Sarcoidosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
sarcoidosis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple top-tier textbooks. I have everything needed to write a thorough, well-structured answer on sarcoidosis.
Sarcoidosis
Definition and Overview
Sarcoidosis is a systemic, multi-organ granulomatous disease of unknown etiology, defined by the presence of noncaseating epithelioid cell granulomas at sites of disease. While any organ can be affected, the lungs and intrathoracic lymph nodes are involved in more than 90% of cases. Like syphilis, it is classically called a "great imitator" because of its widely variable presentations. - Fishman's Pulmonary Diseases and Disorders, p. 922
Epidemiology
- More common in women and African Americans in the United States (African Americans are affected at a rate 3-4x that of White Americans)
- Peak incidence in adults aged 20-40 years; a second peak occurs in women over 50
- Global variation: Scandinavian countries have some of the highest reported rates worldwide
- Organ involvement data from two large U.S. cohorts (n=2700):
| Organ | Frequency |
|---|---|
| Lungs | ~89% |
| Eye | 23-33% |
| Skin | 32-33% |
| Liver | 13-20% |
| Neurologic | 9-14% |
| Cardiac | 4-5% |
Etiology and Pathogenesis
The exact cause remains unknown. The current leading hypothesis is that sarcoidosis results from gene-environment interactions: certain microbial antigens (particularly from mycobacterial or propionibacterial organisms) trigger a disproportionate immune response in genetically susceptible individuals.
Key pathogenic elements:
- Genetic susceptibility: HLA-DRB1 alleles strongly implicated; GWAS studies (the GRADS study) identified multiple genetic associations
- Immune dysregulation: Polarization toward a Th1 (and Th17) immune response with excessive TNF-alpha, IL-2, and IFN-gamma production
- Antigen-driven inflammation: Serum amyloid A accumulation within granulomas is hypothesized to sustain chronic disease
- Autoimmune features: Low-titer ANAs, rheumatoid factor, and hypergammaglobulinemia can be present, though no disease-specific autoantibody has been identified
- TGF-beta and mTOR pathways correlate with parenchymal (fibrotic) involvement; IL-7 + IL-2 correlate with airway involvement - Fishman's, p. 924
Histopathology - The Cornerstone
The pathologic hallmark is the discrete, noncaseating epithelioid cell granuloma:
- Central core: Epithelioid cells (differentiated mononuclear phagocytes) + CD4+ T lymphocytes + mature macrophages
- Periphery: CD4+, CD8+ T cells, and B lymphocytes
