
WhatsApp Image 2026-06-18 at 2.40.25 PM.jpeg
explain case and answer the question
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed. Here is the full case explanation and answers to all 6 questions:
Blunt Chest Trauma - Case Analysis
Clinical Case Summary
Patient: Azmat Ali, 40-year-old male
Mechanism: Road traffic accident - driver hit a steering pole (blunt frontal chest trauma)
Vitals: BP 110/70 mmHg, Pulse 100/min, SpO2 95%
Examination findings:
- Diminished air entry on the right middle and lower zones
- Paradoxical chest wall movements (the hallmark sign)
- Bilateral rib fractures at multiple sites on X-ray
Diagnosis: Flail Chest
The paradoxical movements + multiple bilateral rib fractures at multiple sites = classic flail chest from blunt trauma. The plan for endotracheal intubation and mechanical ventilation is the correct management.
Answers to All Six Questions
Q1. Which bony and cartilaginous structures contribute to the formation and stability of the thoracic cage?
The thoracic cage is formed by:
Bony components:
- 12 pairs of ribs - provide the lateral walls
- 12 thoracic vertebrae - form the posterior wall
- Sternum (manubrium, body, xiphoid process) - forms the anterior midline
Cartilaginous components (critical for stability):
- Costal cartilages of ribs 1-7 (true ribs) - connect directly to the sternum, providing anterior rigidity
- Costal cartilages of ribs 8-10 (false ribs) - attach to the costal cartilage above, forming the costal margin - this "chain link" arrangement absorbs force and adds flexibility
- Ribs 11-12 (floating ribs) - have no anterior attachment; contribute little to anterior stability
How these contribute to stability:
The cage is an elastic, compressible structure. The articulations between ribs and vertebrae (costovertebral joints), between ribs and cartilages, and the costal cartilages joining the sternum all work together to resist deformation while allowing respiratory excursion. Anterior connections via costal cartilage are the most vulnerable to blunt frontal impact.
(Gray's Anatomy for Students)
Q2. How can a typical rib be distinguished from an atypical rib based on its anatomical features?
| Feature | Typical Rib (Ribs 3-9) | Atypical Ribs |
|---|---|---|
| Head | Two articular facets (demifacets for its own + adjacent vertebra) | Single facet |
| Neck | Present and distinct | Variable or absent |
| Tubercle | Present; has articular + non-articular parts | Modified or absent |
| Shaft | Curved, with angle, costal groove on inferior inner surface | Variable |
| Anterior end | Connects to costal cartilage | Variable |
Atypical Ribs and their distinguishing features:
- Rib I: Flat in horizontal plane (broadest); single facet on head (only articulates with T1); has the scalene tubercle separating subclavian artery groove (posterior) from subclavian vein groove (anterior); shortest and most curved
- Rib II: Flat but twice as long as Rib I; has a roughened area (tuberosity for serratus anterior)
- Rib X: Head has a single facet (articulates only with T10)
- Ribs XI & XII (floating ribs): No neck, no tubercle, no anterior connection; short, pointed anteriorly; articulate only with the body of their own vertebra; have no transverse costal facets
(Gray's Anatomy for Students)
Q3. Why does a patient with multiple fractures of adjacent ribs develop paradoxical movement of the chest wall during respiration?
This is the core pathophysiology of flail chest.
