Corrosive poisons
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive, high-quality content from multiple authoritative sources. Here is a complete, well-structured response on corrosive poisons:
Corrosive Poisons
Definition and Terminology
A caustic or corrosive is a dry or liquid chemical agent that is immediately dangerous to living tissue upon contact. In contrast, a poison exerts a systemic toxic effect that requires time to become apparent. Some agents are both corrosives and poisons. The word "corrosive" is derived from the Latin corrodere — "to gnaw" through flesh. "Caustic" is often used synonymously with "corrosive" but strictly refers to strong bases/alkalis; however, medical literature groups both acids and alkalis under "caustic." — Cummings Otolaryngology, p. 3984
Classification of Corrosive Agents
| Class | pH | Examples | Common Products |
|---|---|---|---|
| Alkali (bases) | >7 | Sodium hydroxide (NaOH/lye), potassium hydroxide (KOH), ammonia | Drain cleaners (Drano, Liquid Plumbr), oven cleaners, hair relaxers, dish detergents |
| Acids | <7 | Sulfuric acid, hydrochloric acid, nitric acid, formic acid, acetic acid | Toilet bowl cleaners, swimming pool cleaners, rust removers, battery fluid |
| Bleaches/Oxidants | ~7 | Sodium hypochlorite | Mildew removers, household bleach |
Mechanisms of Tissue Injury
Alkalis → Liquefaction Necrosis
Strong alkalis cause liquefaction necrosis — rapid disintegration of mucosa with deep penetration into tissues. The process involves:
- Intense inflammatory reaction and edema
- Hemorrhagic congestion and eosinophilic necrosis
- Bacterial invasion and saponification (tissue fats + lye form a viscous, soap-like mass)
- Thrombosis → further compromise of blood supply → necrosis and perforation
Because there is no coagulum barrier, alkalis penetrate full thickness and cause the most severe esophageal injuries (60–80% of serious cases). NaOH (lye) at pH 13–14 (drain cleaners) is the most dangerous.
Acids → Coagulation Necrosis
Acids cause coagulation necrosis — denaturation of proteins forming a gel-like coagulum on the mucosa. This coagulum limits deep penetration in the esophagus. However:
- Acids cause greater injury to the stomach, where the higher pH may allow deeper penetration
- Gastric complications: pyloric stenosis, gastric outlet obstruction, perforation with peritonitis
Severity Factors
The severity of tissue injury depends on:
- pH — the more extreme, the more severe
- Concentration of the agent
- Contact time — solid/crystal forms adhere longer; liquids cause more circumferential burns
- Volume ingested
Timeline of Tissue Injury (Alkali)
| Time | Pathological Event |
|---|---|
| First 24 hr | Epithelial degeneration, lymphocytic submucosa infiltration |
| Day 4 | Fibroblasts and new blood vessels emerge |
| Day 7 | Necrosis complete |
| Week 2 | Granulation tissue predominates, contractile (stricture) stage begins |
| 3–4 weeks | Established strictures |
Endoscopic Grading (Zargar Classification)
| Grade | Findings |
|---|---|
| 0 | No injury |
| 1 | Mucosal edema and hyperemia |
| IIa | Superficial, non-circumferential whitish membranes, shallow ulcers, hemorrhage |
| IIb | Deep, circumferential lesions with stricture formation |
| IIIa | Small, scattered areas of necrosis |
| IIIb | Extensive necrosis |
| IV | Perforation |
Circumferential injuries have an extremely high likelihood of stricture formation. — Cummings Otolaryngology, p. 3985
Clinical Presentation
Common symptoms:
- Vomiting (most common), dysphagia, drooling
- Oral pain, odynophagia
- Chest pain, abdominal pain
Danger signs (perforation):
- Fever + chest/abdominal pain + hypotension
