
1000036227.jpg
Interpretation
analyse_media
Reading File
AP Pelvis X-ray Interpretation
Patient: Radya Shyam Kawan | PID: 394743 | Facility: Khwopa Hospital | Date: 2026-07-14
Technique
Anteroposterior (AP) view of the pelvis, 0.79x magnification. Adequate exposure and positioning.
Findings
LEFT HIP - Major Pathology
- Fracture-dislocation of the left hip: The left femoral head is severely deformed, fragmented, and displaced superiorly and laterally out of the acetabular cup - consistent with posterior/superior dislocation
- Comminuted fracture through the left femoral neck/intertrochanteric region with complete displacement
- Associated left acetabular disruption - the acetabular roof and posterior wall appear involved, suggesting a complex fracture-dislocation pattern
- Marked osteopenia of the left proximal femur and hemipelvis (likely disuse atrophy or chronic pathology)
RIGHT HIP
- Femoral head spherical and well-seated in the acetabulum
- Mild superior joint space narrowing
- Mild subchondral sclerosis of the acetabular roof - consistent with early osteoarthritis
- No acute fracture or dislocation
Pelvis / Pubic Symphysis / SI Joints
- Pubic symphysis is aligned; no diastasis
- Bilateral SI joint sclerosis and mild narrowing, more pronounced on the left - likely reactive
- No clear isolated pubic rami fractures identified, though pelvic tilt from left hip displacement alters geometry
Lumbar Spine
- L4-L5 visible with mild marginal osteophytes and disc space narrowing - degenerative changes
Soft Tissue
- Large oval radiolucency overlying the lower sacrum/coccyx - rectal gas shadow, not a bony lytic lesion
Summary of Key Findings
| Finding | Side | Severity |
|---|---|---|
| Fracture-dislocation (femoral neck/intertrochanteric + acetabulum) | Left | Severe |
| Osteopenia | Left hemipelvis | Marked |
| Osteoarthritis | Right hip, bilateral SI joints | Mild-moderate |
| Degenerative disc disease | L4-L5 | Mild |
Clinical Impression
Severe left hip fracture-dislocation - this is an orthopedic emergency. The combination of femoral neck/intertrochanteric comminuted fracture with acetabular involvement and superior-lateral femoral head displacement requires urgent management.
Recommendations
- Urgent orthopedic surgery consultation
- CT pelvis with 3D reconstruction - to fully characterize acetabular fracture pattern, assess pelvic ring stability, and plan surgical approach
- Assess neurovascular status of left lower limb (sciatic nerve injury risk with posterior hip dislocation)
- Surgical options to discuss: open reduction and internal fixation (ORIF) vs. total hip arthroplasty, depending on patient age, bone quality, and chronicity
⚠️ This interpretation is provided for educational/clinical support purposes. Final radiological diagnosis should be confirmed by a qualified radiologist and treating orthopedic surgeon.
