa vasorum permanently shut down, the thick middle layer of the main pelvic and thigh arteries—the **tunica media**—was starved of oxygen and nutrients. The smooth muscle cells and elastic fibers within the media underwent widespread ischemic death. The body attempted to patch these dead structural zones with weak, irregular, unyielding collagen scar tissue. Lacking healthy, elastic muscle fibers, the left iliac and femoral artery walls lost their structural elasticity, becoming fragile and unable to safely regulate hemodynamic pressure. ## 2. Hemodynamic Failure & Laplace’s Law The progression of this dead, calcified, and scarred arterial wall into a massive, expanding aneurysm is governed by the principles of vascular physics defined by **Laplace’s Law**: Where: * T = **Wall Tension** (the mechanical tearing force pulling the cells of the artery wall apart) * P = **Transmural Blood Pressure** (the outward force exerted by the blood against the wall) * r = **Radius** of the vessel (half of the internal diameter) * h = **Wall Thickness** ### The Vicious Expansion Loop 1. **The Pressure Variable (P):** The patient’s systemic blood pressure was elevated at 150/80\text{ mmHg}. This high pressure exerted a powerful outward force against the left external iliac and femoral artery segments. 2. **The Radius Variable (r):** Because the tunica media was structurally ruined by radiation-induced endarteritis obliterans, it could not snap back against this pressure. The artery wall gave way, and its radius began to expand. At his 4-month follow-up examination, the left femoral artery diameter had dilated to 1.8\text{ cm}. By the time of this acute admission, it had expanded to **2.0\text{ cm} on CT** and was measured as a **2.5\text{ cm} prominent pulsatile area** on physical examination. 3. **The Wall Thickness Variable (h):** As the vessel ballooned outward to more than double its normal size, its structural walls were stretched thinner and thinner. 4. **The Unstoppable Mathematical Feedback:** According to the equation, doubling the radius (r) while thinning the wall (h) causes the internal wall tension (T) to rise exponentially, even if the systemic blood pressure stays completely steady. This created a progressive feedback loop: dilation increased wall tension, which forced further dilation, which further increased tension. Eventually, the mechanical tearing force (T) outstripped the physical breaking strength of the brittle, calcified tissue layers. ## 3. Pathophysiology of the Chronic Contained Leak When the structural limits of Laplace's Law were exceeded, the rigid, brittle calcium plaques inside the artery wall cracked under the stress. This did not result in an immediate, fatal internal hemorrhage due to localized mechanical containment. ``` [ CROSS-SECTION OF THE LEFT GROIN VASCULAR CRISIS ] Outward High-Pressure Blood (150 mmHg) │ ▼ [ Cracks / Fissures in Brittle Calcified Plaque Shell ] │ ▼ [ Plasma & Red Blood Cells Seep Outside the True Vessel ] │ ▼ +-----------------------------------------------------------------------+ | THE COLLATERAL RADIATION SCAR WRAPPER | | Dense, Stiff Peri-Arterial Fibrosis (Poorly Defined Tissue Density) | +-----------------------------------------------------------------------+ │ ▼ Mechanical Tamponade (External Pressure Equalization) │ ▼ Hemorrhage Slowed to a Microscopic, Intermittent Weep (Contained) ``` * **The External Scar Wrapper:** The same historic radiation that destroyed the vasa vasorum also caused extensive collateral damage to the surrounding peri-arterial fat planes. It triggered chronic fat necrosis and replaced soft, dark adipose tissue with a dense, unyielding sleeve of collagen scar tissue (**peri-arterial fibrosis**). * **The Mechanical Tamponade Effect:** As high-pressure blood seeped out through the microscopic cracks in the calcified artery wall, it ran into this rigid fibrotic scar barrier. The scar tissue acted as a natural external pressure cuff, trapping the escaped blood and forcing the pressure in the extracellular space to quickly equal the pressure inside the artery. This pressure equalization created a **tamponade effect**, slowing the bleeding to a minimal, intermittent weep. * **The Imaging Footprint:** On his abdominal and pelvic CT scan, this complex matrix of dense radiation scars, localized inflammatory fluid, and slow-leaking, thrombosed blood appears as the **"poorly defined soft-tissue density surrounding the left external iliac artery... extending into the common femoral, superficial femoral, and profunda femoris arteries."** Because the blood slowly leaked along the irregular borders of the scarred tissue planes, the radiologist noted the edges of this mass were hazy and "poorly defined." This continuous trail of abnormal density represents the physical path of a chronic, contained leak tracking along his left lower pelvic and leg anatomy. ## 4. Unilateral Pitting Edema & Compression Neuropathy As the aneurysm expanded and blood leaked into the surrounding tissues, it created a localized space-occupying mass effect within the tight anatomical boundaries of the left groin, leading to clear peripheral symptoms. ### Unilateral Grade 3 (+++) Pitting Edema The physical exam noted **+++ pitting edema** restricted exclusively to the left lower extremity, while the right leg remained entirely normal. * **The Mechanism:** The femoral artery and femoral vein run side-by-side within the tight confines of the femoral sheath. The massive 2.5\text{ cm} aneurysmal mass, coupled with the dense surrounding soft-tissue density, physically pressed against the thin-walled, low-pressure **left common femoral vein**, flattening its channel. * **Hydrostatic Intravascular Backup:** This mechanical compression blocked the return of venous blood from the left leg back to the heart. Blood backed up downstream, causing a severe rise in hydrostatic pressure inside the capillaries of the left calf and foot. * **The Pitting Manifestation:** This high hydrostatic pressure forced vast amounts of water and electrolytes out of the capillaries and into the interstitial tissue spaces. When the clinician pressed a thumb into the swollen left leg, this displaced fluid left a deep, persistent 6\text{ mm} indentation that took 1 to 2 minutes to disappear, fulfilling the definition of **Grade 3 (+++) pitting edema**. Because the right leg was normal, systemic causes of edema (such as right-sided heart failure, liver cirrhosis, or kidney failure, which cause equal fluid buildup in both legs) were excluded, confirming a localized mechanical blockage in the left groin. ### Radiating Groin-to-Leg Pain The patient presented with severe pain in the left groin that radiated down the entire length of his left leg, while his comprehensive neurological examination remained completely negative. * **The Mechanism:** The **femoral nerve** passes immediately lateral to the femoral artery within the iliopectineal fossa. The expanding aneurysm and the contained blood leak pressed directly against this nerve trunk. This mechanical pressure irritated the sensory nerve fibers, triggering nociceptive pain signals that the brain mapped along the nerve's anatomical path down the front of the thigh and leg (**compression neuropathy**). * **Neuropraxia without Axon Death:** The normal neurological exam (intact reflexes, intact motor function, no paralysis) proves that while the nerve was mechanically irritated (**neuropraxia**), the pressure had not yet cut off its microscopic blood supply (*vasa nervorum*). There was no permanent nerve death or axonal degeneration, indicating that the radiating pain should resolve once the pressure from the aneurysm is surgically corrected. ## 5. The Acute-on-Chronic Ischemic Crisis The patient’s transition from a long-standing, stable vascular condition into an acute surgical crisis is rooted in the altered fluid dynamics inside his diseased lower leg vessels. ``` [ THE OUTFLOW THROMBOEMBOLIC CASCADE ] Normal Flow -> Laminar, High Velocity │ ▼ [ LEFT POPLITEAL ANEURYSM (Behind Knee joint) ] │ ▼ Sluggish, Swirling Eddies & Turbulent Whirlpools │ ▼ Fulfills Virchow's Triad -> Layered Mural Thrombi Form Along Wall │ ▼ Mechanical Shear -> Fragment of Blood Clot Breaks Free (Embolus) │ ▼ Washes Distally Down the Left Leg Arterial Tree │ ▼ Physically Wedges into the Small Runoff Arteries of the Foot │ ▼ [ Total Sudden Blockage -> ABSENT LEFT DORSALIS PEDIS PULSE ] │ ▼ ACUTE-ON-CHRONIC LIMB ISCHEMIA ``` * **Virchow's Triad in Aneurysms:** In a healthy artery, blood flows in a smooth, high-velocity parallel path (**laminar flow**). Inside both the diffuse groin aneurysm and the **focal aneurysm in the left popliteal artery** (located behind the knee joint just above the tibial plateau), the expanded diameter caused blood to swirl in sluggish, turbulent whirlpools. This localized stasis, combined with the rough, calcified, exposed endothelial lining, fulfilled Virchow’s Triad, causing layered sheets of blood clots (**mural thrombi**) to form along the inside walls of the aneurysms. * **The Thromboembolic Trigger:** Under a sudden spike in mechanical pressure or physical leg movement, a piece of this fragile mural clot broke off from the popliteal aneurysm pocket, becoming a mobile **thromboembolus**. This clot washed distally down the leg with the arterial stream until the vessels narrowed near the ankle. * **The Acute Mechanical Blockage:** The embolus wedged into the small runoff artery feeding the top of the foot. This sudden blockage caused a rapid drop in tissue perfusion, manifesting on physical exam as an **absent left dorsalis pedis pulse**. Because his left popliteal and posterior tibial pulses remained palpable, the exam isolated the block to the very end of the arterial line. * **Acute-on-Chronic Ischemia:** This sudden cutoff of oxygenated blood left the tissues of his foot starving for oxygen. Because the patient had suffered from *chronic* PAD for years, his body had grown tiny, alternative bypass vessels over time (**collateral circulation**). These collaterals provided a minimal baseline of blood flow that prevented instant tissue death (necrosis), buying the clinical team a narrow window of time. However, the sudden embolic blockage pushed the tissues past their metabolic threshold, causing severe, acute ischemia that required immediate surgical removal of the clot. ## 6. Detailed Systemic Organ & Imaging Compendium Beyond the left lower extremity vascular crisis, the patient’s diagnostic workup revealed several long-standing physiological changes across multiple organ systems. ### A. The Cardiovascular System & The Right Bundle Branch Block (RBBB) The patient’s laboratory panel—including serum electrolytes, calcium, phosphorus, glucose, coagulation factors (PT/PTT), and markers of kidney function (BUN/creatinine)—was normal. However, his electrocardiogram (ECG) revealed a **Right Bundle Branch Block (RBBB)** with a stable, normal sinus rhythm at a rate of 80 beats per minute. * **Pathophysiology of the Conduction Block:** The heart's electrical wiring splits into the Left Bundle Branch and the Right Bundle Branch to deliver the signal to squeeze the ventricles. An RBBB means the electrical highway leading to the right ventricle is physically scarred or blocked. Because the main highway is down, the electrical signal must detour through ordinary muscle fibers to reach the right ventricle. This detour takes longer, presenting on his ECG as a widened QRS complex with a classic delayed electrical wave in the right-sided chest leads. * **The Pulmonary Connection:** This structural block is directly linked to his **30-year cigarette and 32-year pipe-smoking history**, which caused **chronic bronchitis**. Chronic airway inflammation and mucus plugging make the lungs stiffer and harder to pump blood through. This increases the resistance against the right side of the heart (**pulmonary hypertension**). Over decades, this constant mechanical workload caused mild stretching and microscopic scarring of the right ventricular wall, easily interrupting the delicate fibers of the right bundle branch. * **Why the Rhythm Remained Normal at 80 bpm:** A bundle branch block is a **conduction** defect, not a **pacemaker** defect. The heart’s primary pacemaker—the Sinoatrial (SA) node—is healthy, firing at a steady rate of 80 beats per minute. The electrical signal originates normally and travels down the left bundle branch without delay, ensuring the left ventricle squeezes on time to maintain a steady, functional pulse. The right ventricle simply receives the signal a fraction of a second later, making this a stable, chronic change that did not cause his current leg pain. ### B. The Respiratory System & Asbestos Exposure His chest radiograph revealed **bilateral calcific pleural plaques**, but noted that the underlying lung tissue (**parenchyma**) was entirely clear, and the heart and mediastinal shadows were normal. * **Pathophysiology of Pleural Plaques:** These calcified plaques are the physical footprint of his past occupation as a **shipyard pipe fitter**. In the mid-to-late 20th century, shipyard piping was heavily insulated with **asbestos**. The patient routinely inhaled these microscopic, needle-like asbestos fibers. Due to their size and shape, the fibers bypassed the lung's clearing mechanisms and migrated across the lung tissue into the parietal pleura (the outer lining of the chest cavity). * **Dystrophic Mineralization:** The human body cannot break down asbestos fibers. Macrophages repeatedly attempted to engulf them, releasing pro-inflammatory cytokines and growth factors that sparked a slow, decades-long inflammatory response. Over 30 to 50 years, this chronic irritation led to dense collagen scarring and localized **dystrophic calcification** along the chest wall. Because these plaques were noted as **"unchanged from those seen on earlier examinations,"** they represent stable, historic asbestos exposure rather than an active cancer like mesothelioma. Furthermore, because his lung parenchyma was clear, he has avoided diffuse lung tissue scarring (asbestosis), and his respiratory symptoms remain driven by tobacco-related chronic bronchitis. ### C. The Musculoskeletal System & DISH His spinal imaging noted **"bridging ossification of the thoracic vertebral bodies, suggestive of Diffuse Idiopathic Skeletal Hyperostosis (DISH),"** but showed that the remaining bones were normal. * **Pathophysiology of DISH:** DISH (also known as Forestier’s disease) is a non-inflammatory, degenerative systemic condition common in older men where the ligaments running along the spine slowly turn into bone (**ossify**). In this patient, the anterior longitudinal ligament running down the front of his spine ossified, forming large bone spurs that grew to bridge the gaps between neighboring thoracic vertebrae like melted candle wax. * **Clinical Significance:** This condition explained any chronic stiffness in his spine, but its presence confirmed that his spinal