Tell me about the leprosy in detail microbiology aspect exam oriented
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the detailed exam-oriented answer.
Leprosy (Hansen's Disease) - Detailed Microbiology (Exam-Oriented)
1. THE ORGANISM - Mycobacterium leprae
| Feature | Detail |
|---|---|
| Kingdom/Type | Gram-positive (by cell wall chemistry), acid-fast bacillus |
| Morphology | Straight or slightly curved rod, 1-8 µm long, 0.3-0.5 µm wide |
| Arrangement | Found in clumps called "globi" inside macrophages (lepromatous form) |
| Culture | Cannot be cultured in vitro (absolute obligate intracellular pathogen) - classic exam fact |
| Animal models | Grows in nine-banded armadillo (ideal model, 32-34°C body temp); also in mouse foot pads and nude mice |
| Temperature | Replicates best at 32-34°C (body surface temperature) - explains distribution on cool skin, nose, ears, testes |
| Staining | Acid-fast bacillus - but uses Fite stain (not standard Ziehl-Neelsen) because M. leprae is more sensitive to decolorization than M. tuberculosis |
| Doubling time | ~12-14 days - the slowest dividing bacterium known |
| Cell wall | Contains PGL-1 (phenolic glycolipid-1) - key virulence factor; enables invasion of Schwann cells and binding to laminin of peripheral nerve axons |
| Species note | M. lepromatosis (proposed 2008) - rarely causes diffuse lepromatous leprosy (mainly Mexico, Caribbean) |
2. EPIDEMIOLOGY
- Reservoir: Humans (primary); nine-banded armadillos (in Southern USA, South America); wild squirrels and certain primates
- Transmission: Nasal droplets from untreated multibacillary cases (primary route); skin contact through wounds/tattoos possible; NOT highly contagious
- Incubation period: Average 2-7 years; can be up to 40 years (longest incubation period of any bacterial disease)
- Endemic regions: India, Brazil, Indonesia account for ~80% of global burden
- Current burden: ~200,000 new cases/year globally (down from 5.2 million in 1985 due to MDT)
- WHO elimination target: <1 case per 10,000 population - achieved globally in 2000
- Children: ~8% of new cases; rare in children <5 years; age distribution bimodal (teens and adults)
3. PATHOGENESIS
Entry and Primary Target
- M. leprae enters via respiratory tract (primary) or skin breach