HAV hepatitis
Finding Sources
Searching the Web
hepatitis A virus HAV clinical features diagnosis management 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Hepatitis A (HAV)
1. Virology
HAV belongs to the Picornaviridae family, genus Hepatovirus. Key features:
- 27 nm, non-enveloped, icosahedral nucleocapsid
- Positive-sense, single-stranded RNA genome (~7.4-7.5 kb)
- Capsid made of 4 proteins: VP1, VP2, VP3, VP4 - VP1 is the spike that binds host cell receptor (α2-macroglobulin)
- Only one serotype (multiple genotypes: I, II, III; genotype I predominates worldwide)
- Replicates in the cytoplasm via RNA-dependent RNA polymerase
- Resists inactivation; stable at -20°C and low pH
- Formerly called "infectious hepatitis" or "short-incubation hepatitis"
(Goldman-Cecil Medicine; Sherris & Ryan Medical Microbiology)
2. Epidemiology & Transmission
-
Worldwide distribution - endemic in Asia, Africa, Middle East, Central/South America
-
Seroprevalence ranges from ~13% (Sweden) to ~100% (poor sanitary conditions)
-
Primary route: Fecal-oral - contaminated food/water, person-to-person contact
-
High-risk groups:
- Travelers to endemic countries
- Children in day care centers (and their parents)
- Men who have sex with men
- Injection drug users / homeless persons
- Hemophilia patients receiving plasma products
- Health care workers
-
Blood transfusion transmission is possible but uncommon
-
No chronic carriage - does not cause chronic infection
(Goldman-Cecil Medicine, p. 1567)
3. Pathogenesis
After ingestion, HAV:
- Replicates in intestinal mucosa (incubation 15-45 days)
- Enters viremia → spreads to liver
- In the liver: causes lymphoid cell infiltration, hepatocyte necrosis, and Kupffer cell proliferation
- Virus is secreted into bile → shed in stool (major infectious route)
- Cell lysis releases virions
4. Clinical Features
- Incubation period: 15-45 days (mean ~1 month)
