Why headache when got hungry in tension type headache
tension type headache hunger fasting mechanism
tension type headache hypoglycemia fasting triggers
headache fasting hypoglycemia pathophysiology
why does hunger cause tension type headache mechanism pathophysiology
PMID: 19472450
Why Hunger Triggers Headache in Tension-Type Headache
1. Hypoglycemia - The Primary Trigger
- Neurons in pain-processing centers become hyperexcitable - low glucose reduces the brain's ability to maintain inhibitory neurotransmission (particularly GABA-ergic inhibition).
- This lowers the pain threshold in central nociceptive pathways, including the trigeminal nucleus and spinal dorsal horn - the very same pathways already sensitized in TTH.
- A landmark review (Torelli et al., Headache, 2009 - PMID: 19472450) confirmed that fasting headache has identical clinical features to TTH, and that the probability of onset increases directly with fasting duration. Hypoglycemia was identified as a primary causative factor.
2. Central Sensitization Already Present in TTH
- The nociceptive system in TTH patients operates with a reduced baseline threshold for pain.
- Any additional stressor - including metabolic stress from low blood sugar - tips the balance more easily, triggering a headache that might not occur in someone without this underlying sensitization.
- Studies show patients with chronic TTH have allodynia and hyperalgesia even in non-head areas (e.g., fingers), confirming a globally lowered pain tolerance.
3. Muscle Tension from Hunger-Related Stress
- Increases pericranial and cervical muscle tension (scalp, temporalis, sternocleidomastoid, trapezius).
- Myofascial trigger points in these muscles are already common in TTH, and their activation by hunger-related sympathetic tone amplifies peripheral nociceptive input.
- That peripheral input feeds the already-sensitized central nociceptive network, producing or worsening the headache.
4. Serotonin Drop
- Impairs the descending antinociceptive pathways (periaqueductal gray - rostral ventromedial medulla axis).
- Reduces the brain's natural ability to suppress pain signals.
- This is particularly relevant in TTH because decreased antinociception (inability to "turn off" pain) is one of the proposed central mechanisms in TTH.
5. Caffeine Withdrawal (if applicable)
6. Dehydration Component
Summary Table
| Mechanism | Effect in TTH |
|---|---|
| Low blood glucose | Lowers nociceptive threshold, hyperexcites pain neurons |
| Pre-existing central sensitization | Makes pain system more reactive to any metabolic trigger |
| Sympathetic activation / stress | Increases pericranial muscle tension |
| Serotonin drop | Impairs descending pain inhibition |
| Caffeine withdrawal | Cerebral vasodilation (in habitual users) |
| Dehydration | Reduces cerebral pain tolerance |
All type of treatment available for tension type headache
tension type headache treatment management
PMID: 38813682
PMID: 40129422
tension type headache all treatments acute preventive non-pharmacological 2024 guidelines
All Treatments for Tension-Type Headache (TTH)
A. ACUTE (ABORTIVE) PHARMACOLOGICAL TREATMENT
1. First-Line Simple Analgesics
| Drug | Dose | Notes |
|---|---|---|
| Ibuprofen | 400 mg | Best evidence - #1 ranked in 2024 network meta-analysis (PMID: 38813682) |
| Diclofenac-K | 12.5-25 mg | Equally effective; good safety profile |
| Acetaminophen (Paracetamol) | 1000 mg | Preferred in pregnancy or NSAID contraindication; 500 mg dose insufficient |
| Aspirin | 500-1000 mg | Long-established; some GI risk |
| Naproxen | 500 mg | Second-line; slower onset |
| Ketoprofen | 25 mg | Effective but higher adverse event rate |
Evidence: A 2024 network meta-analysis confirmed ibuprofen and diclofenac-K are the top two acute options with the highest 2-hour pain-free rates (RR 2.86 and 2.61 vs placebo respectively) - PMID: 38813682.
2. Combination Analgesics
- Aspirin + acetaminophen + caffeine - caffeine acts as adjuvant, significantly boosts efficacy of any analgesic
- Acetaminophen + isometheptene + dichloralphenazone - useful for moderately severe attacks
- Ibuprofen or aspirin + caffeine
⚠️ Caution: Combination analgesics with codeine, butalbital, or propoxyphene should be avoided - high risk of medication overuse headache (MOH) with frequent use.