- Disseminates through blood and lymphatics
- Primary target = Schwann cells (glial cells of peripheral nervous system)
- PGL-1 + laminin-binding protein mediate invasion of Schwann cells and binding to peripheral nerve basal lamina
- This causes demyelination of peripheral sensory nerves → anesthesia
Virulence Mechanisms (Exam High-Yield)
- Cannot be cultured in vitro - absolute obligate intracellular
- Secretes no toxins - virulence is through cell wall components
- Inhibits mitochondrial energy metabolism to evade host immune response
- BCG vaccination offers partial cross-protection (similar cell wall to M. tuberculosis)
The Immunologic Spectrum - KEY EXAM CONCEPT
The entire spectrum of leprosy depends on the host Th1 vs Th2 response:
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| CMI | Strong Th1 | Weak Th1 / Th2 predominant |
| CD4+ T cells | Abundant | Scarce |
| CD8+ T cells | Few | Numerous |
| Cytokines | IL-2, IFN-γ (Th1) | IL-4, IL-5, IL-10 (Th2) |
| Bacterial load | Paucibacillary (few/no AFB) | Multibacillary (many AFB) |
| Granulomas | Well-formed, with giant cells | Poorly formed / absent |
| Macrophages | Epithelioid, activated (M1) | Foamy (lipid-laden), deactivated |
| Lepromin test | Positive | Negative |
| Antibodies | Low | High (but non-protective - form immune complexes) |
| Contagiousness | Low (non-contagious) | High (contagious) |
4. RIDLEY-JOPLING CLASSIFICATION (1962) - Exam Classic
Five overlapping categories on a spectrum:
TT ←→ BT ←→ BB ←→ BL ←→ LL
(tuberculoid) (lepromatous)
Strong CMI ←————————→ Weak CMI
- TT = Tuberculoid (polar, stable)
- BT = Borderline tuberculoid
- BB = Mid-borderline (unstable, rare - rapidly shifts toward BL)
- BL = Borderline lepromatous
- LL = Lepromatous (polar, stable)
- IL = Indeterminate leprosy (early, not yet classified)
WHO Simplified Classification (for field use):
| WHO Type | Definition | Skin Lesions | Nerves |
|---|---|---|---|
| Paucibacillary (PB) | Smear negative at all sites | 1-5 lesions | ≤1 nerve trunk |
| Multibacillary (MB) | Smear positive at any site | >5 lesions | >1 nerve trunk |
5. MORPHOLOGY / HISTOPATHOLOGY
Tuberculoid Leprosy
- Skin: Flat red lesions → enlarge with indurated, elevated, hyperpigmented margins and depressed, pale, hairless centers (central healing)
