COPD
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic obstructive pulmonary disease"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"COPD"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material for a detailed COPD overview. Let me compile the full answer.
Chronic Obstructive Pulmonary Disease (COPD)
Definition
COPD is defined by the WHO as "a common, preventable and treatable disease characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities caused by exposure to noxious particles or gases." The diagnostic spirometric criterion is a post-bronchodilator FEV1/FVC ratio < 0.70. - Goldman-Cecil Medicine, p. 890
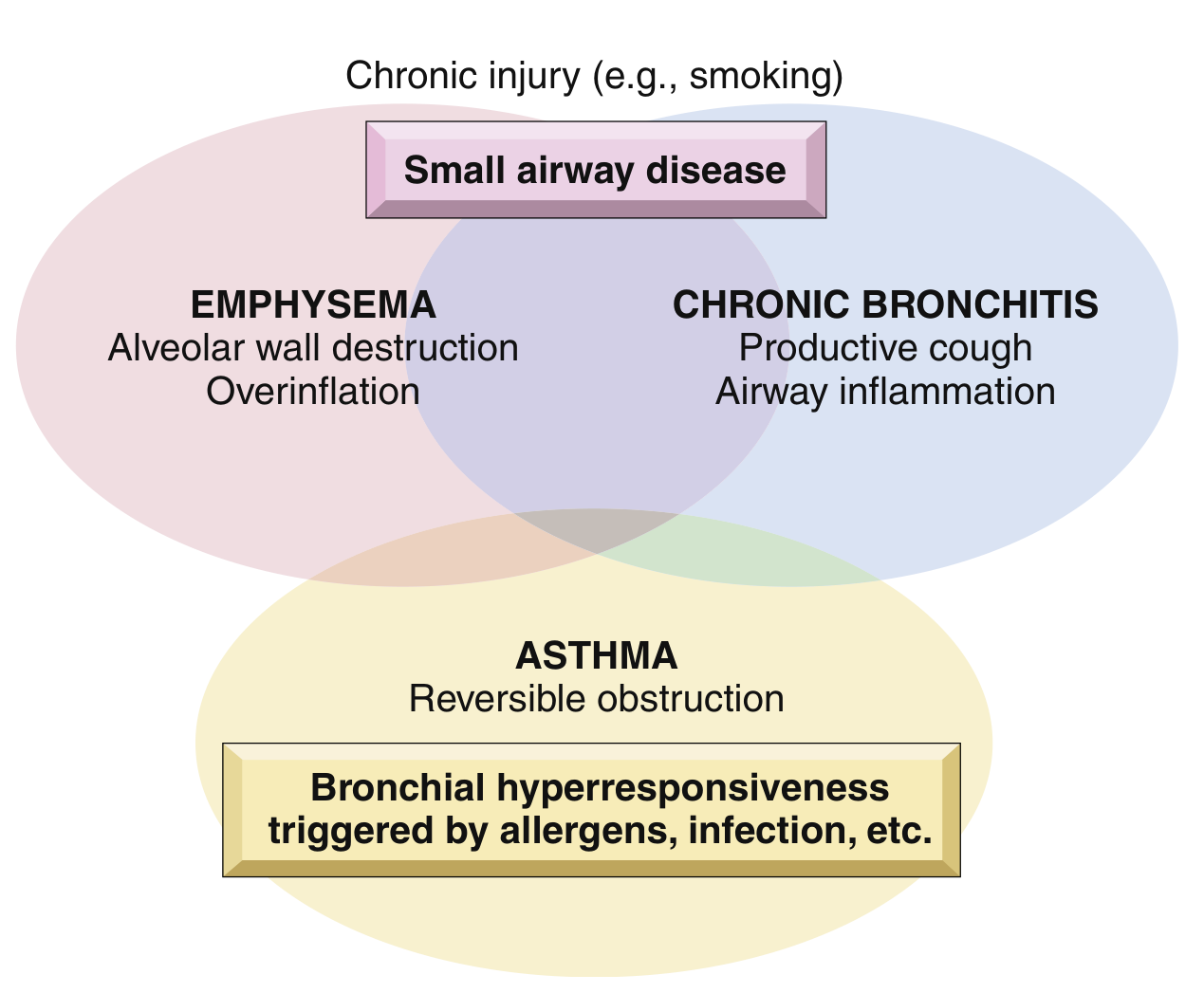
The COPD Spectrum
COPD is not a single entity but an umbrella term. Nearly all patients have features of both emphysema (alveolar wall destruction) and chronic bronchitis (daily productive cough for ≥3 months in ≥2 consecutive years):
Epidemiology
-
Affects >10% of U.S. adults over age 40; global prevalence ~175 million
-
Third leading cause of death worldwide, responsible for ~3.2 million deaths/year
-
Annual U.S. costs estimated at $50 billion (~$30B direct, ~20B indirect)
-
35-50% of heavy smokers develop COPD; ~80% of COPD is attributable to smoking
-
Women appear more susceptible than men
-
Robbins Basic Pathology, p. 447; Goldman-Cecil Medicine, p. 890
Risk Factors
| Category | Examples |
|---|---|
| Primary | Cigarette smoking (pack-years inversely correlated with FEV1) |
| Indoor exposure | Biomass fuel combustion in poorly ventilated spaces |
| Occupational | Dust in mines, grain facilities, cotton mills |
| Developmental | Poor lung development, childhood respiratory infections |
| Genetic | Alpha-1 antitrypsin (AAT) deficiency (panacinar emphysema) |
| Other | Airway hyperresponsiveness, environmental air pollution |
Pathology
Emphysema Patterns
-
Centriacinar (centrilobular) - most common; involves central/proximal acini while distal alveoli are spared; upper-lobe predominant; caused by cigarette smoking (~20x more common than panacinar)
-
Panacinar (panlobular) - uniform enlargement from respiratory bronchiole to terminal alveoli; lower-lobe predominant; associated with AAT deficiency
