MBBS Essay OBG Endometrial Cancer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from authoritative textbooks plus the histology images. Let me compile the full MBBS-level essay.
Endometrial Cancer
MBBS Essay - Obstetrics & Gynaecology
Definition
Endometrial carcinoma is a malignant neoplasm arising from the epithelial lining of the uterine body (endometrium). It is the most common malignancy of the female genital tract, accounting for nearly half of all gynaecologic cancers and ~7% of all invasive cancers in women (excluding skin cancer).
- Berek & Novak's Gynecology, p. 2141
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 932
Epidemiology
- Predominantly a disease of postmenopausal women; peak incidence in the 6th-7th decade, average age at diagnosis ~60 years
- 75% of cases occur in women over 50 years of age
- Overall lifetime risk: approximately 2.8% of women
- Overall 5-year survival rate: approximately 75%
- Deaths from endometrial carcinoma rose ~2% per year from 2010 to 2014, reflecting an increasing burden
- Berek & Novak's Gynecology, p. 2141
Pathogenesis: Two Major Types
There are two well-defined pathogenetic types of endometrial carcinoma:
| Feature | Type I (Endometrioid) | Type II (Non-Endometrioid) |
|---|---|---|
| Frequency | 75-85% | 15-25% |
| Estrogen | Estrogen-dependent | Estrogen-independent |
| Background | Endometrial hyperplasia | Atrophic endometrium |
| Histology | Endometrioid adenocarcinoma | Serous, clear cell |
| Grade | Well-differentiated (low grade) | Poorly differentiated (high grade) |
| Prognosis | Favorable | Poor |
| Patient | Obese, younger, perimenopausal | Thin, older, postmenopausal |
| Racial predominance | Any | Disproportionate in African American, Asian women |
- Berek & Novak's Gynecology, p. 2141
Risk Factors
All major risk factors relate to prolonged, unopposed estrogen stimulation of the endometrium:
High-risk factors:
- Obesity - adipose tissue converts androgens to estrone (peripheral aromatization); major risk in Western populations
- Nulliparity
- Late menopause (after age 52)
- Unopposed exogenous estrogen therapy - risk increased 4 to 8 times; risk increases with duration and dose
- Tamoxifen use (weak estrogen agonist on endometrium)
- Polycystic ovarian syndrome (PCOS)
- Estrogen-secreting tumours (granulosa cell tumours)
- Type 2 diabetes mellitus, hypertension - commonly co-occur with obesity
Hereditary risk:
- Lynch syndrome (Hereditary Non-Polyposis Colorectal Cancer - HNPCC) - mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, PMS2); lifetime endometrial cancer risk up to 40-60%
- Cowden syndrome (PTEN hamartoma tumour syndrome)
Protective factors:
-
Combined oral contraceptive pill use (reduces risk by ~50%)
-
Progestogen therapy (opposes estrogenic stimulation)
-
Multiparity
-
Smoking (paradoxically reduces risk via anti-estrogenic effects - not recommended)
-
Physical activity
-
Berek & Novak's Gynecology, p. 2141; Robbins, p. 932
Molecular Pathogenesis
Genomic sequencing has revealed four major molecular subtypes:
- Ultramutated / POLE tumours - Mutations in DNA polymerase epsilon (POLE); exceptionally high somatic mutation burden; paradoxically good prognosis
- Hypermutated / MSI (Microsatellite Instability) - Mutations or epigenetic silencing of DNA mismatch repair genes (MLH1 promoter hypermethylation most common); ~20% of sporadic tumours; associated with Lynch syndrome
- Copy number low / Non-specific molecular phenotype - Common subtype; associated with endometrioid morphology; multiple mutations upregulating PI3K/AKT pathway (PTEN, PIK3CA, KRAS, ARID1A)
- Copy number high / TP53 mutated - Aggressive tumours with serous or high-grade endometrioid morphology; TP53 mutations >90% of serous carcinomas; worst prognosis
Key mutations in endometrioid carcinoma:
-
PTEN - most frequently mutated gene (30-80%)
-
PIK3CA - activating mutations (~40%)
-
KRAS - (~25%)
-
ARID1A - loss of function (~33%)
-
TP53 - late event; found in ~50% of poorly differentiated tumours
-
Robbins, p. 932-933
Precursor Lesion: Endometrial Hyperplasia
Endometrial hyperplasia is the recognized precursor to Type I endometrial carcinoma. The WHO classification recognizes:
- Hyperplasia without atypia - Low risk of malignant progression (<5%)
- Atypical hyperplasia (Endometrial Intraepithelial Neoplasia - EIN) - High risk; ~30% progress to carcinoma if untreated; some cases of "atypical hyperplasia" are already carcinoma on hysterectomy specimen
Histologically, identical mutations in PTEN, ARID1A, PIK3CA, KRAS are present in both atypical hyperplasia and adjacent carcinoma in the same uterus, supporting the precursor relationship.