changes were entirely benign. In a patient with a history of prostate cancer, spinal variations can indicate bone metastases; DISH confirmed there were **no metastatic lesions in his spine**, and his bones were structurally clear. ### D. The Renal System & Embryonic Vascular Variations Abdominal imaging and angiography identified multiple fluid-filled **right renal cysts** (including a large 10\text{ cm} cyst at the upper pole) and revealed a **double right renal artery** alongside a standard **single left renal artery**. * **Pathophysiology of Simple Renal Cysts:** These cysts are fluid-filled pockets that develop from microscopic outpouchings of the renal tubules as a person ages. Over time, these pockets detach from the tubule and fill with clear fluid. Despite the large 10\text{ cm} size of the upper pole cyst, it is purely a fluid collection rather than solid tissue, meaning it is non-cancerous. Because his BUN and creatinine levels were normal, these cysts have not damaged his overall kidney function. * **Anatomy of the Double Renal Artery:** During early fetal development, the kidneys initially form down in the pelvis and ascend to the upper abdomen, receiving temporary blood vessels from local arteries along the way. Normally, these lower embryonic vessels disappear as the kidney hitches to its final, single renal artery high up in the abdomen. When an early embryonic vessel fails to regress, it persists as an **accessory (double) renal artery**. * **Vascular Patentcy:** The angiogram explicitly noted that his single left renal artery and both right renal arteries were **patent** (completely open, with no narrow segments). This ruled out *renovascular hypertension* (where a narrowed kidney artery triggers an overproduction of renin to drive up systemic blood pressure). His high blood pressure was instead driven by essential, systemic atherosclerosis. ## 7. Complete Onco-Pathological Remission Profile A key element of this case is that despite the patient's extensive history of aggressive cancers, **both of his primary malignancies were in complete remission**, meaning his groin mass and leg swelling were entirely vascular. ### Resected Colon Carcinoma Ten years prior, the patient underwent a **left hemicolectomy** to resect a colon tumor. On this admission, his abdominal exam was clear, his serum amylase was normal, and his stool specimen returned a **negative test for occult blood**. * **Pathophysiology:** Malignant colon tumors are highly vascularized but structurally fragile, consistently shedding microscopic amounts of blood into the stool. The negative chemical occult blood test proves that his intestinal lining is intact, and there are no bleeding or ulcerative tumor recurrences at his old surgical site. ### Quiescent Prostate Adenocarcinoma Seventeen months before this admission, the patient faced a severe prostate cancer recurrence marked by a palpable nodule on rectal exam and a massive serum Prostate-Specific Antigen (PSA) spike to **94.5\ \mu\text{g/L}** (normal range is 0.5 to 3.9\ \mu\text{g/L}). He was treated with a transurethral resection of the prostate (TURP) and a surgical **bilateral orchiectomy**. On this admission, his rectal exam showed a **flat prostatic bed**, and his follow-up PSA and Prostatic Acid Phosphatase (PAP) levels were completely normal. * **The Mechanism of Castration Success:** Prostate cancer cells rely heavily on circulating androgens—specifically testosterone—to activate their growth pathways and produce tumor markers like PSA and PAP. A bilateral orchiectomy removes both testicles, permanently eliminating 95\% of systemic testosterone production. Starved of this hormone, the remaining prostate cancer cells underwent widespread apoptosis (programmed cell death). * **Pathophysiology of the Flat Bed and Normal Labs:** Because the cancer cells died and the tumor mass collapsed, the prostatic bed felt entirely smooth and **flat** against the rectal wall. With no active cancer tissue left to break through local blood vessel barriers, no tumor markers spilled into his systemic circulation. This kept his PSA and PAP levels perfectly normal, confirming his cancer was in complete biochemical and anatomical remission. ## 8. Final Definitive Synthesis The **"diagnostic procedure"** performed at the end of his workup was a **Diagnostic Catheter Angiography (with Fluoroscopy)**. A vascular specialist advanced a flexible catheter into his aorta to deliver contrast dye under real-time X-ray imaging. This procedure mapped out his vascular anatomy and confirmed that his presentation was an acute vascular emergency. The final clinical picture shows a patient whose lifestyle factors (smoking, hypertension) and past medical treatments (high-dose pelvic radiation) combined over a ten-year period to destroy the structural matrix of his left femoral artery wall. This structural failure resulted in a slow-leaking, 2.5\text{ cm} groin aneurysm that compressed his femoral vein, causing severe **Grade 3 (+++) pitting edema** and pressing against his femoral nerve to cause radiating leg pain. The acute crisis was triggered when turbulent blood flow inside a separate **focal popliteal aneurysm** behind his knee formed a blood clot that broke free and traveled down his leg. This embolus mechanically wedged into the small runoff arteries of his foot, causing an **absent left dorsalis pedis pulse** and throwing him into **acute-on-chronic limb ischemia**. This complex, multi-layered vascular failure required immediate surgical intervention—including an emergency embolectomy to clear the foot blockage, excision of the leaking groin aneurysm, and bypass grafting to save his lower leg. 1. Now can u me a flow chart and image explaining the pathophysiology of the chronic contained leak. 2. Generate me image explaining the unilateral pitting edema and compression neuropathy
A detailed medical pathophysiology flowchart diagram showing the chronic contained leak mechanism in a diseased femoral artery. The diagram is a vertical cross-sectional and flow chart hybrid illustration. At the top, show a cross-section of a diseased artery wall with three labeled layers: inner lumen with blood at 150 mmHg, a middle layer showing cracked brittle calcified atherosclerotic plaques with fissures and fracture lines, and an outer layer of dense radiation-induced peri-arterial fibrosis (collagen scar tissue shown as dense fibrous bands). Arrows show high-pressure blood seeping through the cracks in the calcified plaque shell into the surrounding tissue. Below the cross-section, a flowchart with labeled boxes connected by arrows: Box 1: "Atherosclerotic Calcified Plaque Shell - Brittle, Rigid, Crystalline Hydroxyapatite" → Box 2: "Laplace's Law Failure - Rising Wall Tension Exceeds Tensile Strength" → Box 3: "Microfractures in Calcified Shell - Cracks Open Under 150 mmHg Pressure" → Box 4: "Blood Plasma & RBCs Seep Through Cracks Into Peri-Arterial Space" → Box 5: "Radiation-Induced Peri-Arterial Fibrosis Acts as External Scar Wrapper" → Box 6: "Tamponade Effect - Extravascular Pressure Equalizes Intravascular Pressure" → Box 7: "Hemorrhage Slowed to Intermittent Microscopic Weep - Contained Leak" → Final Box: "CT Finding: Poorly Defined Soft-Tissue Density Surrounding Left External Iliac Artery". Use medical illustration style, dark blue and red color scheme for blood vessels, orange-yellow for calcified plaques, gray-white for fibrotic scar tissue, clear sans-serif labels, clean clinical diagram aesthetic.