- Up to 50% of infections are subclinical in children; symptomatic cases increase with age
Prodromal (pre-icteric) phase:
- Fever, anorexia, nausea, vomiting
- Right upper quadrant pain
- Fatigue, malaise
Icteric phase:
- Jaundice
- Dark urine (bilirubinuria) - appears before jaundice
- Clay/pale-colored stools
- Pruritus (if cholestatic)
Special forms:
- Relapsing hepatitis A - most common cause of relapsing cholestatic hepatitis
- Prolonged course (6-9 months) in ~10% of adults
- Hospitalization required in up to 13% of adult cases
5. Serological Markers & Timeline
The serological course is the most important concept for diagnosis:
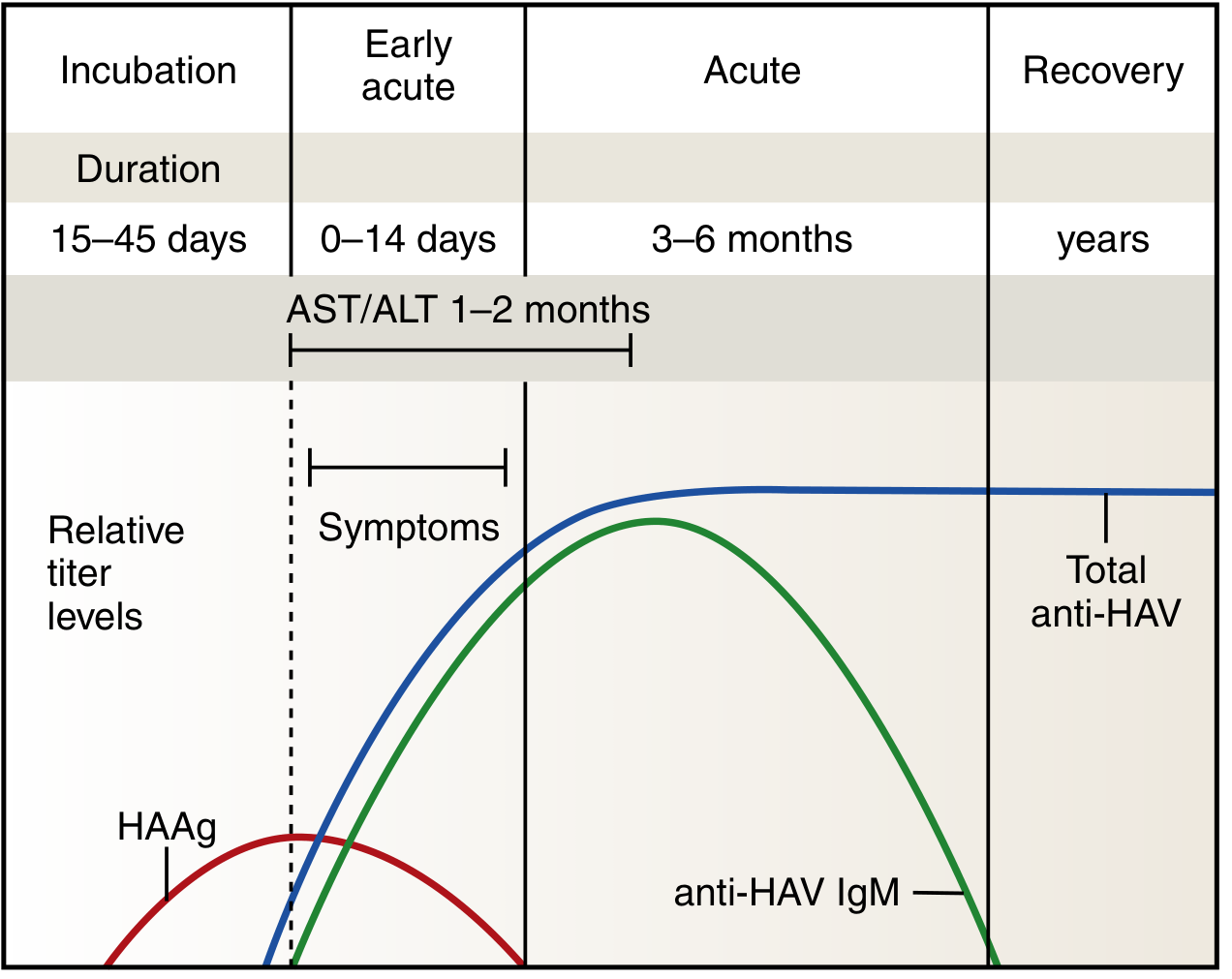
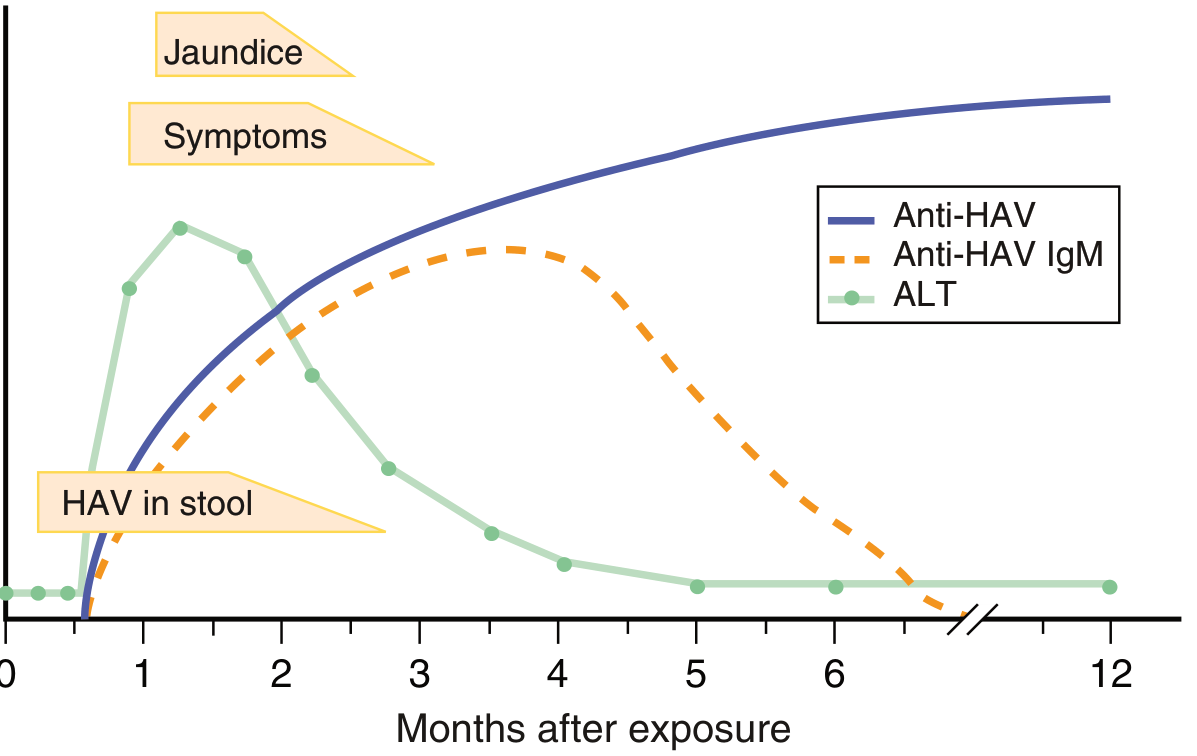
| Marker | Appearance | Significance |
|---|---|---|
| HAV RNA in stool | 3-10 days before symptom onset; 1-2 weeks after | Peak infectivity period |
| HAAg (HAV antigen) | Incubation period | Disappears before acute illness |
| IgM anti-HAV | ~2-3 weeks post-infection; peaks at 2nd month | Gold standard for acute HAV diagnosis |
| IgG anti-HAV | 1-2 weeks after IgM | Persists for life; confers immunity |
| AST/ALT | Rise at early acute phase; last 1-2 months | Non-specific liver injury marker |
- IgM anti-HAV disappears in 4-12 months
- IgG anti-HAV persists lifelong - protective immunity
(Henry's Clinical Diagnosis; Goldman-Cecil Medicine, p. 1567)
6. Diagnosis
- Definitive: IgM anti-HAV by enzyme immunoassay (EIA) - the diagnostic standard for acute infection
- HAV RNA by PCR (stool/serum) - not routinely needed
- LFTs: elevated ALT, AST, bilirubin
- "Total anti-HAV" (detects both IgM + IgG) - used to assess immunity/vaccination status, not acute diagnosis
- Only test symptomatic individuals with IgM (false positives occur in asymptomatic)
7. Treatment
- No specific antiviral treatment - infection is self-limited
- Supportive care: rest, hydration, nutrition
- Hospitalization for severe cases
- Liver transplantation is the only option for fulminant acute liver failure (rare)