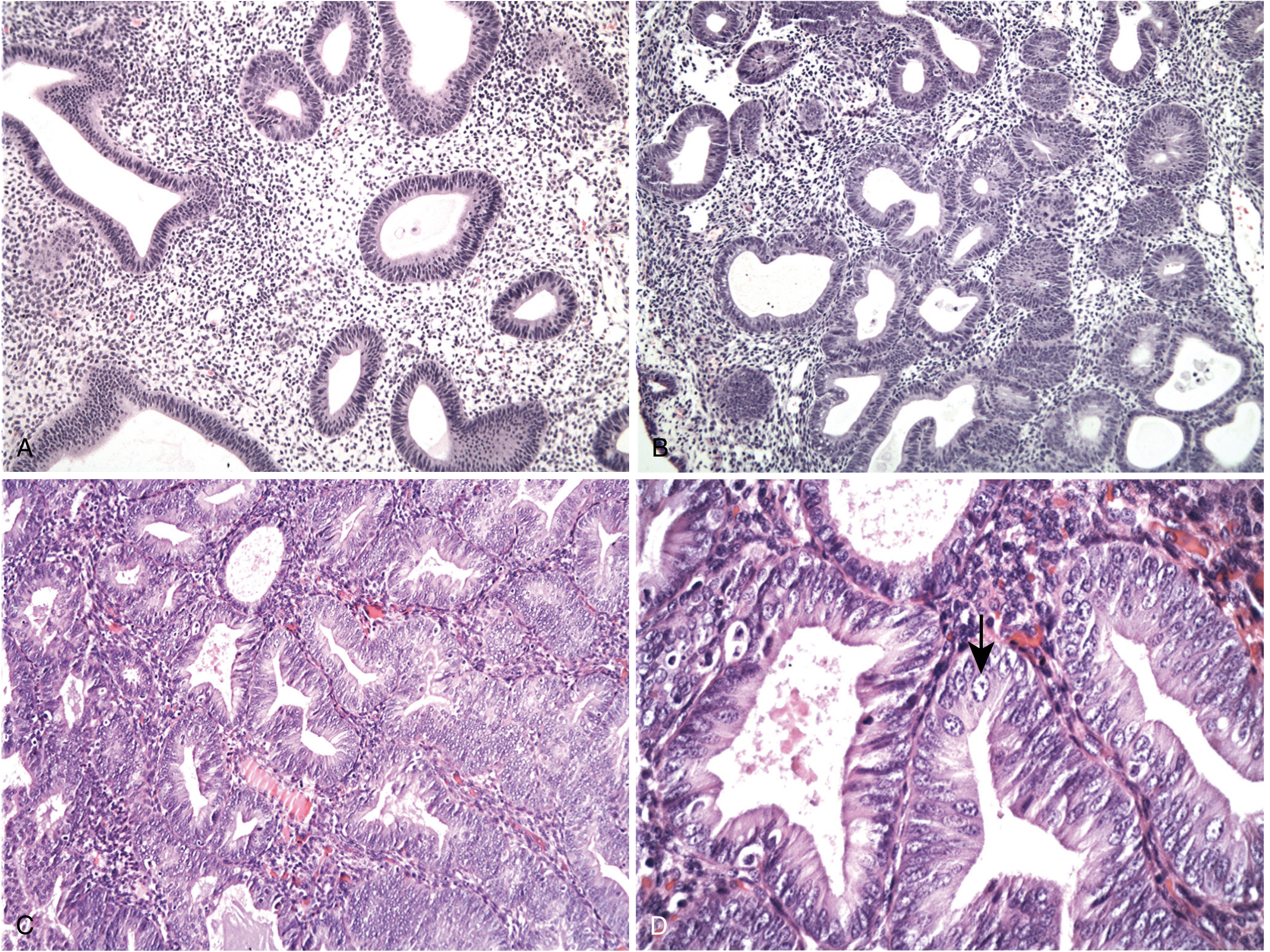
Fig. Endometrial hyperplasia spectrum (H&E) - Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathology / Histological Types
1. Endometrioid Adenocarcinoma (Most Common - 80-85%)
- Arises from endometrial hyperplasia
- Mimics proliferative endometrial glands (hence "endometrioid")
- Histologic grading (FIGO):
- Grade 1 (well-differentiated): <5% non-squamous solid growth
- Grade 2 (moderately differentiated): 6-50% solid areas
- Grade 3 (poorly differentiated): >50% solid growth pattern
- May contain foci of squamous differentiation (up to 20% of cases); graded on glandular component alone
2. Serous Carcinoma (Uterine Papillary Serous Carcinoma - UPSC) (~15%)
- Type II tumour; arises on a background of endometrial atrophy in older women
- Highly aggressive; fibrovascular papillary stalks lined by highly atypical cells with tufting
- Psammoma bodies frequently present
- TP53 mutations >90%
- Despite being <10% of endometrial cancers, accounts for >50% of all endometrial cancer deaths
- Has propensity for intraperitoneal spread even without myometrial invasion (simulates ovarian carcinoma)
- Berek & Novak's Gynecology, p. 2158
3. Clear Cell Carcinoma
- Type II; aggressive tumour; poor prognosis
- Clear cells (glycogen-rich cytoplasm) and hobnail cells
- Also arises in older, postmenopausal women without hyperestrogenism
4. Mucinous Carcinoma
- Rare; most are low-grade and well-differentiated
- Must be distinguished from endocervical carcinoma
5. Mixed Carcinomas
- Combinations of histologic types (especially endometrioid + serous); behave as aggressively as the higher-grade component
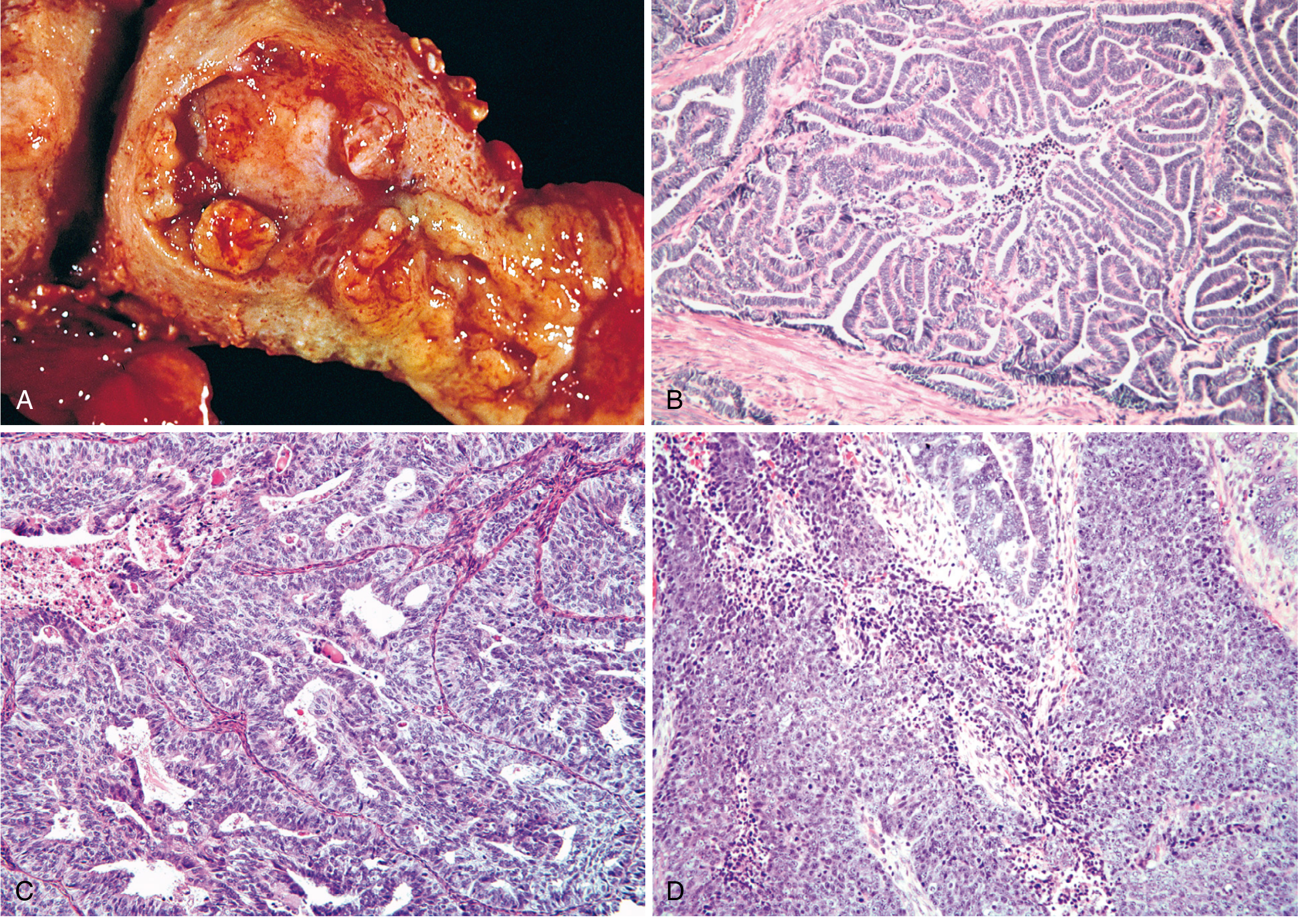
Fig. Endometrioid adenocarcinoma, gross and microscopic grades (Robbins, Cotran & Kumar)
Clinical Features
Symptoms
- Postmenopausal bleeding - cardinal symptom; present in ~90% of patients
- Any postmenopausal bleeding must be investigated until cancer is excluded
- Abnormal perimenopausal bleeding - irregular, heavy