3. Muscle Relaxants (Adjunct for Acute Use)
- Tizanidine, cyclobenzaprine, methocarbamol - can help when significant pericranial muscle tension is present
- Not first-line; typically reserved for severe acute episodes with neck/shoulder involvement
B. PREVENTIVE (PROPHYLACTIC) PHARMACOLOGICAL TREATMENT
1. Tricyclic Antidepressants (TCAs) - FIRST-LINE
| Drug | Dose | Notes |
|---|---|---|
| Amitriptyline | 50-150 mg/day (start 10-25 mg at bedtime) | Most effective prophylactic; >50% improvement in 65% of patients (Bradley and Daroff's Neurology, p. 2495) |
| Nortriptyline | 25-100 mg/evening | Better tolerated than amitriptyline; less sedation |
| Doxepin | 25-75 mg/day | Also useful |
| Maprotiline | 10-25 mg/day | Tetracyclic; TCA-like profile |
TCAs are more efficacious than SSRIs for TTH prevention (Goldman-Cecil Medicine, p. 3817).
2. Other Antidepressants (Second-Line)
- Mirtazapine - noradrenergic/serotonergic; good evidence in TTH
- Fluoxetine - 10-20 mg/day; less effective than TCAs but useful if TCAs not tolerated
- Venlafaxine (SNRI) - some evidence for chronic TTH
3. Anticonvulsants / Mood Stabilizers
- Gabapentin - modest evidence; sometimes used as adjunct
- Sodium valproate - second-line; effective in some patients
- Topiramate - second-line; weight loss side effect can be advantageous
4. Botulinum Toxin (OnabotulinumtoxinA)
- Localized injection into pericranial muscles
- Evidence is limited and mixed for TTH specifically (unlike in chronic migraine where it is approved)
- The 2024 VA/DoD CPG found onabotulinumtoxinA did not show significant benefit for chronic TTH
- May still be tried in refractory cases with significant myofascial involvement
C. NON-PHARMACOLOGICAL TREATMENTS (Recommended as First-Line for Prevention)
1. Physical Therapy
- Neck-shoulder strength exercises - significant reduction in headache intensity, duration, and frequency (PMID: 40129422)
- Manual therapy / cervical mobilization - targets myofascial trigger points in trapezius, suboccipital, and sternocleidomastoid muscles
- Posture correction - particularly relevant for patients with desk/screen work
- Massage therapy - scalp and neck; short-term benefit well established
2. Psychological / Behavioral Interventions
- Cognitive Behavioral Therapy (CBT) - helps identify and modify stress-related thought patterns that lead to muscle tension; evidence-based, especially for chronic TTH