- Avoid hepatotoxic drugs and alcohol
8. Prognosis
- Typically resolves in 3-4 weeks without complications
- Never progresses to chronic infection (key differentiator from HBV/HCV)
- Fulminant hepatitis A: <0.1% of cases, but risk and mortality increase with age
- Mortality: 1.8% in patients >50 years
- 4% of all fulminant hepatitis cases in the US are HAV
- Superinfection with HAV in chronic HBV patients: 6-23x higher morbidity/mortality
- Poor prognosis indicators: Factor V <40%, signs of encephalopathy, worsening jaundice, ascites, acute liver shrinkage
(Goldman-Cecil Medicine, p. 1568)
9. Prevention & Vaccination
Vaccine (inactivated HAV antigen):
- Two-dose schedule: Day 0 and 6-18 months later
- Accelerated schedule (for travelers): Days 0, 7, 21
- Virtually 100% seroconversion in healthy individuals
- Combined HAV+HBV vaccine is available
- Protective titers persist: at least 27 years after vaccination
- Post-vaccination IgG titers remain detectable in ~99% at 5 years
Indications for vaccination:
- Travelers to endemic areas
- MSM (men who have sex with men)
- Injection drug users
- Healthcare professionals
- Patients with chronic liver disease
- Close contacts of HAV cases
- Children as part of childhood immunization programs
Post-exposure prophylaxis (PEP):
- Both HAV vaccine and immunoglobulin (IG) are ~98% effective for PEP
- Vaccination preferred (also prevents secondary cases)
- Often used together in PEP settings
(Goldman-Cecil Medicine, p. 1567-1568)
Summary Comparison with other Hepatitis Viruses
| Feature | HAV |
|---|---|
| Virus family | Picornaviridae |
| Genome | ssRNA (+sense) |
| Envelope | None (naked) |
| Transmission | Fecal-oral |
| Incubation | 15-45 days |
| Chronic infection | Never |
| Vaccine | Yes (inactivated) |
| Diagnosis | IgM anti-HAV |
| Treatment | Supportive |
This is a shared conversation. Sign in to Orris to start your own chat.