-
Distal acinar (paraseptal) - affects acini distal to the respiratory bronchiole, near pleura; causes bullae; presents as spontaneous pneumothorax in young adults
-
Irregular - associated with scarring; usually clinically insignificant
Chronic Bronchitis Pathology
- Hypersecretion of mucus from enlarged Reid index (ratio of mucous gland to bronchial wall thickness) >0.4
- Goblet cell hyperplasia, squamous metaplasia, airway inflammation
Pathogenesis
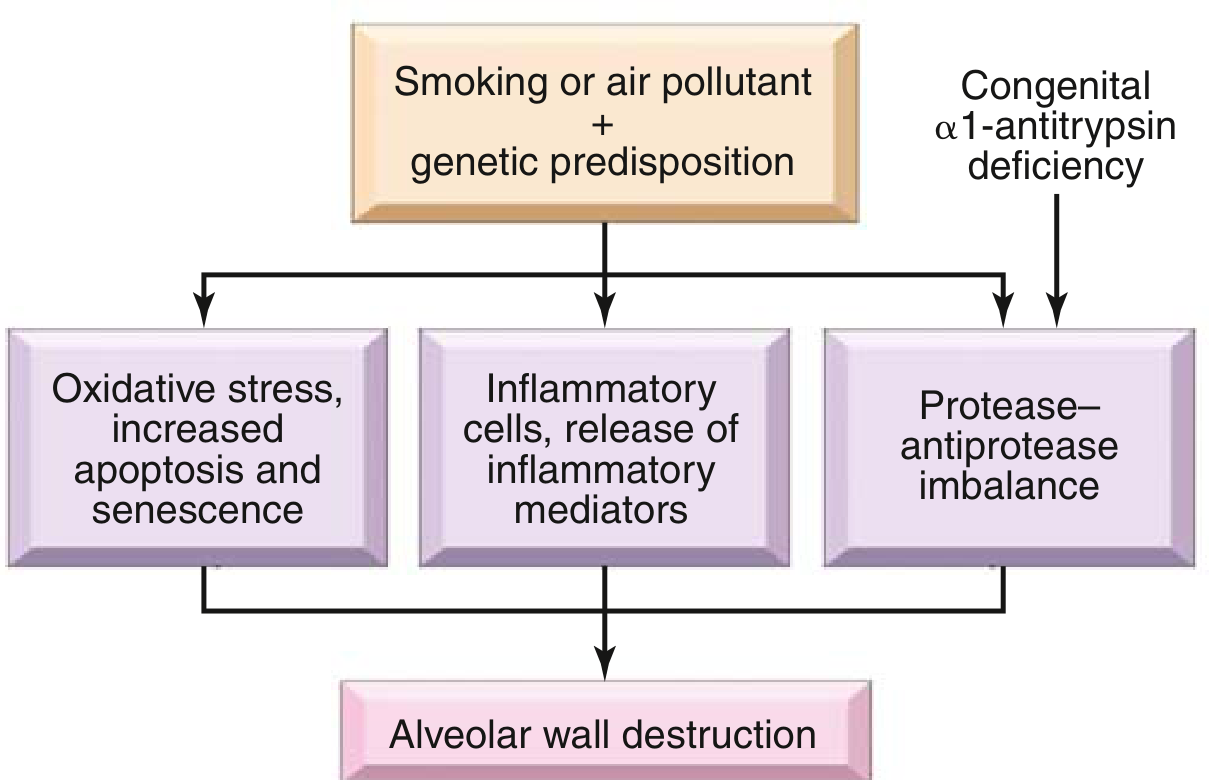
Three key mechanisms operate together:
- Inflammatory cells and mediators - neutrophils, macrophages, CD4+/CD8+ T cells release LTB4, IL-8, TNF-alpha
- Protease-antiprotease imbalance - elastases (MMP, neutrophil elastase) exceed antiproteases (AAT), leading to connective tissue breakdown
- Oxidative stress - reactive oxygen species from cigarette smoke and activated inflammatory cells cause increased apoptosis and cellular senescence
- Robbins Basic Pathology, p. 448
Clinical Features
Symptoms (progressive over years)
- Dyspnea on exertion (earliest complaint) progressing to rest
- Chronic productive cough (bronchitis component)
- Wheezing, chest tightness
- In advanced disease: breathlessness with basic ADLs
Physical Examination
- Early: often normal
- Later: prolonged expiratory phase, expiratory wheezing
- Hyperinflation signs: barrel chest, poor diaphragmatic excursion, hyperresonance
- Severe: accessory muscle use (sternocleidomastoid, scalenes), "tripod" posture, cyanosis
- Advanced: cachexia, weight loss (elevated TNF-alpha), cor pulmonale (right heart failure), peripheral edema
Important: Clubbing is NOT a feature of COPD - its presence should prompt evaluation for lung cancer or other causes. - Harrison's, p. 2298
"Pink Puffer" vs "Blue Bloater"
| Pink Puffer (emphysema-predominant) | Blue Bloater (chronic bronchitis-predominant) | |
|---|---|---|
| Build | Thin, cachexic | Overweight |
| Breathing | Pursed-lip, tachypneic | Normal/slow rate |
| Cyanosis | Absent | Present |
| PaCO2 | Low/normal | Elevated (hypercapnic) |
| Hypoxemia | Mild | Severe |
| Cor pulmonale | Late | Early/common |
Diagnosis