A detailed medical anatomy diagram showing the left groin region illustrating two simultaneous mechanisms: unilateral pitting edema and femoral nerve compression neuropathy. The illustration shows a frontal anatomical view of the left femoral triangle with labeled structures. In the center, a large 2.5 cm pulsatile aneurysmal mass with surrounding soft tissue density (radiation fibrosis) is shown compressing two adjacent structures. On the left side of the aneurysm: the left common femoral vein is shown being flattened and compressed, with an arrow showing upstream venous blood backup, and a downstream diagram showing the left leg with fluid accumulating in calf and foot tissue labeled "Grade 3 Pitting Edema - 6mm pit, 1-2 min rebound" with blue wavy lines indicating interstitial fluid accumulation in the leg. The right leg is shown normal for comparison. On the right side of the aneurysm: the femoral nerve is shown being mechanically compressed by the expanding mass, with nociceptive pain signals (shown as lightning bolt symbols) radiating down the anterior thigh and leg, labeled "Compression Neuropathy - Neuropraxia without Axonal Death" and "Normal reflexes, normal motor function preserved". A small inset shows the femoral sheath anatomy with femoral nerve (lateral), femoral artery (center), and femoral vein (medial) - NAVEL mnemonic arrangement. Color scheme: red for arteries, blue for veins, yellow for nerves, green for the aneurysmal mass, purple for radiation fibrosis. Medical textbook illustration style, clean labeled anatomy diagram.
# Pathophysiological Compendium & Complete Case Analysis This comprehensive analysis systematically connects this patient's lifetime exposures, past oncology treatments, genetic anatomy variants, and hemodynamic variables to construct a unified pathophysiological explanation of his entire clinical presentation. ## 1. Longitudinal Timeline & The "Dual-Hit" Vascular Injury The severe Peripheral Arterial Disease (PAD) presenting as a diffuse, leaking groin aneurysm and a downstream acute-on-chronic embolic crisis is the product of a distinct "dual-hit" pathological process. ``` +-------------------------------------------------------------------------+ | HIT 1 | | 62-Pack-Year Tobacco Toxins + Chronic Mechanical Hypertension (150mmHg)| +-------------------------------------------------------------------------+ │ ▼ Chronic Endothelial Shear Injury │ ▼ Subendothelial LDL Infiltration & Macrophage Activation │ ▼ Foam Cell & Fatty Streak Formation │ ▼ Smooth Muscle Proliferation & Fibrous Cap │ ▼ Atherosclerotic Plaque Calcification (Crescentic Shells on CT) │ │ +--------------------------------───┴─────────────────────────────────────+ | HIT 2 | | Historic High-Dose Pelvic Radiotherapy (4500 cGy Pelvis / 6900 cGy) | +-------------------------------------------------------------------------+ │ ▼ Obliterative Endarteritis of the Microscopic Vasa Vasorum │ ▼ Total Microvascular Occlusion -> Hypoxic Starvation of Vessel Wall │ ▼ Coagulative Ischemic Necrosis of Tunica Media │ ▼ Permanent Structural Erasure of Elastic and Muscular Fibers │ ▼ Brittle, Rigid, Non-Compliant, Unstable Inflow Network (PAD) ``` ### Hit 1: Lifestyle & Metabolic Atherogenesis For 30 years, the patient smoked one pack of cigarettes daily, followed by 32 years of pipe-smoking, accumulating a **62-pack-year history of tobacco exposure**. * **Endothelial Shearing:** Inhaled nicotine and polycyclic aromatic hydrocarbons act as potent circulating chemical toxins. These compounds directly sheared the delicate inner endothelial monolayer of his large and medium-sized arteries. This chemical trauma was compounded by chronic, poorly controlled **hypertension** (150/80\text{ mmHg}), which applied continuous, raw mechanical stress to the vessel walls. * **The Lipid Cascade:** Endothelial injury breached the blood-artery barrier, allowing circulating Low-Density Lipoprotein (LDL) cholesterol to infiltrate the subendothelial space of the tunica intima. These lipids underwent chemical oxidation, transforming into highly immunogenic molecules. * **Foam Cell and Plaque Formation:** Circulating monocytes migrated into the vessel wall, differentiating into macrophages to engulf the oxidized LDL. These cells became bloated, fat-filled **foam cells**, forming foundational fatty streaks. Over decades, smooth muscle cells migrated from the media to the intima, secreting collagen to lock this fatty core beneath a fibrous cap, establishing advanced atherosclerotic plaques. * **Dystrophic Calcification:** As these plaques aged, cellular death (necrosis) occurred within their cores. Intracellular calcium pumps failed, causing a massive release of calcium ions into the necrotic tissue debris. These ions bound to negatively charged phosphate groups on broken cell membrane fragments, precipitating as **calcium phosphate** and reorganizing into rock-hard **hydroxyapatite crystals**. On his pelvic CT scan, this process is visible as the **"scattered crescentic calcifications present adjacent to the arterial lumen."** These rigid, crescent-shaped shells are the calcified structural outlines of his underlying atherosclerotic plaques. ### Hit 2: Iatrogenic Radiation-Induced Vascular Obliteration Ten years prior to this admission, the patient received a massive dose of ionizing radiation to treat an aggressive stage \text{B}_1 adenocarcinoma of the prostate gland: **4500 cGy to the wider pelvis**, followed by a localized booster dose of **6900 cGy straight to the prostatic bed**, delivered via a 4-MeV linear accelerator. * **Endarteritis Obliterans:** Large, thick conduits like the external iliac and common femoral arteries cannot absorb oxygen directly from the high-velocity blood rushing through their main channels. Instead, they rely on a network of microscopic capillaries looping through their outer walls called the **Vasa Vasorum** ("the vessels of the vessels"). The high-energy radiation beams blasted through these groin tissues, causing acute DNA damage to the endothelial cells of these tiny feeder capillaries. This sparked chronic, localized cellular proliferation and extensive swelling of the micro-vessel linings, completely blocking and destroying their microscopic channels (**Obliterative Endarteritis**). * **Ischemic Necrosis of the Media:** With the vasa vasorum permanently shut down, the thick middle layer of the main pelvic and thigh arteries—the **tunica media**—was starved of oxygen and nutrients. The smooth muscle cells and elastic fibers within the media underwent widespread ischemic death. The body attempted to patch these dead structural zones with weak, irregular, unyielding collagen scar tissue. Lacking healthy, elastic muscle fibers, the left iliac and femoral artery walls lost their structural elasticity, becoming fragile and unable to safely regulate hemodynamic pressure. ## 2. Hemodynamic Failure & Laplace’s Law The progression of this dead, calcified, and scarred arterial wall into a massive, expanding aneurysm is governed by the principles of vascular physics defined by **Laplace’s Law**: Where: * T = **Wall Tension** (the mechanical tearing force pulling the cells of the artery wall apart) * P = **Transmural Blood Pressure** (the outward force exerted by the blood against the wall) * r = **Radius** of the vessel (half of the internal diameter) * h = **Wall Thickness** ### The Vicious Expansion Loop 1. **The Pressure Variable (P):** The patient’s systemic blood pressure was elevated at 150/80\text{ mmHg}. This high pressure exerted a powerful outward force against the left external iliac and femoral artery segments. 