- Pelvic pressure or pain - indicates uterine enlargement or extrauterine spread
- Purulent vaginal discharge - if cervical stenosis causes hematometra/pyometra (poor prognostic sign)
- <5% are asymptomatic (detected incidentally on imaging or Pap smear)
Signs
- Uterine enlargement on bimanual palpation
- In advanced disease: adnexal mass, ascites, inguinal lymphadenopathy
- Pap smear may show malignant cells in ~50% (not a screening test)
Differential Diagnosis of Postmenopausal Bleeding
- Endometrial atrophy (most common, 60-80%)
- Endometrial polyps (2-12%)
- Exogenous estrogen therapy
- Endometrial hyperplasia
- Endometrial carcinoma
- Cervical/vaginal/vulval pathology
- Atrophic vaginitis (up to 15%)
Investigations
Step 1 - Endometrial Biopsy (Gold Standard)
- Office endometrial aspiration biopsy (Pipelle biopsy) - first-line, accepted standard
- Sensitivity for endometrial cancer: ~90-95%
- If inadequate sample or high clinical suspicion: proceed to D&C ± hysteroscopy
Step 2 - Transvaginal Ultrasound (TVS)
- Endometrial thickness:
- >4-5 mm in postmenopausal women is threshold for further investigation
- Atrophic endometrium (<4 mm) makes cancer very unlikely
- A thin endometrial stripe essentially excludes malignancy
Step 3 - Hysteroscopy + Directed Biopsy
- Direct visualization of endometrial cavity
- Best for detecting polyps and focal lesions missed by blind biopsy
- Considered gold standard for diagnosis
Further Workup (Pre-treatment):
- Complete Blood Count, LFT, RFT, blood glucose
- CA-125 (elevated in advanced disease, serous type)
- Chest X-ray, CT chest/abdomen/pelvis - for staging, lymph node assessment, metastases
- MRI pelvis - best modality for assessing depth of myometrial invasion and cervical involvement
- Cystoscopy / Proctoscopy - if bladder/bowel involvement suspected (Stage IVA)
Staging
Endometrial cancer is surgically staged using the FIGO 2009 system (most widely used at MBBS level):
| Stage | Description |
|---|---|