Mechanism:
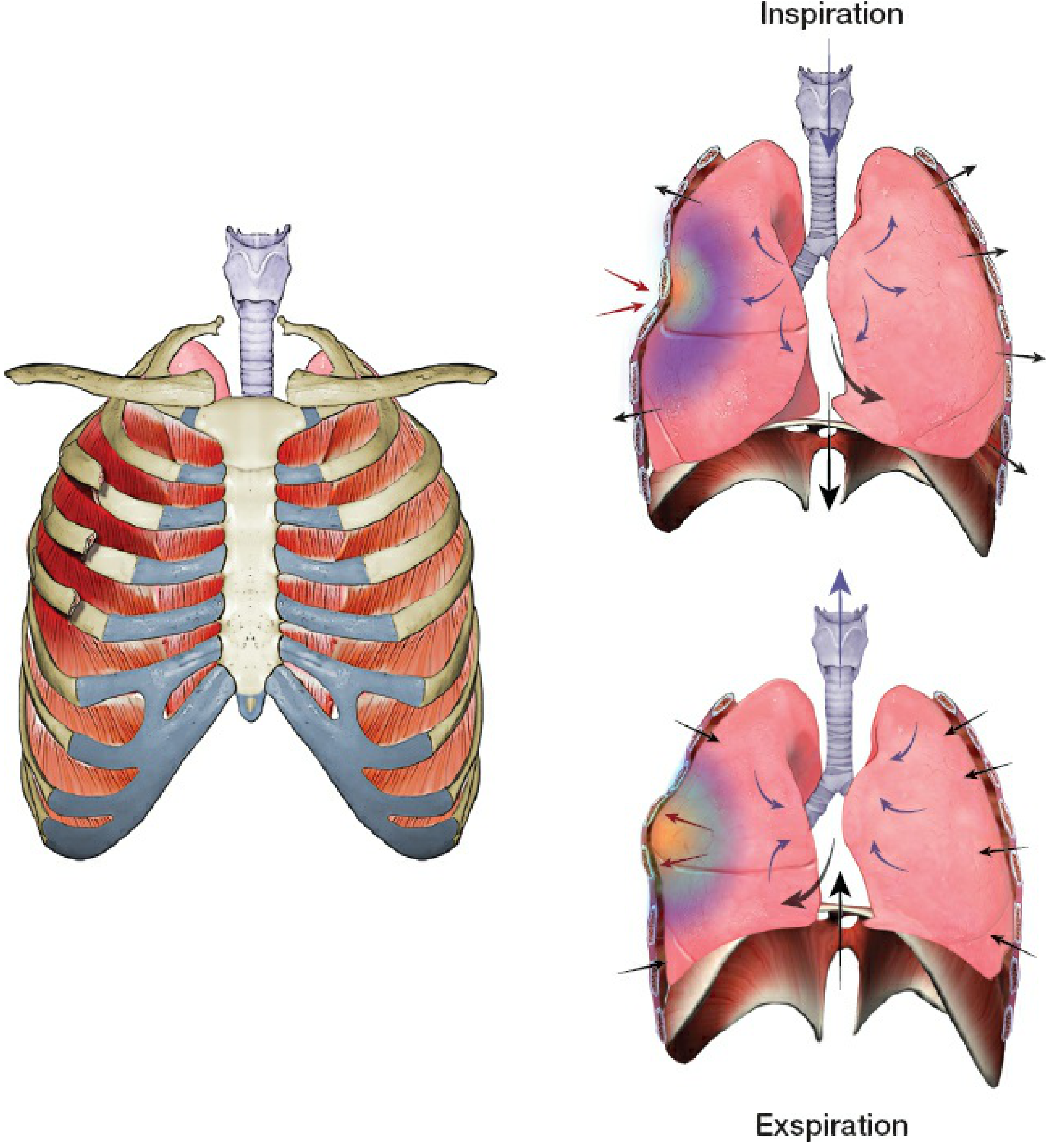
Normally, the chest wall moves as a single unit - outward during inspiration (as diaphragm descends and intrathoracic pressure drops) and inward during expiration.
When 3 or more consecutive ribs are fractured in 2 or more locations, a "flail segment" is created - a section of chest wall that is no longer mechanically connected to the rest of the thoracic cage.
- During inspiration: Intrathoracic pressure drops (becomes more negative). The intact chest wall expands outward, but the flail segment - lacking bony continuity - is pushed inward by the relatively higher atmospheric pressure. This is the paradoxical motion.
- During expiration: Intrathoracic pressure rises. The intact chest wall moves inward, but the flail segment is pushed outward.
This means the flail segment moves opposite to the rest of the chest wall with each breath.
Consequences:
- Reduced tidal volume and ineffective ventilation
- Underlying pulmonary contusion reduces lung compliance, worsening the defect
- The work of breathing increases dramatically, risking respiratory failure
(Rockwood & Green's Fractures in Adults, 10th ed. 2025)
Q4. What types of injuries or accidents are most commonly associated with blunt trauma to the chest?
| Mechanism | Frequency |
|---|---|
| Motor vehicle collision (MVC) | ~79% - the most common cause |
| Falls from height | ~16% |
| Other blunt trauma (assault, crush injuries, sports) | ~5% |
In MVCs specifically, the typical injury pattern involves the driver's chest striking the steering wheel (as in Azmat Ali's case), causing direct anterior impact. This typically fractures ribs in two places - creating an anterolateral or posterolateral flail segment.