- Biofeedback - patients learn to consciously reduce pericranial muscle activity using EMG feedback; a 2008 meta-analysis confirmed it as evidence-based; strong psychological component
- Relaxation therapy - progressive muscle relaxation, diaphragmatic breathing, guided imagery; often combined with biofeedback
- Stress management training - since stress is the #1 trigger for episodic TTH
3. Acupuncture
- Traditional acupuncture and electroacupuncture both have supporting evidence
- A 2024 systematic review and network meta-analysis (PMID: 39703352) confirmed efficacy of acupuncture-related therapies for TTH
- Electroacupuncture showed significant improvement in headache duration and intensity (PMID: 40129422)
4. Occupational Therapy
- Ergonomic workplace assessment and modification
- Particularly useful when TTH is triggered by sustained postures or repetitive movements
5. Lifestyle Modifications
| Modification | Rationale |
|---|---|
| Regular meals (avoid skipping) | Prevents hypoglycemia-triggered headaches |
| Adequate hydration | Dehydration is a common trigger |
| Regular sleep schedule | Sleep disruption worsens TTH |
| Aerobic exercise (regular) | Reduces frequency of episodic TTH |
| Caffeine moderation | Prevents withdrawal headaches |
| Screen time limits / breaks | Reduces postural and eye-strain triggers |
6. Sleep Optimization
- Screening for obstructive sleep apnea (OSA) is recommended in frequent/chronic TTH - OSA is an independent risk factor for TTH (Bradley and Daroff's Neurology, p. 2495)
- Treating OSA can significantly reduce TTH frequency
D. INTERVENTIONAL / EMERGING TREATMENTS
| Treatment | Evidence |
|---|---|
| Peripheral nerve blocks (greater occipital nerve) | Used in refractory chronic TTH; case series evidence |
| Dry needling (trigger point needling) | Targets active myofascial trigger points; improving evidence |
| Transcranial magnetic stimulation (TMS) | Limited evidence; investigational |
| Transcutaneous electrical nerve stimulation (TENS) | Some evidence for pericranial application |
E. WHAT TO AVOID
- Opioids - never indicated for TTH; risk of MOH and dependency
- Triptans - specific to migraine mechanism; not effective in TTH
- Frequent use of any acute analgesic (>10-15 days/month) - causes medication overuse headache, which transforms episodic TTH into a daily refractory headache syndrome
Quick Reference Summary