2. **The Radius Variable (r):** Because the tunica media was structurally ruined by radiation-induced endarteritis obliterans, it could not snap back against this pressure. The artery wall gave way, and its radius began to expand. At his 4-month follow-up examination, the left femoral artery diameter had dilated to 1.8\text{ cm}. By the time of this acute admission, it had expanded to **2.0\text{ cm} on CT** and was measured as a **2.5\text{ cm} prominent pulsatile area** on physical examination. 3. **The Wall Thickness Variable (h):** As the vessel ballooned outward to more than double its normal size, its structural walls were stretched thinner and thinner. 4. **The Unstoppable Mathematical Feedback:** According to the equation, doubling the radius (r) while thinning the wall (h) causes the internal wall tension (T) to rise exponentially, even if the systemic blood pressure stays completely steady. This created a progressive feedback loop: dilation increased wall tension, which forced further dilation, which further increased tension. Eventually, the mechanical tearing force (T) outstripped the physical breaking strength of the brittle, calcified tissue layers. ## 3. Pathophysiology of the Chronic Contained Leak When the structural limits of Laplace's Law were exceeded, the rigid, brittle calcium plaques inside the artery wall cracked under the stress. This did not result in an immediate, fatal internal hemorrhage due to localized mechanical containment. ``` [ CROSS-SECTION OF THE LEFT GROIN VASCULAR CRISIS ] Outward High-Pressure Blood (150 mmHg) │ ▼ [ Cracks / Fissures in Brittle Calcified Plaque Shell ] │ ▼ [ Plasma & Red Blood Cells Seep Outside the True Vessel ] │ ▼ +-----------------------------------------------------------------------+ | THE COLLATERAL RADIATION SCAR WRAPPER | | Dense, Stiff Peri-Arterial Fibrosis (Poorly Defined Tissue Density) | +-----------------------------------------------------------------------+ │ ▼ Mechanical Tamponade (External Pressure Equalization) │ ▼ Hemorrhage Slowed to a Microscopic, Intermittent Weep (Contained) ``` * **The External Scar Wrapper:** The same historic radiation that destroyed the vasa vasorum also caused extensive collateral damage to the surrounding peri-arterial fat planes. It triggered chronic fat necrosis and replaced soft, dark adipose tissue with a dense, unyielding sleeve of collagen scar tissue (**peri-arterial fibrosis**). * **The Mechanical Tamponade Effect:** As high-pressure blood seeped out through the microscopic cracks in the calcified artery wall, it ran into this rigid fibrotic scar barrier. The scar tissue acted as a natural external pressure cuff, trapping the escaped blood and forcing the pressure in the extracellular space to quickly equal the pressure inside the artery. This pressure equalization created a **tamponade effect**, slowing the bleeding to a minimal, intermittent weep. * **The Imaging Footprint:** On his abdominal and pelvic CT scan, this complex matrix of dense radiation scars, localized inflammatory fluid, and slow-leaking, thrombosed blood appears as the **"poorly defined soft-tissue density surrounding the left external iliac artery... extending into the common femoral, superficial femoral, and profunda femoris arteries."** Because the blood slowly leaked along the irregular borders of the scarred tissue planes, the radiologist noted the edges of this mass were hazy and "poorly defined." This continuous trail of abnormal density represents the physical path of a chronic, contained leak tracking along his left lower pelvic and leg anatomy. ## 4. Unilateral Pitting Edema & Compression Neuropathy As the aneurysm expanded and blood leaked into the surrounding tissues, it created a localized space-occupying mass effect within the tight anatomical boundaries of the left groin, leading to clear peripheral symptoms. ### Unilateral Grade 3 (+++) Pitting Edema The physical exam noted **+++ pitting edema** restricted exclusively to the left lower extremity, while the right leg remained entirely normal. * **The Mechanism:** The femoral artery and femoral vein run side-by-side within the tight confines of the femoral sheath. The massive 2.5\text{ cm} aneurysmal mass, coupled with the dense surrounding soft-tissue density, physically pressed against the thin-walled, low-pressure **left common femoral vein**, flattening its channel. * **Hydrostatic Intravascular Backup:** This mechanical compression blocked the return of venous blood from the left leg back to the heart. Blood backed up downstream, causing a severe rise in hydrostatic pressure inside the capillaries of the left calf and foot. * **The Pitting Manifestation:** This high hydrostatic pressure forced vast amounts of water and electrolytes out of the capillaries and into the interstitial tissue spaces. When the clinician pressed a thumb into the swollen left leg, this displaced fluid left a deep, persistent 6\text{ mm} indentation that took 1 to 2 minutes to disappear, fulfilling the definition of **Grade 3 (+++) pitting edema**. Because the right leg was normal, systemic causes of edema (such as right-sided heart failure, liver cirrhosis, or kidney failure, which cause equal fluid buildup in both legs) were excluded, confirming a localized mechanical blockage in the left groin. ### Radiating Groin-to-Leg Pain The patient presented with severe pain in the left groin that radiated down the entire length of his left leg, while his comprehensive neurological examination remained completely negative. * **The Mechanism:** The **femoral nerve** passes immediately lateral to the femoral artery within the iliopectineal fossa. The expanding aneurysm and the contained blood leak pressed directly against this nerve trunk. This mechanical pressure irritated the sensory nerve fibers, triggering nociceptive pain signals that the brain mapped along the nerve's anatomical path down the front of the thigh and leg (**compression