- Giant cells with cytoplasmic inclusions:
- Schaumann bodies (calcium- and iron-laden)
- Hamazaki-Wesenberg bodies
- Focal fibrinoid necrosis is acceptable; caseating (cheese-like) necrosis is NOT a feature of sarcoidosis - its presence mandates exclusion of tuberculosis and fungal infection
- In the lung, granulomas cluster along lymphatic routes (peribronchial, perivascular, and subpleural)
Photomicrographs of noncaseating granulomatous inflammation:
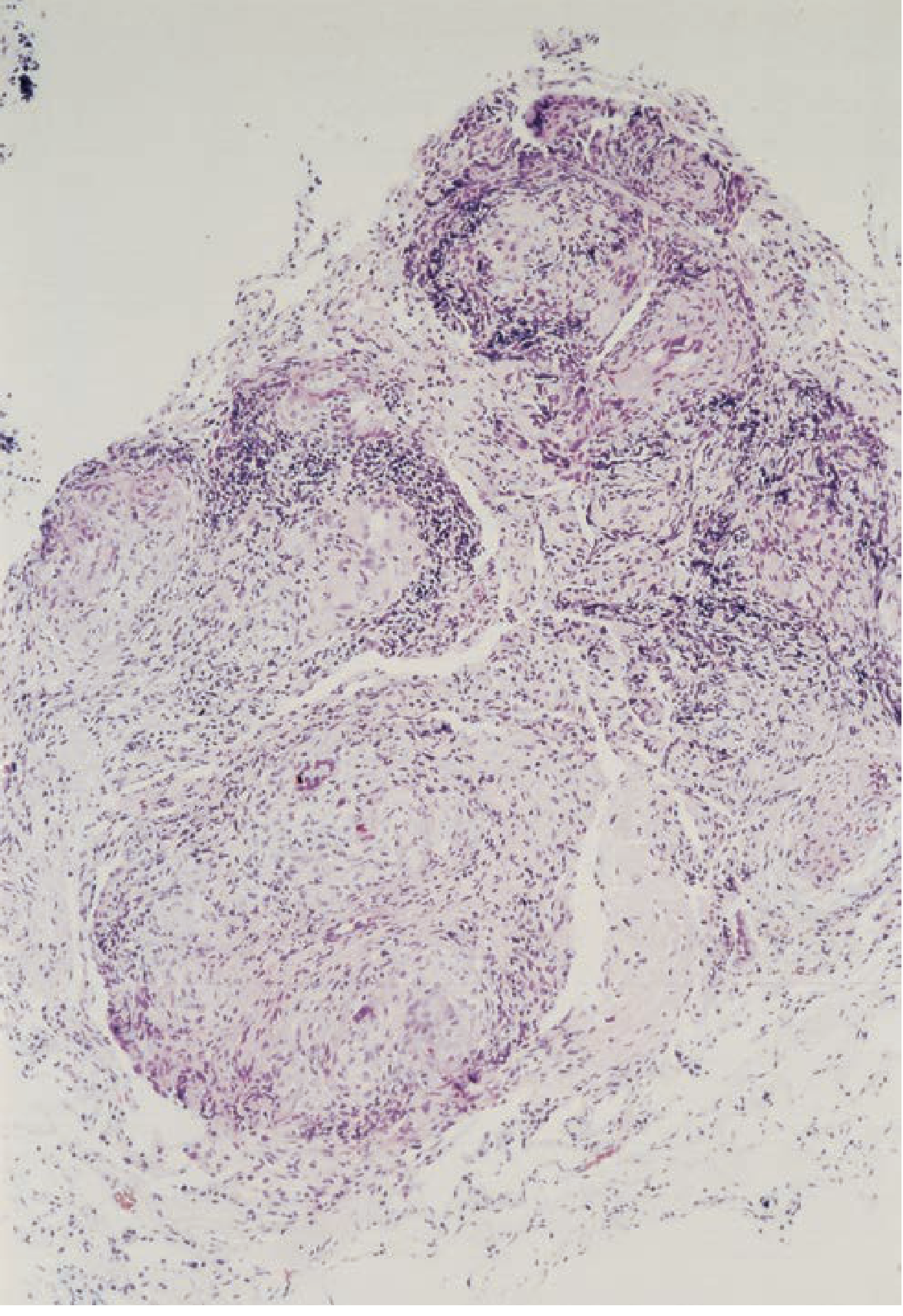
Fig. A - Thoracoscopic lung biopsy (×80): extensive granulomatous inflammation with multinucleated giant cells
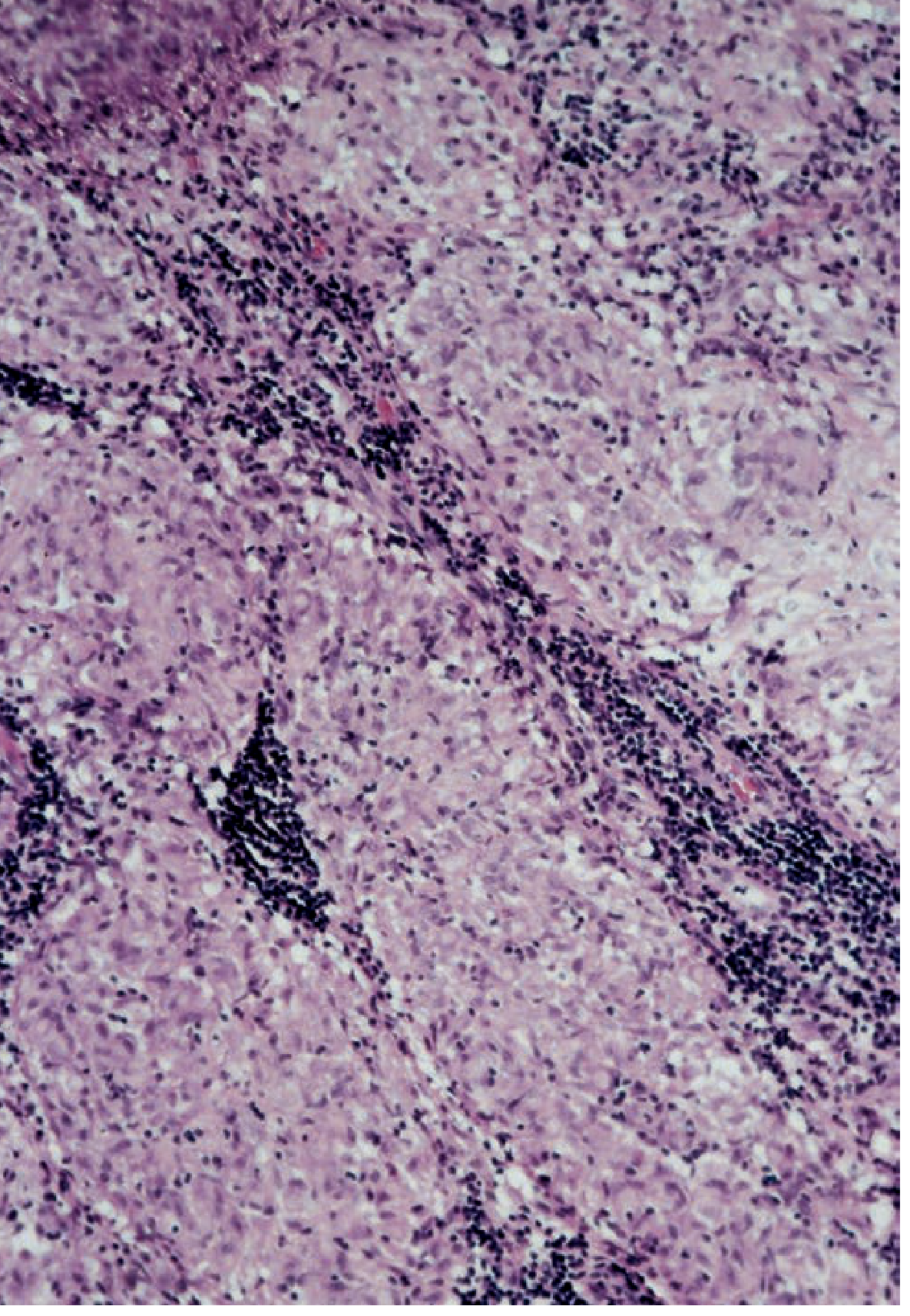
Fig. B - Mediastinal lymph node biopsy (×200): classic discrete epithelioid granulomas
Clinical Features
Constitutional (>50%)
Fever, night sweats, malaise, excessive fatigue, unintentional weight loss. Fatigue is reported by >50% of patients in Europe and the U.S. and may persist long after other disease evidence has regressed.
Pulmonary (>90%)
- Dyspnea and dry cough are most common
- Restrictive or obstructive impairment, reduced diffusing capacity (DLCO)
- Fibrocystic disease, pulmonary hypertension, bronchiectasis
- Tracheal/bronchial stenosis, cavitating nodules, mycetomas
Radiographic staging (Scadding stages):
| Stage | Chest X-ray Findings | Spontaneous Remission |
|---|---|---|
| 0 | Normal | - |
| I | Bilateral hilar lymphadenopathy (BHL) only | ~80% |
| II | BHL + pulmonary infiltrates | ~50-60% |
| III | Pulmonary infiltrates only (no BHL) | ~30% |
| IV | Pulmonary fibrosis | Rare |
Skin (20-30%)
- Erythema nodosum (tender red nodules on shins): part of Löfgren syndrome (acute sarcoidosis with excellent prognosis)
- Lupus pernio: indurated, violaceous plaques on nose, cheeks, ears, lips - highly associated with chronic disease and pulmonary granulomatous infiltration of the upper airway
- Scar granulomas, tattoo infiltration, alopecia
- Classic lesions are red-brown, non-scaly papules/plaques on the face around nose and mouth - Textbook of Family Medicine, p. 481
Ocular (23-33%)
- Anterior uveitis is most common (acute, painful with red eye)
- Posterior uveitis, panuveitis, chorioretinitis
- Heerfordt syndrome (uveoparotid fever): fever + parotid enlargement + facial palsy + uveitis + bilateral hilar adenopathy
Cardiac (4-5%, but up to 25% at autopsy)
- Complete heart block and ventricular arrhythmias are the leading causes of sudden death
- Cardiomyopathy, pericardial effusion
- FDG-PET is the most sensitive imaging tool for active cardiac sarcoidosis