- Histology: Well-formed granulomas - epithelioid cells + Langhans giant cells + lymphocyte infiltration (resembles TB granuloma)
- Nerves: Enclosed within granulomatous reaction; small peripheral twigs can be completely destroyed → sensory loss
- AFB: Almost none visible → "paucibacillary"
- The presence of granulomas + absence of bacteria = reflects strong T-cell immunity
Lepromatous Leprosy
- Skin: Macular/papular/nodular lesions on face, ears, wrists, elbows, knees; diffuse symmetric thickening
- Facies: "Leonine facies" - nodular lesions coalesce giving lion-like appearance; loss of eyebrows (madarosis)
- Histology: Large aggregates of lipid-laden foamy macrophages = "Lepra cells" (Virchow cells) filled with masses ("globi") of AFB
- Nerves: Symmetric invasion of ulnar and peroneal nerves by mycobacteria; minimal inflammation despite massive bacillary load
- Other sites: Testes (destruction of seminiferous tubules → sterility); anterior eye; upper airways; lymph nodes (paracortical foamy macrophages)
- AFB: Abundant → "multibacillary"
- Vital organs/CNS usually spared (temperature too high for M. leprae)
Histopathology Images (Robbins Pathology):
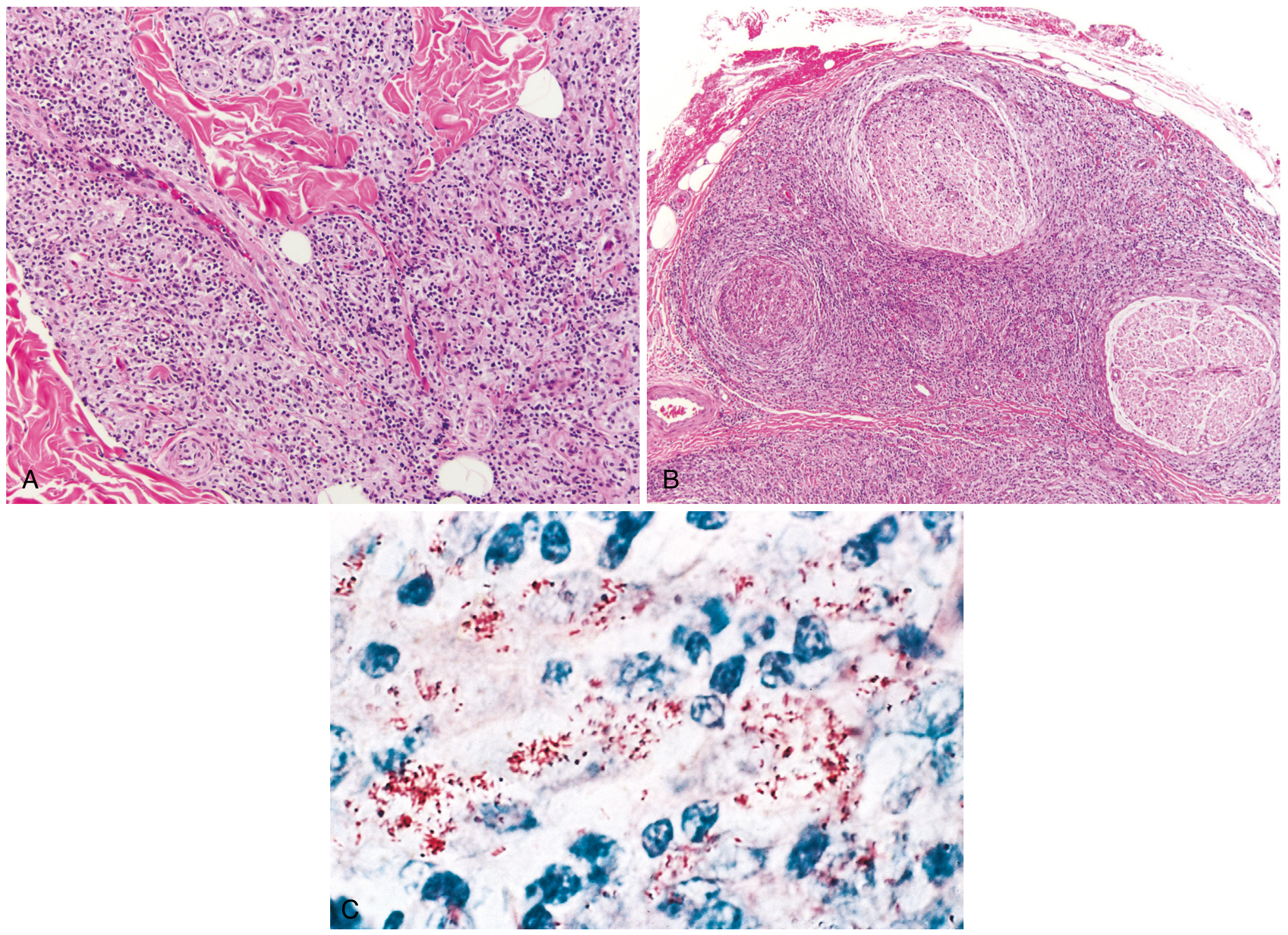
(A) Dense dermal macrophage infiltration surrounding adnexa, vessels, and nerves in lepromatous leprosy; (B) Dense chronic lymphocytic and macrophage infiltration into large nerve bundles in tuberculoid leprosy; (C) Acid-fast bacilli (red) within macrophages - lepromatous form
Clinical Lepromatous Leprosy:
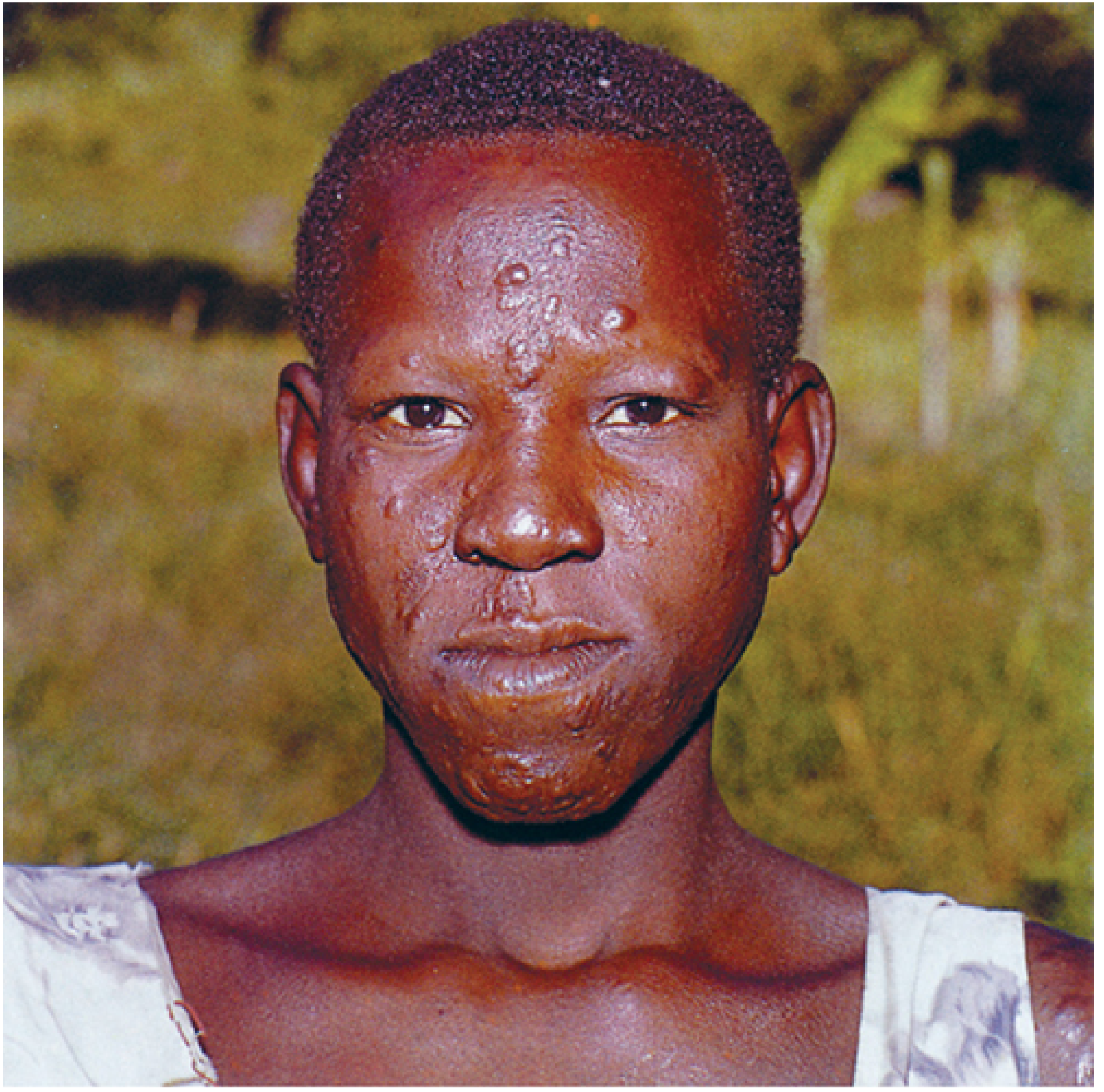
Lepromatous leprosy - note cutaneous plaques, infiltrates, and loss of eyebrows (madarosis)
6. CLINICAL FEATURES - Cardinal Signs (WHO)
Diagnosis requires ONE or more of these:
- Hypopigmented/erythematous skin patch with definite loss of sensation
- Thickened peripheral nerve (with or without tenderness)
- Positive slit-skin smear for AFB (Fite stain)
7. LABORATORY DIAGNOSIS
| Test | Details |
|---|---|
| Slit-skin smear | Smear from ear lobe, nasal mucosa, or skin lesion; Fite stain (modified AFB); use this not ZN - M. leprae is more acid-labile |
| Bacteriological Index (BI) | Logarithmic scale 0-6+ for bacillary load on slit-skin smear |
| Morphological Index (MI) | % of solid-staining (viable) bacilli |