neuropathy**). * **Neuropraxia without Axon Death:** The normal neurological exam (intact reflexes, intact motor function, no paralysis) proves that while the nerve was mechanically irritated (**neuropraxia**), the pressure had not yet cut off its microscopic blood supply (*vasa nervorum*). There was no permanent nerve death or axonal degeneration, indicating that the radiating pain should resolve once the pressure from the aneurysm is surgically corrected. ## 5. The Acute-on-Chronic Ischemic Crisis The patient’s transition from a long-standing, stable vascular condition into an acute surgical crisis is rooted in the altered fluid dynamics inside his diseased lower leg vessels. ``` [ THE OUTFLOW THROMBOEMBOLIC CASCADE ] Normal Flow -> Laminar, High Velocity │ ▼ [ LEFT POPLITEAL ANEURYSM (Behind Knee joint) ] │ ▼ Sluggish, Swirling Eddies & Turbulent Whirlpools │ ▼ Fulfills Virchow's Triad -> Layered Mural Thrombi Form Along Wall │ ▼ Mechanical Shear -> Fragment of Blood Clot Breaks Free (Embolus) │ ▼ Washes Distally Down the Left Leg Arterial Tree │ ▼ Physically Wedges into the Small Runoff Arteries of the Foot │ ▼ [ Total Sudden Blockage -> ABSENT LEFT DORSALIS PEDIS PULSE ] │ ▼ ACUTE-ON-CHRONIC LIMB ISCHEMIA ``` * **Virchow's Triad in Aneurysms:** In a healthy artery, blood flows in a smooth, high-velocity parallel path (**laminar flow**). Inside both the diffuse groin aneurysm and the **focal aneurysm in the left popliteal artery** (located behind the knee joint just above the tibial plateau), the expanded diameter caused blood to swirl in sluggish, turbulent whirlpools. This localized stasis, combined with the rough, calcified, exposed endothelial lining, fulfilled Virchow’s Triad, causing layered sheets of blood clots (**mural thrombi**) to form along the inside walls of the aneurysms. * **The Thromboembolic Trigger:** Under a sudden spike in mechanical pressure or physical leg movement, a piece of this fragile mural clot broke off from the popliteal aneurysm pocket, becoming a mobile **thromboembolus**. This clot washed distally down the leg with the arterial stream until the vessels narrowed near the ankle. * **The Acute Mechanical Blockage:** The embolus wedged into the small runoff artery feeding the top of the foot. This sudden blockage caused a rapid drop in tissue perfusion, manifesting on physical exam as an **absent left dorsalis pedis pulse**. Because his left popliteal and posterior tibial pulses remained palpable, the exam isolated the block to the very end of the arterial line. * **Acute-on-Chronic Ischemia:** This sudden cutoff of oxygenated blood left the tissues of his foot starving for oxygen. Because the patient had suffered from *chronic* PAD for years, his body had grown tiny, alternative bypass vessels over time (**collateral circulation**). These collaterals provided a minimal baseline of blood flow that prevented instant tissue death (necrosis), buying the clinical team a narrow window of time. However, the sudden embolic blockage pushed the tissues past their metabolic threshold, causing severe, acute ischemia that required immediate surgical removal of the clot. ## 6. Detailed Systemic Organ & Imaging Compendium Beyond the left lower extremity vascular crisis, the patient’s diagnostic workup revealed several long-standing physiological changes across multiple organ systems. ### A. The Cardiovascular System & The Right Bundle Branch Block (RBBB) The patient’s laboratory panel—including serum electrolytes, calcium, phosphorus, glucose, coagulation factors (PT/PTT), and markers of kidney function (BUN/creatinine)—was normal. However, his electrocardiogram (ECG) revealed a **Right Bundle Branch Block (RBBB)** with a stable, normal sinus rhythm at a rate of 80 beats per minute. * **Pathophysiology of the Conduction Block:** The heart's electrical wiring splits into the Left Bundle Branch and the Right Bundle Branch to deliver the signal to squeeze the ventricles. An RBBB means the electrical highway leading to the right ventricle is physically scarred or blocked. Because the main highway is down, the electrical signal must detour through ordinary muscle fibers to reach the right ventricle. This detour takes longer, presenting on his ECG as a widened QRS complex with a classic delayed electrical wave in the right-sided chest leads. * **The Pulmonary Connection:** This structural block is directly linked to his **30-year cigarette and 32-year pipe-smoking history**, which caused **chronic bronchitis**. Chronic airway inflammation and mucus plugging make the lungs stiffer and harder to pump blood through. This increases the resistance against the right side of the heart (**pulmonary hypertension**). Over decades, this constant mechanical workload caused mild stretching and microscopic scarring of the right ventricular wall, easily interrupting the delicate fibers of the right bundle branch. * **Why the Rhythm Remained Normal at 80 bpm:** A bundle branch block is a **conduction** defect, not a **pacemaker** defect. The heart’s primary pacemaker—the Sinoatrial (SA) node—is healthy, firing at a steady rate of 80 beats per minute. The electrical signal originates normally and travels down the left bundle branch without delay, ensuring the left ventricle squeezes on time to maintain a steady, functional pulse. The right ventricle simply receives the signal a fraction of a second later, making this a stable, chronic change that did not cause his current leg pain. ### B. The Respiratory System & Asbestos Exposure His chest radiograph revealed **bilateral calcific pleural plaques**, but noted that the underlying lung tissue (**parenchyma**) was entirely clear, and the heart and mediastinal shadows were normal. * **Pathophysiology of Pleural Plaques:** These calcified plaques are the physical footprint of his past occupation as a **shipyard pipe fitter**. In the mid-to-late 20th century, shipyard piping was heavily insulated with **asbestos**. The patient routinely inhaled these microscopic, needle-like asbestos fibers. Due to their size and shape, the fibers bypassed the lung's clearing mechanisms and migrated across the lung tissue into the parietal pleura (the outer lining of the chest cavity). * **Dystrophic Mineralization:** The human body cannot break down asbestos fibers. Macrophages repeatedly attempted to engulf them, releasing pro-inflammatory cytokines and growth factors that sparked a slow, decades-long inflammatory response. Over 30 to 50 years, this chronic irritation led to dense collagen scarring and localized **dystrophic calcification** along the chest wall. Because these plaques were noted as **"unchanged from those seen on earlier examinations,"** they represent stable, historic asbestos exposure rather than an active cancer like mesothelioma. Furthermore, because