Spirometry (mandatory)
- Post-bronchodilator FEV1/FVC < 0.70 confirms airflow obstruction
- GOLD spirometric grading (based on FEV1 % predicted):
| GOLD Grade | FEV1 % Predicted |
|---|---|
| GOLD 1 (Mild) | ≥ 80% |
| GOLD 2 (Moderate) | 50-79% |
| GOLD 3 (Severe) | 30-49% |
| GOLD 4 (Very Severe) | < 30% |
Other investigations
- ABG: resting or exertional hypoxemia; hypercarbia in severe disease
- Chest X-ray: hyperinflation, flat diaphragms, increased AP diameter, bullae; ~25% show abnormalities during exacerbations (pneumonia, CHF, pneumothorax)
- CT chest: better assessment of emphysema distribution; detects pulmonary artery enlargement (predictor of exacerbations)
- DLCO: reduced in emphysema (reflects parenchymal destruction)
- Alpha-1 antitrypsin level: screen all patients with COPD, especially age <45 or minimal smoking history
Multidimensional Assessment
The BODE index (Body mass index, airflow Obstruction, Dyspnea, Exercise capacity) better predicts mortality than FEV1 alone. Symptoms quantified by:
- mMRC dyspnea scale (0-4)
- CAT score (COPD Assessment Test, 0-40)
GOLD ABE Classification (2024 Updated)
The current GOLD 2024 framework classifies patients into three groups based on symptoms + exacerbation history:
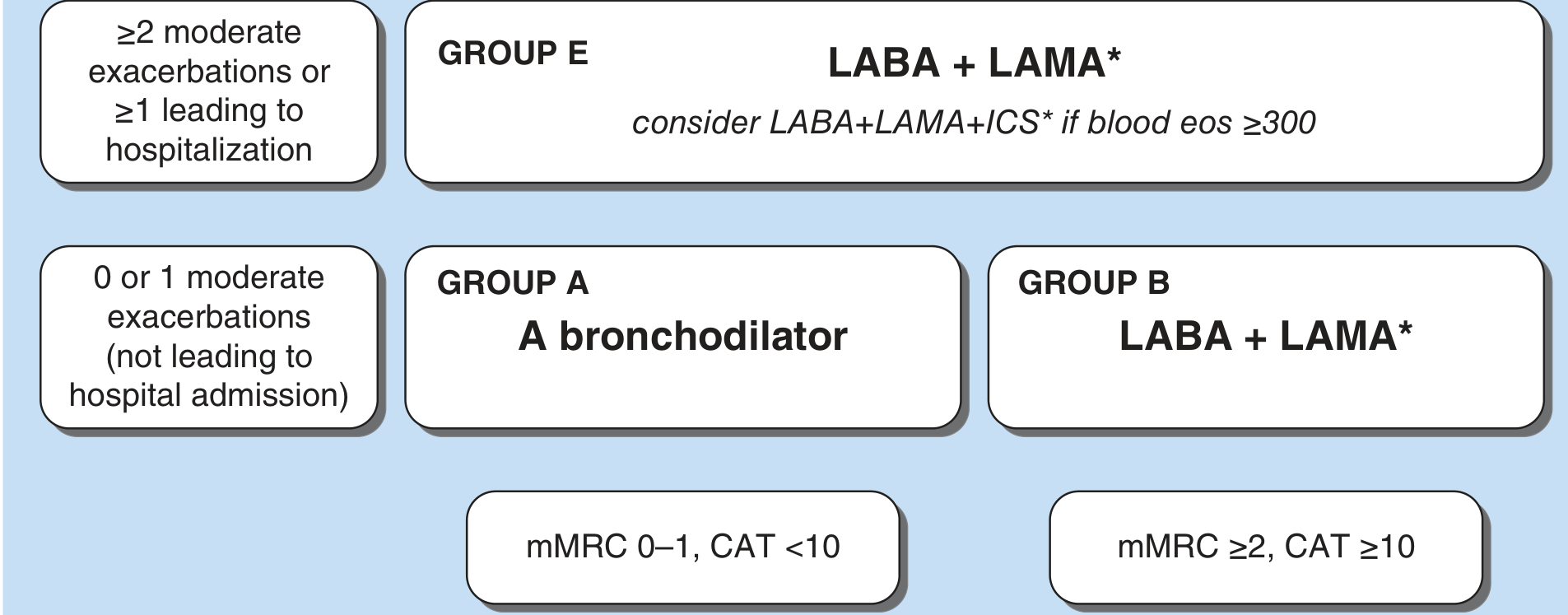
| Group | Exacerbations | Symptoms | Initial Treatment |
|---|---|---|---|
| A | 0-1 moderate (no hospitalization) | mMRC 0-1, CAT <10 | A bronchodilator (short- or long-acting) |
| B | 0-1 moderate (no hospitalization) | mMRC ≥2, CAT ≥10 | LABA + LAMA |
| E | ≥2 moderate OR ≥1 leading to hospitalization | Any | LABA + LAMA; consider LABA+LAMA+ICS if eos ≥300/µL |
From GOLD 2024 Guidelines (referenced in Harrison's 22E, 2025)
Pharmacological Management
Bronchodilators (cornerstone of therapy)
Short-acting beta-2 agonists (SABA)
- Albuterol (salbutamol), levalbuterol - PRN relief
- Available as MDI, DPI, nebulizer solution
Short-acting muscarinic antagonists (SAMA)
- Ipratropium - also available combined with albuterol (soft mist inhaler)
Long-acting beta-2 agonists (LABA)
- Salmeterol, formoterol, indacaterol - twice daily or once daily
- Never used as monotherapy in COPD (unlike asthma concerns)