| Stage I | Confined to the uterine body |
| IA | Tumour invades <50% of myometrium |
| IB | Tumour invades ≥50% of myometrium |
| Stage II | Tumour invades cervical stroma, but not beyond uterus |
| Stage III | Local/regional spread |
| IIIA | Tumour invades uterine serosa and/or adnexa |
| IIIB | Vaginal and/or parametrial involvement |
| IIIC1 | Pelvic lymph node metastasis |
| IIIC2 | Para-aortic lymph node metastasis |
| Stage IV | Tumour invades bladder/bowel mucosa, or distant metastases |
| IVA | Bladder/bowel mucosal invasion |
| IVB | Distant metastases (lungs, liver, bone, inguinal lymph nodes) |
Most women (75%) present with Stage I disease due to early symptoms (postmenopausal bleeding).
- Berek & Novak's Gynecology, p. 2141
Prognostic Factors
Adverse prognostic variables:
- Advanced age
- Non-endometrioid histology (serous, clear cell) or Grade 3 histology
- Deep myometrial invasion (≥50%) - Stage IB and beyond
- Lymph-vascular space invasion (LVSI)
- Large tumour size (>2 cm)
- Cervical extension (Stage II)
- Lymph node metastasis (Stage IIIC)
- Intraperitoneal spread
- Positive peritoneal cytology
- Hormone receptor negativity (ER/PR negative tumours behave more aggressively)
- Abnormal DNA ploidy (aneuploidy)
- Berek & Novak's Gynecology, p. 2142
Treatment
Surgical Treatment (Primary)
Surgery is the mainstay of treatment for endometrial carcinoma and serves both therapeutic and staging purposes.
Standard surgical procedure:
- Total Hysterectomy + Bilateral Salpingo-Oophorectomy (TAH+BSO)
- Peritoneal washings/cytology
- Lymph node assessment - pelvic and para-aortic lymph node dissection in most patients
- May be omitted in low-risk patients (Grade 1-2, Stage IA, no LVSI)
- Omentectomy and peritoneal biopsies for serous/clear cell histology
Route of surgery:
- Laparoscopic/robotic-assisted preferred over open laparotomy (comparable oncologic outcomes, faster recovery, lower morbidity)
- Open laparotomy for bulky disease or advanced stages