his lung parenchyma was clear, he has avoided diffuse lung tissue scarring (asbestosis), and his respiratory symptoms remain driven by tobacco-related chronic bronchitis. ### C. The Musculoskeletal System & DISH His spinal imaging noted **"bridging ossification of the thoracic vertebral bodies, suggestive of Diffuse Idiopathic Skeletal Hyperostosis (DISH),"** but showed that the remaining bones were normal. * **Pathophysiology of DISH:** DISH (also known as Forestier’s disease) is a non-inflammatory, degenerative systemic condition common in older men where the ligaments running along the spine slowly turn into bone (**ossify**). In this patient, the anterior longitudinal ligament running down the front of his spine ossified, forming large bone spurs that grew to bridge the gaps between neighboring thoracic vertebrae like melted candle wax. * **Clinical Significance:** This condition explained any chronic stiffness in his spine, but its presence confirmed that his spinal changes were entirely benign. In a patient with a history of prostate cancer, spinal variations can indicate bone metastases; DISH confirmed there were **no metastatic lesions in his spine**, and his bones were structurally clear. ### D. The Renal System & Embryonic Vascular Variations Abdominal imaging and angiography identified multiple fluid-filled **right renal cysts** (including a large 10\text{ cm} cyst at the upper pole) and revealed a **double right renal artery** alongside a standard **single left renal artery**. * **Pathophysiology of Simple Renal Cysts:** These cysts are fluid-filled pockets that develop from microscopic outpouchings of the renal tubules as a person ages. Over time, these pockets detach from the tubule and fill with clear fluid. Despite the large 10\text{ cm} size of the upper pole cyst, it is purely a fluid collection rather than solid tissue, meaning it is non-cancerous. Because his BUN and creatinine levels were normal, these cysts have not damaged his overall kidney function. * **Anatomy of the Double Renal Artery:** During early fetal development, the kidneys initially form down in the pelvis and ascend to the upper abdomen, receiving temporary blood vessels from local arteries along the way. Normally, these lower embryonic vessels disappear as the kidney hitches to its final, single renal artery high up in the abdomen. When an early embryonic vessel fails to regress, it persists as an **accessory (double) renal artery**. * **Vascular Patentcy:** The angiogram explicitly noted that his single left renal artery and both right renal arteries were **patent** (completely open, with no narrow segments). This ruled out *renovascular hypertension* (where a narrowed kidney artery triggers an overproduction of renin to drive up systemic blood pressure). His high blood pressure was instead driven by essential, systemic atherosclerosis. ## 7. Complete Onco-Pathological Remission Profile A key element of this case is that despite the patient's extensive history of aggressive cancers, **both of his primary malignancies were in complete remission**, meaning his groin mass and leg swelling were entirely vascular. ### Resected Colon Carcinoma Ten years prior, the patient underwent a **left hemicolectomy** to resect a colon tumor. On this admission, his abdominal exam was clear, his serum amylase was normal, and his stool specimen returned a **negative test for occult blood**. * **Pathophysiology:** Malignant colon tumors are highly vascularized but structurally fragile, consistently shedding microscopic amounts of blood into the stool. The negative chemical occult blood test proves that his intestinal lining is intact, and there are no bleeding or ulcerative tumor recurrences at his old surgical site. ### Quiescent Prostate Adenocarcinoma Seventeen months before this admission, the patient faced a severe prostate cancer recurrence marked by a palpable nodule on rectal exam and a massive serum Prostate-Specific Antigen (PSA) spike to **94.5\ \mu\text{g/L}** (normal range is 0.5 to 3.9\ \mu\text{g/L}). He was treated with a transurethral resection of the prostate (TURP) and a surgical **bilateral orchiectomy**. On this admission, his rectal exam showed a **flat prostatic bed**, and his follow-up PSA and Prostatic Acid Phosphatase (PAP) levels were completely normal. * **The Mechanism of Castration Success:** Prostate cancer cells rely heavily on circulating androgens—specifically testosterone—to activate their growth pathways and produce tumor markers like PSA and PAP. A bilateral orchiectomy removes both testicles, permanently eliminating 95\% of systemic testosterone production. Starved of this hormone, the remaining prostate cancer cells underwent widespread apoptosis (programmed cell death). * **Pathophysiology of the Flat Bed and Normal Labs:** Because the cancer cells died and the tumor mass collapsed, the prostatic bed felt entirely smooth and **flat** against the rectal wall. With no active cancer tissue left to break through local blood vessel barriers, no tumor markers spilled into his systemic circulation. This kept his PSA and PAP levels perfectly normal, confirming his cancer was in complete biochemical and anatomical remission. ## 8. Final Definitive Synthesis The **"diagnostic procedure"** performed at the end of his workup was a **Diagnostic Catheter Angiography (with Fluoroscopy)**. A vascular specialist advanced a flexible catheter into his aorta to deliver contrast dye under real-time X-ray imaging. This procedure mapped out his vascular anatomy and confirmed that his presentation was an acute vascular emergency. The final clinical picture shows a patient whose lifestyle factors (smoking, hypertension) and past medical treatments (high-dose pelvic radiation) combined over a ten-year period to destroy the structural matrix of his left femoral artery wall. This structural failure resulted in a slow-leaking, 2.5\text{ cm} groin aneurysm that compressed his femoral vein, causing severe **Grade 3 (+++) pitting edema** and pressing against his femoral nerve to cause radiating leg pain. The acute crisis was triggered when turbulent blood flow inside a separate **focal popliteal aneurysm** behind his knee formed a blood clot that broke free and traveled down his leg. This embolus mechanically wedged into the small runoff arteries of his foot, causing an **absent left dorsalis pedis pulse** and throwing him into **acute-on-chronic limb ischemia**. This complex, multi-layered vascular failure required immediate surgical intervention—including an emergency embolectomy to clear the foot blockage, excision of the leaking groin aneurysm, and bypass grafting to save his lower leg. 1. Now can u me a flow chart and image explaining the pathophysiology of the chronic contained leak.