| Skin biopsy | Full-thickness biopsy showing granulomas (tuberculoid) or foamy macrophages with AFB (lepromatous) |
| Culture | NOT POSSIBLE in vitro - classic exam question |
| Animal inoculation | Mouse foot pad; nine-banded armadillo |
| Lepromin (Mitsuda) test | Skin test using killed M. leprae; NOT a diagnostic test; measures CMI status |
| PCR | Detects M. leprae DNA; useful for paucibacillary and doubtful cases |
| Anti-PGL-1 antibody (ELISA) | Detects antibodies to phenolic glycolipid-1; elevated in lepromatous; not useful for paucibacillary |
8. LEPROMIN (MITSUDA) TEST - Exam High-Yield
What it is: Intradermal injection of heat-killed M. leprae (lepromin antigen)
Two reactions:
| Reaction | Timing | Size (positive) | Significance |
|---|---|---|---|
| Fernandez reaction (early) | 48-72 hours | >10 mm erythema | Measures delayed hypersensitivity (DTH); similar to tuberculin |
| Mitsuda reaction (late) | 3-4 weeks | >3-5 mm nodule | Measures cell-mediated immunity (CMI); more clinically significant |
Key facts:
- NOT a diagnostic test (positive in healthy non-cases; negative in lepromatous)
- Used to classify leprosy and assess prognosis (CMI status)
- Positive in TT, negative in LL
- BCG vaccination can convert lepromin-negative to positive
- First 6 months of life: most children are lepromin-negative
9. IMMUNITY
| Aspect | Detail |
|---|---|
| Primary immunity | T-cell mediated (CMI) - not humoral |
| Th1 → tuberculoid | IL-2, IFN-γ produced → activates macrophages (M1) → kills bacilli |
| Th2/regulatory T cells → lepromatous | Weak CMI; humoral response predominates; antibodies non-protective |
| IFN-γ role | Same as in TB - mobilizes effective macrophage response; low bacterial burden |
| Immune complexes | In lepromatous: antibody + free antigens → erythema nodosum leprosum (ENL), vasculitis, glomerulonephritis (Type III reaction) |
| BCG vaccination | Provides partial cross-protection against M. leprae |
10. LEPROSY REACTIONS (Immunological Complications)
| Reaction | Type | Form | Mechanism |
|---|---|---|---|
| Type 1 (Reversal reaction) | Delayed hypersensitivity (Type IV) | Borderline (BT, BB, BL) | Sudden increase in CMI → inflammation in existing lesions and nerves |