- Cardiac involvement warrants ECG, echocardiography, and cardiac MRI or FDG-PET evaluation
Neurologic (9-14%)
- CN VII palsy (facial nerve) is most common
- Aseptic meningitis, optic neuropathy, hypothalamic/pituitary insufficiency
- Sarcoidosis can involve the optic chiasm, causing blindness
Musculoskeletal
- Löfgren syndrome: erythema nodosum + bilateral hilar adenopathy + periarticular ankle inflammation
- Lytic bone lesions (punched out lesions on X-ray, especially small bones of hands/feet)
- Myopathy: rare, but may present with elevated CK
Calcium Metabolism
- Hypercalciuria (more common) and hypercalcemia (up to 30% of patients)
- Mechanism: autonomous 1-alpha-hydroxylase activity in macrophages and epithelioid cells converts 25(OH)D to active 1,25(OH)2 vitamin D3
- Consequences: nephrocalcinosis, kidney stones, renal failure
Hepatic/Splenic
- Elevated alkaline phosphatase (more than transaminases)
- Liver biopsy positive for granulomas in most patients even without symptoms
- End-stage hepatic fibrosis is uncommon
Diagnosis
Diagnosis requires:
- Compatible clinical + radiographic presentation
- Histological confirmation: noncaseating epithelioid granulomas in ≥1 organ
- Exclusion of other granulomatous diseases (TB, fungal infections, berylliosis, foreign body reactions, Crohn's disease)
Investigations
| Test | Findings in Sarcoidosis |
|---|---|
| Chest X-ray / HRCT | BHL, perilymphatic nodules, upper lobe fibrosis |
| Serum ACE | Elevated (~60%); not specific |
| Serum calcium / 24h urine calcium | Elevated |
| LFTs | Raised ALP |
| FBC | Lymphopenia, anaemia |
| BAL | CD4:CD8 ratio >3.5 (normal ~2) |
| Serum soluble IL-2 receptor | Elevated; correlates with disease activity |
| SPEP | Hypergammaglobulinemia |
Biopsy Sites (in order of preference)
- Transbronchial biopsy (yield ~70-90% if lung involved)
- EBUS-guided sampling of mediastinal lymph nodes (high yield)
- Skin lesions (easy, high yield when present)
- Liver (high granuloma prevalence even when asymptomatic)
- Avoid biopsy: erythema nodosum (yield low, nonspecific)
FDG-PET
Useful for: identifying extrapulmonary disease sites for biopsy, assessing treatment response (especially cardiac and neurosarcoidosis) - Fishman's, p. 933
Complications
Sarcoidosis-Associated Pulmonary Hypertension (SAPH)
- Overall incidence: 5-15% in all sarcoidosis patients
- In moderate-to-severe pulmonary disease, rates are much higher
- Mechanisms: LV diastolic dysfunction, pulmonary arterial vasculitis, pulmonary veno-occlusive disease, fibrosis, hypoxia - Murray & Nadel's, p. 2131