Fertility-sparing treatment (selected young patients with Stage IA, Grade 1):
- High-dose progestin therapy (medroxyprogesterone acetate / megestrol acetate)
- Close surveillance with serial biopsies
- Hysterectomy recommended after childbearing is complete
Radiotherapy
- Vaginal brachytherapy - for Stage I intermediate/high-intermediate risk; reduces vaginal vault recurrence (up to 80% salvage for isolated vaginal recurrence)
- External Beam Pelvic Radiotherapy (EBRT) - Stage IB high grade, Stage II; decreases pelvic recurrence
- Extended-field radiation (para-aortic) - when para-aortic nodes involved
- Whole-abdomen radiation - occasionally for peritoneal spread (largely replaced by chemotherapy)
- Radiotherapy as primary treatment is reserved for medically unfit patients who cannot undergo surgery
Chemotherapy
- Indicated for high-risk disease (serous, clear cell, Grade 3, advanced stage)
- Standard regimen: Carboplatin + Paclitaxel (preferred over older cisplatin-doxorubicin-paclitaxel due to similar efficacy with less toxicity)
- For Stage III/IV: combined modality approach (chemotherapy + radiation)
- "Sandwich" chemotherapy-radiation-chemotherapy protocol shows improved survival in some studies
Hormonal Therapy
- Progestins (medroxyprogesterone acetate, megestrol acetate) - for recurrent/metastatic disease with ER/PR-positive tumours
- Response rates ~15-25% in recurrent disease
- Also used for fertility preservation
Treatment by Stage:
| Stage | Primary Treatment | Adjuvant |
|---|---|---|
| IA, Grade 1-2 | TAH+BSO | Observation ± vaginal brachytherapy |
| IA, Grade 3 / IB | TAH+BSO + lymph nodes | Vaginal brachytherapy ± EBRT |
| Stage II | TAH+BSO + lymph nodes | EBRT + vaginal brachytherapy |
| Stage III | TAH+BSO + debulking | Chemotherapy + radiation |
| Stage IV | Debulking surgery | Chemotherapy; palliative care |
Pattern of Spread
- Direct extension - myometrium → cervix → vagina → parametria → bladder, rectum
- Lymphatic - to pelvic (obturator, external iliac) and para-aortic lymph nodes