EPISODIC TTH (mild-moderate, infrequent):
→ Ibuprofen 400 mg or Acetaminophen 1000 mg
→ + lifestyle modifications
EPISODIC TTH (frequent attacks):
→ Add: CBT, biofeedback, relaxation, physical therapy
→ Consider: amitriptyline low dose
CHRONIC TTH (>15 days/month):
→ Amitriptyline 50-100 mg/day (first-line)
→ Physical therapy + CBT + biofeedback
→ Second-line: nortriptyline, mirtazapine, valproate, topiramate
→ Refractory: nerve blocks, acupuncture, botulinum toxin (selected cases)
Interventional treatment for tth
tension type headache interventional nerve block trigger point injection
interventional treatments tension type headache nerve block trigger point botulinum toxin neuromodulation 2024
tension type headache occipital nerve block trigger point injection
tension headache dry needling neuromodulation sphenopalatine
https://practicalneurology.com/archives/may-jun-2025-issue/n…
tension type headache botulinum toxin neuromodulation transcranial
tension headache ultrasound guided injection dry needling RCT
Interventional Treatments for Tension-Type Headache
1. PERIPHERAL NERVE BLOCKS (PNBs)
A. Greater Occipital Nerve Block (GONB) - Most Common
- Palpate the posterior occipital protuberance
- Move 1.5-2 cm laterally, feel for the occipital artery pulsation and groove
- Inject 2-3 mL of 0.5% bupivacaine ± 20 mg triamcinolone or Depo-Medrol, down to the periosteum, fanning out
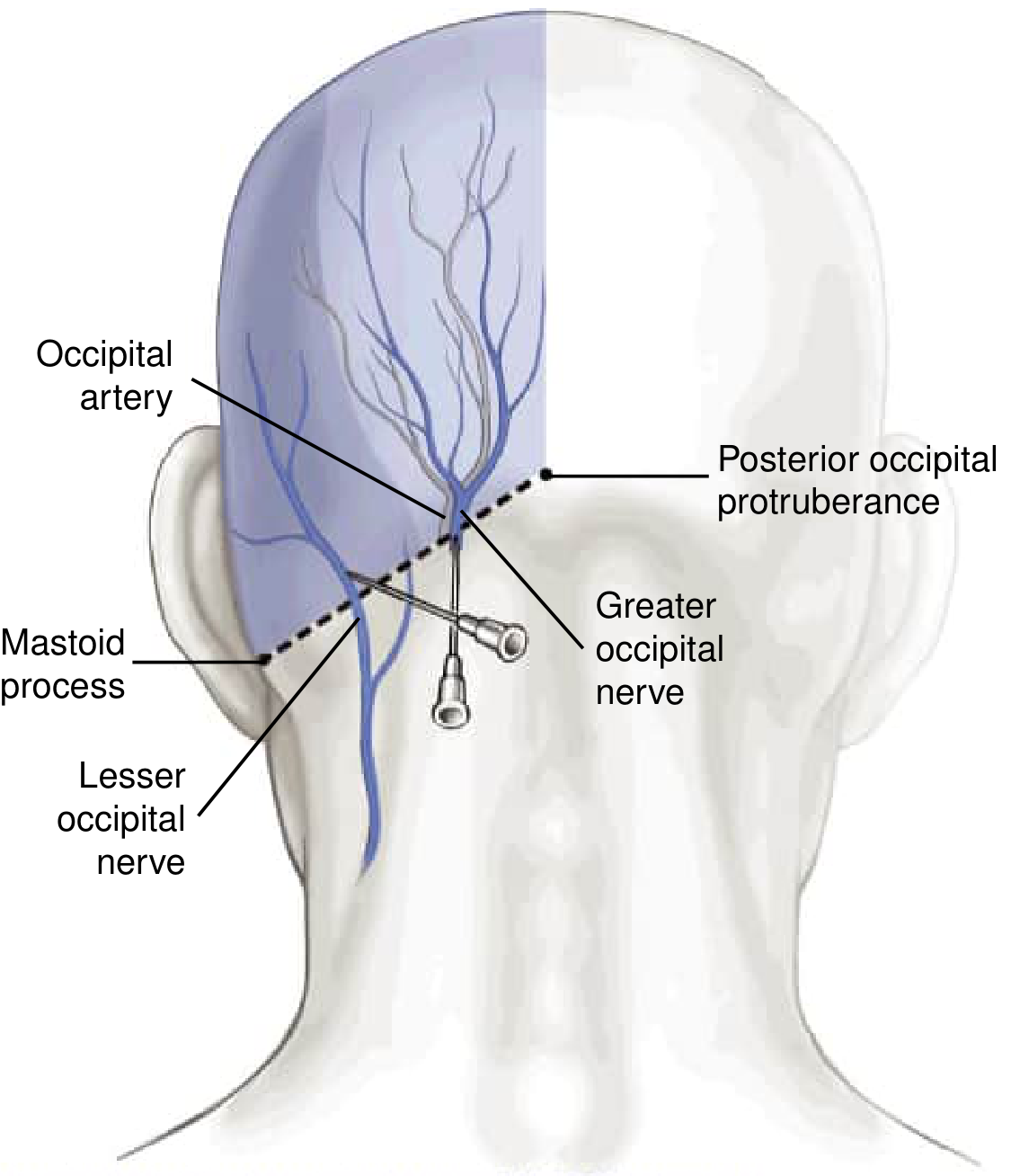
B. Lesser Occipital Nerve Block
- Done simultaneously with GONB for broader posterior scalp coverage
- Injected over the posterior border of the middle third of the sternocleidomastoid
- Must remain subcutaneous; avoid intravascular structures
C. Pericranial Nerve Block (Multi-Nerve "En Bloc" Block)
| Nerve | Area covered |
|---|---|
| Greater occipital nerve (C2) | Posterior scalp |
| Lesser occipital nerve (C2-C3) | Posterior-lateral scalp |
| Third occipital nerve (C3) | Lower occipital region |
| Supraorbital nerve (V1) | Forehead, frontal scalp |
| Supratrochlear nerve (V1) | Medial forehead |
| Auriculotemporal nerve (V3) | Temple, lateral scalp |
| Zygomaticotemporal nerve (V2) | Temporal region |
| Greater auricular nerve | Ear, jaw angle |
A 2024 study found that concurrent occipital nerve blocks + myofascial trigger point injections significantly reduced headache severity compared to occipital nerve block alone (Practical Neurology, 2025).