| Type 2 - ENL (Erythema Nodosum Leprosum) | Immune complex (Type III) | Lepromatous/BL | Antigen-antibody complexes → complement activation → tender nodules, fever, neuritis |
11. TREATMENT (WHO MDT - Multi-Drug Therapy)
| Regimen | Disease | Drugs | Duration |
|---|---|---|---|
| Paucibacillary | 1-5 lesions | Dapsone + monthly Rifampicin | 6 months |
| Multibacillary | >5 lesions | Dapsone + Clofazimine + monthly Rifampicin | 12 months |
Mechanisms:
- Dapsone (sulfone): Blocks PABA metabolism in M. leprae (like sulfonamides in bacteria)
- Rifampicin: Inhibits RNA polymerase - most bactericidal drug
- Clofazimine: Binds DNA; also anti-inflammatory
12. QUICK-FIRE EXAM MNEMONICS
"CAFE" for cardinal signs: Cutaneous patch, Anesthesia, Fiber (nerve thickening), Evidence (AFB smear positive)
Tuberculoid vs Lepromatous - remember "PALE vs FULL":
- Tuberculoid = Pauci-bacillary, Anesthetic lesions, Low organisms, Epitheloid granulomas
- Lepromatous = Foamy macrophages, Unlimited bacteria, Leonine facies, Loss of eyebrows
Lepromin test: NOT for Diagnosis, YES for Classification and Prognosis
13. KEY EXAM FACTS SUMMARY
| Fact | Answer |
|---|---|
| Causative agent | Mycobacterium leprae |
| Cannot be cultured | In vitro - only animal models (armadillo, mouse foot pad) |
| Primary target in nerve | Schwann cells |
| Optimal temperature | 32-34°C |
| Slowest dividing bacterium | M. leprae (~12-14 day doubling time) |
| Stain used | Fite stain (not ZN) |
| Smear from | Ear lobe / nasal mucosa / slit-skin |
| Lepromin test is | NOT diagnostic - measures CMI, used for classification |
| Paucibacillary treatment | Dapsone + Rifampicin × 6 months |
| Multibacillary treatment | Dapsone + Clofazimine + Rifampicin × 12 months |
| Lepra cells | Foamy macrophages in lepromatous leprosy (Virchow cells) |
| Globi | Masses of AFB inside macrophages |
| Longest incubation | Up to 40 years (average 2-7 years) |
| Leonine facies | Lepromatous leprosy |
| ENL reaction type | Type III (immune complex) |
| Type 1 reaction type | Type IV (DTH) - borderline forms |
Sources: Sherris & Ryan's Medical Microbiology 8e | Robbins, Cotran & Kumar Pathologic Basis of Disease | Harrison's Principles of Internal Medicine 22e | Park's Preventive & Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.