- Transtubal / Peritoneal - through fallopian tubes to peritoneal cavity (especially serous type)
- Haematogenous - lungs, liver, bone (late stage)
Recurrent Disease
- Vaginal recurrence most common (vault)
- Managed by: radiotherapy (if not previously irradiated), surgery, chemotherapy, hormonal therapy
- Isolated vaginal recurrences: salvage in up to 80% of patients with radiotherapy
- Berek & Novak's Gynecology, p. 2142
Uterine Sarcomas (Brief Mention)
Uterine sarcomas are a distinct group, different from endometrial carcinomas in risk factors, diagnosis, behavior, and management:
| Type | Origin | Notes |
|---|---|---|
| Leiomyosarcoma | Smooth muscle | Most common uterine sarcoma; arises de novo, not from fibroids |
| Endometrial Stromal Sarcoma | Endometrial stroma | Low-grade; ER/PR positive; responds to hormonal therapy |
| Adenosarcoma | Mixed Mullerian | Low-grade malignant stroma + benign glands |
| Carcinosarcoma (MMMT) | Mixed | Highly aggressive; now classified as metaplastic carcinoma |
- Berek & Novak's Gynecology, p. 2142
Summary of Key Points
| Point | Detail |
|---|---|
| Most common | Malignancy of female genital tract |
| Cardinal symptom | Postmenopausal bleeding |
| Main risk factor | Unopposed estrogen stimulation |
| Commonest type | Endometrioid adenocarcinoma (80-85%) |
| Deadliest type | Serous carcinoma (<10% of cases, >50% of deaths) |
| Precursor | Atypical endometrial hyperplasia |
| Hereditary risk | Lynch syndrome (HNPCC) |
| Diagnosis | Endometrial biopsy (Pipelle) |
| Imaging | TVS (screen), MRI pelvis (staging) |
| Staging | Surgical (FIGO 2009) |
| Treatment | TAH+BSO ± lymph node dissection |
| Adjuvant | Radiotherapy ± chemotherapy |
| Overall 5-yr survival | ~75% |
Sources:
- Berek & Novak's Gynecology, pp. 2141-2165
- Robbins, Cotran & Kumar: Pathologic Basis of Disease, pp. 932-934
- Goldman-Cecil Medicine (International Edition)
This is a shared conversation. Sign in to Orris to start your own chat.