Long-acting muscarinic antagonists (LAMA)
- Tiotropium (gold standard LAMA), umeclidinium, aclidinium, glycopyrronium
- Reduce exacerbations, improve exercise tolerance, slow decline in FEV1
LABA + LAMA combinations
- Preferred in symptomatic patients and high-risk; greater efficacy than either alone
Inhaled Corticosteroids (ICS)
- Never used alone in COPD (unlike asthma) - used only as add-on to bronchodilators
- Indicated when eosinophil count ≥300/µL
- Reduce exacerbation frequency in selected patients
- Side effects: pneumonia risk, oral candidiasis, osteoporosis - Harrison's, p. 2299
Other Pharmacotherapy
Roflumilast (PDE4 inhibitor)
- For severe COPD + chronic bronchitis + frequent exacerbations
- Modest benefit on airflow; side effects: nausea, diarrhea, weight loss
Chronic Azithromycin (macrolide)
- Reduces exacerbation frequency in patients with recent exacerbation history
- Most effective in older, former smokers with milder COPD
- Risks: hearing loss, macrolide resistance; avoid with prolonged QTc
Non-Pharmacological
- Smoking cessation - single most effective intervention; slows FEV1 decline
- Pulmonary rehabilitation - improves exercise capacity and quality of life
- Influenza and pneumococcal vaccination - reduce exacerbations and hospitalizations
- LTOT (Long-term oxygen therapy) - resting SpO2 ≤88% (or ≤89% with cor pulmonale, polycythemia, PH); proven mortality benefit; must be used ≥15-18 hours/day
- Lung volume reduction surgery / bronchoscopic procedures - selected patients with upper-lobe predominant emphysema and low exercise capacity
- Lung transplantation - for very severe disease refractory to all other therapy
COPD Exacerbations
An exacerbation is an acute worsening of respiratory symptoms beyond normal day-to-day variation.
Precipitants
- Viral infections (rhinovirus, influenza) - cause >50% of exacerbations by PCR studies
- Bacterial infections (new strain acquisition)
- Air pollution, allergens, pulmonary embolism (incidence elevated in COPD), medication non-adherence
Assessment in Exacerbation
- Quantify change in dyspnea, sputum character, fever, wheezing