- Local anesthetic alone: 0.5% bupivacaine or 1-2% lidocaine - preferred for repeated use
- Local anesthetic + corticosteroid: triamcinolone 20-40 mg or methylprednisolone - added for longer duration, especially first few treatments
- Saline alone: also shown to have some benefit (possibly from mechanical effect)
2. TRIGGER POINT INJECTIONS (TPIs)
- Mechanical effect of the needle disrupts contracted muscle fibers
- Releases substance P and CGRP causing vasodilation and relief of local ischemia
- Activates Aβ and Aδ fibers
- Engages the endogenous opioid system
- Relieves referred pain via peripheral nerve blockade effect
- Identify active trigger points by palpation (taut bands, jump sign, referred pain)
- Insert needle into trigger point; a local twitch response confirms placement
- Inject 0.5-1 mL local anesthetic (lidocaine 1% or bupivacaine 0.25%) per point
- Multiple points can be injected per session
- Ultrasound guidance can be used for precise localization (especially for deeper muscles)
- Local anesthetic (most common - lidocaine, bupivacaine)
- Saline
- Corticosteroid (short-acting for acute flares)
- Dry needling (no injectate - see below)
3. DRY NEEDLING
- Evidence: A 2023 systematic review showed dry needling had a 93% success rate for reducing headache frequency and orofacial pain from myofascial trigger points - higher than anesthetic injections (83.7%)
- Advantage: no drug-related adverse effects; can be repeated frequently
- Often performed by physiotherapists trained in dry needling
- Targets: temporalis, trapezius, suboccipital muscles, sternocleidomastoid
- A 2024 RCT (Monti-Ballano et al.) specifically confirmed dry needling efficacy on active myofascial trigger points in TTH
4. SPHENOPALATINE GANGLION (SPG) BLOCK
- Patient placed supine, nose pointed at ceiling
- Cotton applicator soaked in 2-4% lidocaine inserted into the nostril toward the posterior nasopharynx
- A slow drip of 2-4 mL lidocaine over 2-4 minutes allows the anesthetic to flow by gravity to the SPG
- Can also be delivered via a small intranasal catheter device
- Non-invasive / minimally invasive
- Can be self-administered by trained patients
- No needles required in the transnasal form
5. BOTULINUM TOXIN (OnabotulinumtoxinA) INJECTIONS
- OnabotulinumtoxinA (Botox) is FDA-approved for chronic migraine (PREEMPT protocol)
- For chronic TTH, evidence is mixed - the 2024 VA/DoD Clinical Practice Guideline found it did not show statistically significant benefit compared to placebo for chronic TTH as a group
- However, it remains useful in select patients with prominent myofascial/muscular component - particularly those with both migraine and TTH overlap, or when significant muscle hypertonia is identified
- Goldman-Cecil Medicine notes it "can be useful" for TTH (p. 3817)
6. NEUROMODULATION DEVICES (Non-invasive)
| Device | Mechanism | Evidence in TTH |
|---|---|---|
| Transcutaneous supraorbital neurostimulation (tSNS) - Cefaly device | Stimulates supraorbital nerve (V1) | Some evidence for TTH prevention; FDA-cleared |
| Transcranial magnetic stimulation (TMS) | Non-invasive cortical modulation; reduces central sensitization | Limited evidence; investigational for TTH |
| Transcranial direct current stimulation (tDCS) | Low-intensity direct current modulates cortical excitability | Emerging evidence; not yet standard of care |
| Transcutaneous electrical nerve stimulation (TENS) | Applied to pericranial muscles/nerves | Evidence for short-term pain reduction; widely available |
| Vagus nerve stimulation (non-invasive, gammaCore) | Modulates trigeminovascular system via vagal afferents | Approved for cluster headache; limited TTH data |
7. OCCIPITAL NERVE STIMULATION (ONS) - Invasive Neuromodulation
- Reserved for the most refractory, disabling chronic TTH that has failed all other treatments
- Modulates central pain processing via the trigeminocervical complex
- Evidence in TTH is limited compared to its use in chronic migraine; however, case series support benefit in carefully selected patients
- Significant risks: lead migration, infection, battery replacement
Summary Table
| Procedure | Indication | Evidence Level | Repeatability |
|---|---|---|---|
| Greater occipital nerve block | Refractory TTH, occipital-predominant | Moderate | Every 4-8 weeks |
| Pericranial multi-nerve block | Chronic/refractory TTH | Moderate | Every 4-8 weeks |
| Trigger point injection | TTH with myofascial trigger points | Moderate | Every 4-6 weeks |
| Dry needling | TTH with myofascial trigger points | Moderate-Good | Weekly/biweekly |
| SPG block (transnasal) | Refractory/acute TTH | Limited-Moderate | As needed/scheduled |
| Botulinum toxin | Refractory chronic TTH with muscle component | Limited (TTH-specific) | Every 3 months |
| TENS / tSNS (Cefaly) | Episodic/chronic TTH | Limited | Daily/as needed |
| Occipital nerve stimulation | Refractory chronic TTH, all else failed | Limited (case series) | Permanent implant |