Aspergilloma
- Forms in cavities created by fibrocystic sarcoidosis
- Can cause life-threatening hemoptysis
Fibrotic Sarcoidosis (Stage IV)
- Progressive fibrosis leading to honeycombing, traction bronchiectasis
- Carries the worst prognosis
Treatment
Treatment is indicated for:
- Threatened organ function (eye, heart, brain, kidney)
- Progressive pulmonary disease
- Hypercalcemia
- Significant systemic symptoms
Treatment Ladder
| Agent | Role | Grade |
|---|---|---|
| Corticosteroids (prednisone 20-40 mg/day) | First-line; acute and chronic disease | 1A/1B |
| Methotrexate | Steroid-sparing; chronic disease | 1A |
| Azathioprine | Steroid-sparing; chronic disease | 1B |
| Leflunomide | Steroid-sparing; chronic disease | 1B |
| Hydroxychloroquine | Skin/hypercalcemia; mild disease | 2B |
| Infliximab (anti-TNF) | Refractory disease | 1A |
| Adalimumab (anti-TNF) | Refractory disease | 1A |
| Mycophenolate | Steroid-sparing | 1C |
For complications:
- SAPH: Bosentan (1A), sildenafil (1B), inhaled iloprost (2B), prostacyclin (1B)
- Fatigue: d-methylphenidate (1A), armodafinil (1A)
- Lung transplantation: For end-stage fibrotic disease (Stage IV)
Important: A 2025 systematic review and meta-analysis in Thorax (PMID 40393718) evaluated biologic and targeted synthetic therapies in sarcoidosis, providing updated evidence on anti-TNF agents and other biologics that may refine current treatment algorithms.
Note: Not all patients require treatment. Many (especially Stage I with Löfgren syndrome) undergo spontaneous remission and should be observed.
Prognosis and Course
| Presentation | Likely Course |
|---|---|
| Löfgren syndrome | Excellent; ~80-90% remission |
| Stage I (BHL only) | ~80% spontaneous remission |
| Stage II | ~50-60% spontaneous remission |
| Stage III | ~30% spontaneous remission |
| Stage IV (fibrosis) | Rarely remits; progressive |
| African American patients | More likely to have chronic/severe disease |
| Cardiac sarcoidosis | Risk of sudden cardiac death |
Sarcoidosis-related mortality is approximately 1-5% in the U.S., most commonly from respiratory failure, cardiac involvement, or neurosarcoidosis. Quality of life is significantly impaired in many patients, with fatigue being a persistent, often underappreciated burden. - Murray & Nadel's, p. 2131
Sources: Fishman's Pulmonary Diseases and Disorders (Chapter 53); Murray & Nadel's Textbook of Respiratory Medicine (Chapter 93); Textbook of Family Medicine 9e; Andrews' Diseases of the Skin
This is a shared conversation. Sign in to Orris to start your own chat.