Other injury patterns:
- Crush injuries - "caved-in chest," causing severe rib displacement and potential impaling of lung or diaphragm
- Falls - can cause posterior rib fractures (associated with less severe clinical derangement due to splinting by paravertebral muscles)
- Anterior flail chest - sternum separates from ribs via costal cartilage fractures (common in steering wheel impact)
Up to 39% of patients with blunt chest trauma are diagnosed with rib fractures. Of these, the majority are isolated (58%), multiple in 41%, and flail chest in ~1.5% - but this small group carries the highest morbidity and mortality.
(Rockwood & Green's Fractures in Adults, 10th ed. 2025)
Q5. What potentially life-threatening complications should be suspected in a patient following significant blunt chest trauma?
The following complications must be actively screened for:
| Complication | Why It Occurs |
|---|---|
| Pulmonary contusion | Direct lung parenchymal injury beneath fractured ribs; reduces compliance; most common cause of hypoxia in blunt chest trauma |
| Pneumothorax | Fractured rib end pierces pleura; air enters pleural space; lung collapses - explains diminished air entry on the right in this patient |
| Tension pneumothorax | Air accumulates under pressure; mediastinum shifts; cardiac output drops - rapidly fatal if untreated |
| Hemothorax | Bleeding into pleural space from intercostal vessels or lung laceration |
| Hemopneumothorax | Combined blood + air in pleural space |
| Aortic injury / traumatic aortic dissection | High deceleration forces can tear the aorta at the ligamentum arteriosum |
| Cardiac contusion / tamponade | Blunt precordial impact may bruise myocardium or cause pericardial bleeding |
| Diaphragmatic rupture | Especially with lower rib fractures; abdominal viscera can herniate into the chest |
| Tracheobronchial injury | Rare but life-threatening; causes massive air leak |
| Respiratory failure | The end result of flail chest + pulmonary contusion + pain-related splinting |
In Azmat Ali's case, the SpO2 of 95% and diminished air entry on the right strongly suggest a co-existing right-sided pneumothorax or hemothorax that needs urgent attention alongside management of flail chest.
Q6. What is the procedure of bilateral chest intubation?
The question refers to endotracheal intubation as a procedure for managing flail chest, with bilateral verification of tube placement.
Endotracheal Intubation - Step-by-Step:
- Pre-oxygenate the patient with 100% O2 for 3-5 minutes
- Position: "Sniffing position" - neck flexed, head extended (align oral, pharyngeal, laryngeal axes)
- Rapid Sequence Induction (RSI): Administer IV sedative (e.g., ketamine or etomidate) + neuromuscular blocker (e.g., succinylcholine)
- Laryngoscopy: Insert laryngoscope into right corner of mouth, sweep tongue left, advance to vallecula (Mac blade) or epiglottis (Miller blade); visualize vocal cords
- Tube insertion: Pass cuffed endotracheal tube through vocal cords (typically 21-23 cm at lips in adults)
- Cuff inflation: Inflate cuff to seal airway (20-30 cmH2O)
- Verification of bilateral placement:
- Auscultate bilateral lung sounds (both axillae)
- Confirm bilateral chest rise visually
- Absence of epigastric gurgling (rules out esophageal intubation)
- Confirm with end-tidal CO2 (capnography) - gold standard
- Confirm position with chest X-ray (tip should be 2-3 cm above carina)
- Secure the tube and connect to mechanical ventilator
Why intubation is indicated in flail chest:
Positive-pressure mechanical ventilation acts as an "internal pneumatic splint" - it stabilizes the flail segment by maintaining positive intrathoracic pressure throughout the respiratory cycle, eliminating the pressure gradient that causes paradoxical motion.
(Current Surgical Therapy, 14th ed.)
Case Summary Table
| Clinical Finding | Anatomical/Pathological Explanation |
|---|---|
| Paradoxical chest movements | Flail segment (bilateral multi-site rib fractures) loses chest wall continuity |
| Diminished air entry right middle/lower zones | Right pneumothorax or hemothorax from fractured rib |
| SpO2 95% (hypoxia) | Pulmonary contusion + ineffective ventilation from flail segment |
| BP 110/70, Pulse 100 | Compensated shock from pain, blood loss, or early tamponade |
| Plan for ETI | Positive pressure ventilation = internal splint for flail segment |
This is a shared conversation. Sign in to Orris to start your own chat.