Laryngeal injury (especially with powders): hoarseness, stridor, nasal flaring, retractions — onset within hours
Severe complications: hemolysis, DIC, renal failure, peritonitis, mediastinitis, metabolic acidosis, CNS depression, death — Cummings Otolaryngology, p. 3985–3986
Important: The presence/absence of oral lesions does not predict esophageal injury. In one series of 473 cases, 61% of patients without oral lesions had esophageal injuries. Conversely, 82% of symptomatic children had no esophageal injury. — Cummings Otolaryngology, p. 3986
Management Algorithm
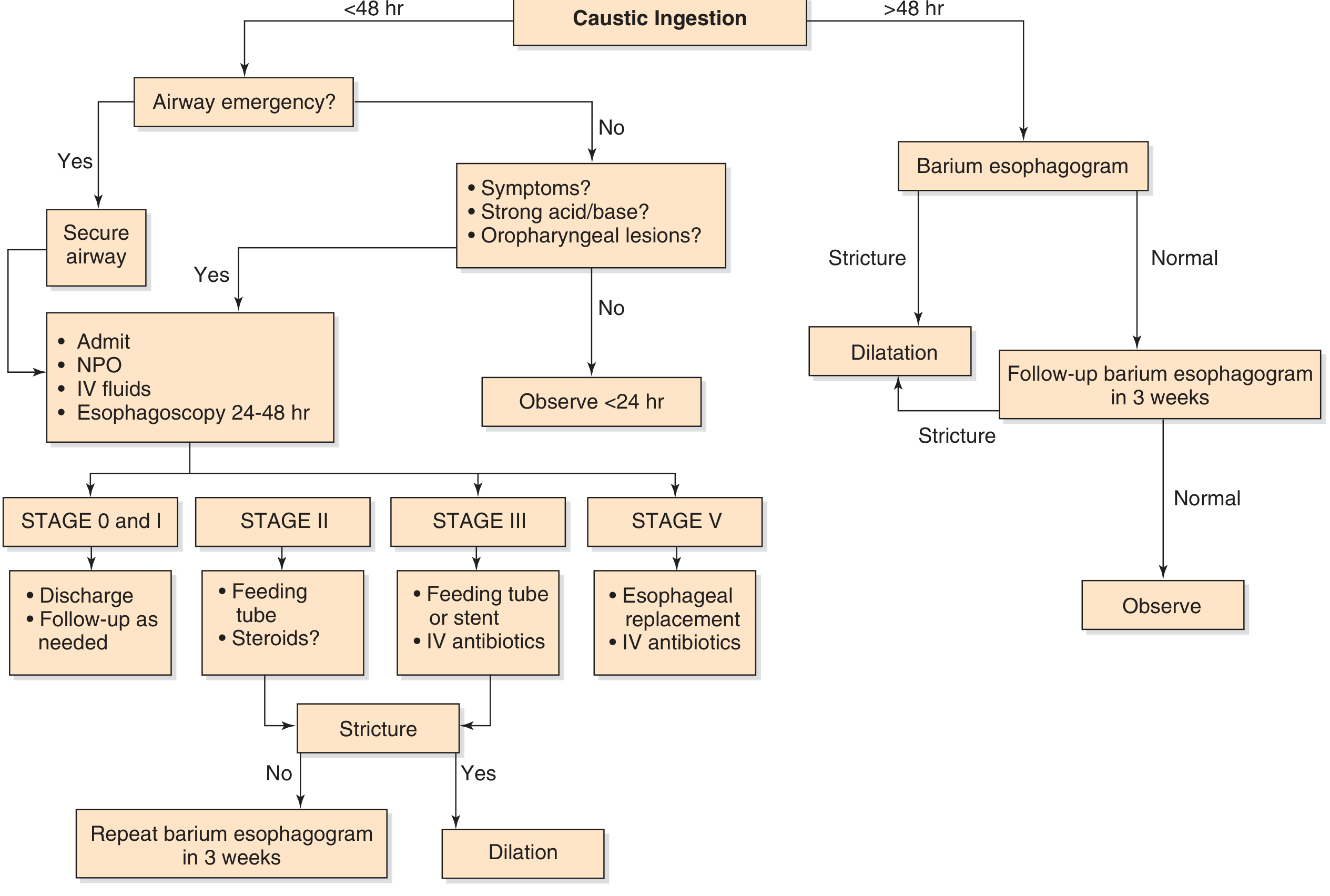
Immediate Steps
- Secure airway if emergency (flexible fiberoptic intubation preferred to avoid emergency cricothyrotomy)
- Do NOT induce vomiting — re-exposes the esophagus/larynx to corrosive
- Do NOT give activated charcoal — does not adsorb caustic agents
- Oral dilution — limited to ≤15 mL/kg of water or milk (may reduce injury, but evidence in humans is weak; excessive amounts may trigger vomiting)
- Blind NG tube placement is contraindicated — risk of perforation
- IV fluids + NPO if admitted
- Chest/abdominal X-ray — rule out free air (mediastinum or peritoneum)
Neutralization (Schwartz's Surgery):
- Alkali → neutralize with half-strength vinegar, lemon juice, or orange juice (within 1 hour)
- Acid → neutralize with milk, egg white, or antacids
- Sodium bicarbonate is avoided (generates CO₂ → risk of perforation)
Endoscopy
- Optimal window: 12–48 hours after ingestion
- <12 hours: evolving lesion may be missed
-
48 hours: necrotic tissue sloughs, esophageal wall too weak → risk of perforation
- Do not advance scope beyond the first level of burn to avoid perforation
- If presenting >48 hours: barium esophagogram instead
Stage-Based Management
| Stage | Management |
|---|---|
| 0–I | Discharge, follow-up as needed |
| II | Feeding tube; steroids (controversial) |
| III | Feeding tube or stent, IV antibiotics |
| IV/V | Esophageal replacement, IV antibiotics |
Stricture Management
- 60% of strictures develop within 1 month; 80% within 2 months
- Fluoroscopically guided balloon dilation (with concurrent esophagoscopy)
- Retrograde dilation via gastrostomy + transesophageal string technique for severe cases
- If strictures do not develop within 8 months, unlikely to occur — Schwartz's Surgery, p. 1113
Special Agents
Hydrofluoric Acid (HFA)
Although corrosive, the hydrogen ion plays a relatively minor role in HFA injury. The fluoride ion is the primary culprit — a protoplasmic poison that causes systemic toxicity including hypocalcemia and cardiac arrhythmias, requiring systemic calcium treatment. — Roberts & Hedges' Clinical Procedures in Emergency Medicine
Bleach (Sodium Hypochlorite, pH ~7)
- Acts as a mild irritant, not a true caustic
- Rarely causes deep penetration or stricture formation
- Common misconception that bleach causes severe injury
Location of Caustic Injury (Distribution)
| Location | Frequency |
|---|---|
| Esophagus (overall) | 70% |
| — Middle third | 65% |
| — Upper | 15% |
| — Lower | 2% |
| — Whole esophagus | 18% |
| Stomach | 20% |
| Pharynx | 10% |
| Both esophagus and stomach | 14% |
— Schwartz's Principles of Surgery, p. 1114
Long-term Complications
- Esophageal stricture (most common late complication)
- Gastric outlet obstruction / pyloric stenosis (acid ingestion)
- Tracheoesophageal fistula
- Increased risk of esophageal carcinoma (squamous cell carcinoma — risk rises 1,000-fold decades after lye ingestion)
- Mediastinitis, peritonitis
Sources: Cummings Otolaryngology Head and Neck Surgery | Schwartz's Principles of Surgery, 11th ed. | K.J. Lee's Essential Otolaryngology | Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.