A detailed medical pathophysiology diagram combining a cross-sectional artery illustration at the top and a vertical flowchart below, showing the chronic contained leak mechanism in a diseased femoral artery. TOP SECTION - Cross-sectional anatomy diagram of the artery wall showing three concentric zones labeled: - CENTER: Arterial lumen with dark red blood, label "Blood at 150 mmHg Systolic Pressure" - MIDDLE RING: Thick layer showing cracked, shattered calcified atherosclerotic plaque with visible fracture lines and fissures, yellow-orange crystalline hydroxyapatite deposits, label "Brittle Calcified Plaque Shell - Fractured Under Laplace Wall Tension" - OUTER RING: Dense fibrous gray-white collagen scar tissue wrapping the outside of the artery, label "Radiation-Induced Peri-Arterial Fibrosis - Dense Collagen Scar Wrapper" Red arrows show blood escaping through cracks in the calcified layer but being stopped by the outer fibrosis ring. Small dots of red between the two outer layers labeled "Trapped Leaked Blood / Thrombosed Hematoma" BOTTOM SECTION - Clean vertical flowchart with 7 boxes connected by downward arrows: Box 1 (dark red): "Laplace's Law Feedback Loop - Wall Tension Exceeds Tensile Strength of Calcified Shell" Arrow down Box 2 (orange): "Microfractures Form in Brittle Hydroxyapatite Plaque Shell - Cracks Open at Points of Maximum Stress" Arrow down Box 3 (red): "High-Pressure Blood (150 mmHg) Forces Plasma and RBCs Through Fissures Into Peri-Arterial Space" Arrow down Box 4 (gray): "Blood Meets Rigid Radiation-Induced Peri-Arterial Fibrosis - Dense Collagen Scar Acts as External Pressure Cuff" Arrow down Box 5 (blue): "Tamponade Effect: Extravascular Pressure Rapidly Equalizes Intravascular Pressure - Hemorrhage Self-Arrests" Arrow down Box 6 (purple): "Slow Intermittent Microscopic Weep - Chronic Contained Leak Accumulates as Thrombosed Hematoma Over Weeks" Arrow down Box 7 (green): "CT Imaging Footprint: Poorly Defined Soft-Tissue Density Surrounding Left External Iliac Artery Extending to Common Femoral, SFA, and Profunda Femoris" Clean medical textbook illustration style, white background, professional sans-serif labels, high contrast colors
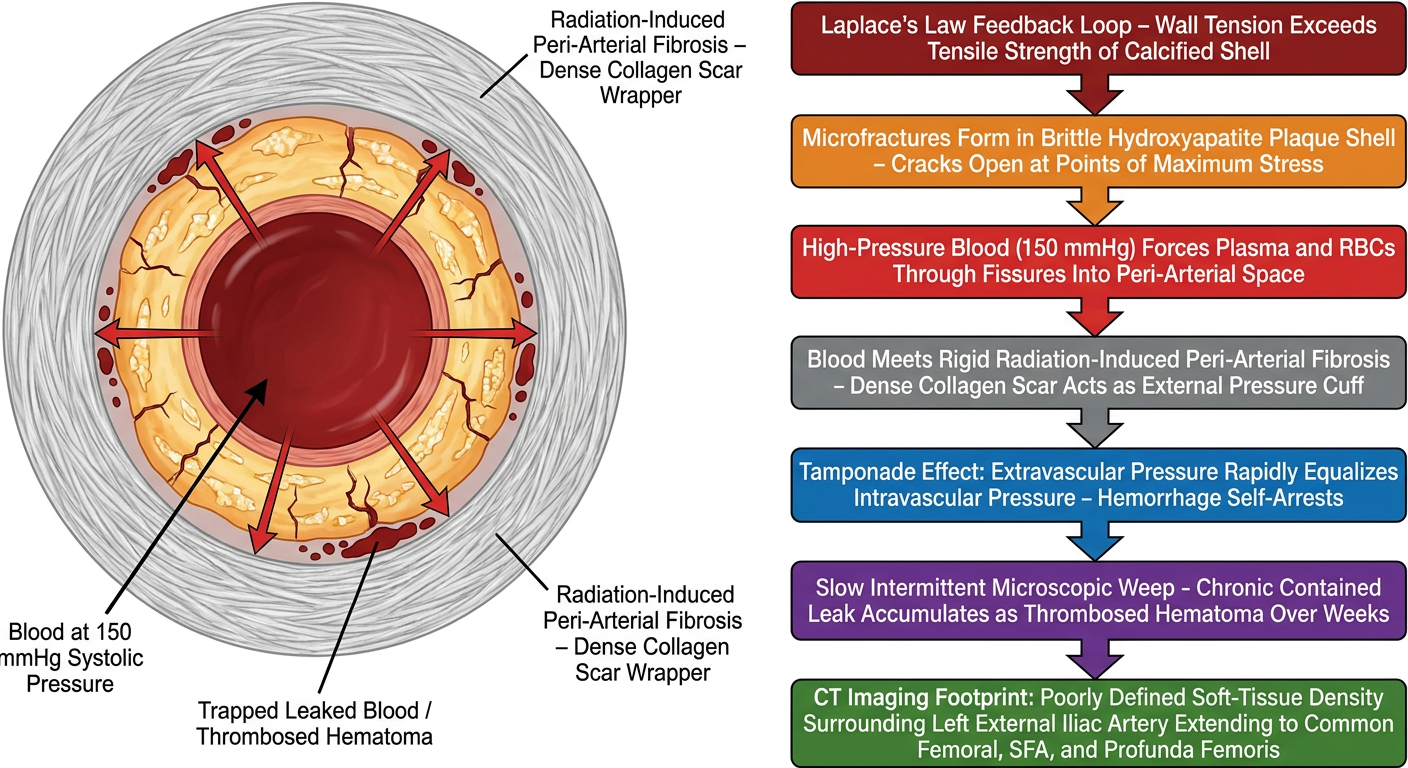
Reading the Diagram
- Center (dark red): Blood under 150 mmHg systolic pressure
- Middle ring (orange/yellow): The brittle, cracked hydroxyapatite calcified plaque shell - the structural layer that fractures under Laplace tension
- Outer ring (gray-white): The radiation-induced peri-arterial fibrosis acting as the involuntary pressure cuff that traps the escaping blood between the two layers
| Step | Event |
|---|---|
| 1 | Laplace's Law wall tension exceeds calcified shell tensile strength |
| 2 | Microfractures form in the brittle hydroxyapatite shell |
| 3 | Blood forces through fissures into peri-arterial space |
| 4 | Escaping blood meets the rigid radiation fibrosis barrier |
| 5 | Tamponade effect - extravascular pressure equalizes intravascular pressure |
| 6 | Bleeding self-arrests into a slow intermittent microscopic weep |
| 7 | CT footprint: poorly defined soft-tissue density along the left iliac/femoral axis |