- Pulse oximetry; ABG if severe COPD, hypercarbia suspected, altered mental status
- CXR/CT: ~25% abnormal (pneumonia, CHF, pneumothorax)
- Spirometry is NOT helpful during exacerbations (unlike asthma)
Indications for Hospitalization
- Respiratory acidosis + hypercarbia (PaCO2 >45 mmHg)
- New or worsening hypoxemia
- Severe underlying COPD
- Significant comorbidities (CHF)
- Inability to manage at home
Treatment of Exacerbations
| Agent | Role |
|---|---|
| SABAs ± SAMAs | First-line bronchodilators (intensify/escalate) |
| Systemic corticosteroids | Prednisone 40 mg/day x 5 days - shortens recovery, reduces treatment failure |
| Antibiotics | If purulent sputum or clinical indicators of bacterial infection (amoxicillin, doxycycline, or macrolide depending on resistance) |
| Controlled oxygen | Target SpO2 88-92% to avoid hypercapnic respiratory failure |
| NIV (BiPAP) | pH <7.35 + hypercarbia - reduces need for intubation, reduces mortality |
| Intubation/IMV | For NIV failure or contraindications |
- Harrison's Principles of Internal Medicine 22E, p. 2302
Comorbidities
COPD rarely exists in isolation. Important comorbidities include:
- Cardiovascular disease (most common cause of death in mild-moderate COPD)
- Lung cancer (shared risk factors; new clubbing in COPD should prompt workup)
- OSA-COPD overlap syndrome - higher risk of hypercapnia, hypoxemia, PH; diagnosed with sleep study (PSG preferred over HSAT in moderate-severe COPD)
- Osteoporosis, depression, anxiety, GERD
- Pulmonary hypertension and cor pulmonale (late complication; supplemental O2 is key treatment)
Prognosis
The BODE index is the best multidimensional mortality predictor. Poor prognostic factors include:
- Low FEV1, severe dyspnea (mMRC ≥3)
- Low 6-minute walk distance
- Low BMI / cachexia
- Frequent exacerbations
- Hypercapnia at rest
- Cor pulmonale / pulmonary hypertension
Sources: Robbins & Kumar Basic Pathology (p. 447-449) | Harrison's Principles of Internal Medicine 22E (pp. 2297-2303) | Goldman-Cecil Medicine (p. 890) | Murray & Nadel's Textbook of Respiratory Medicine (block 15, 27) | Fishman's Pulmonary Diseases and Disorders
Toxicology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.