hernia. definition,risk factors,causes, symptoms,diagnosis, treatment,hernioplasty
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative surgical textbooks. Let me compile the complete answer.
Hernia: A Comprehensive Overview
1. Definition
A hernia is the protrusion of an organ or tissue through an abnormal opening or weakness in the wall of the cavity that normally contains it. Most commonly, this involves abdominal contents (bowel, omentum, fat) protruding through defects in the abdominal wall or related fascial structures.
Key terminology:
- Reducible hernia – contents can be returned to the original cavity spontaneously or with manual pressure
- Irreducible / Incarcerated hernia – contents are trapped and cannot be reduced; may cause obstruction
- Strangulated hernia – vascular supply to the herniated contents is compromised; a surgical emergency
Hernias of all types are second only to adhesions as the most frequent causes of intestinal obstruction in western countries. — Mulholland and Greenfield's Surgery, 7e
2. Classification / Types
By Location
| Type | Description |
|---|---|
| Indirect inguinal | Protrudes through the deep inguinal ring alongside the spermatic cord; congenital (patent processus vaginalis); most common (2/3 of inguinal hernias) |
| Direct inguinal | Protrudes through the posterior wall of the inguinal canal (Hesselbach's triangle) medial to the inferior epigastric vessels; acquired weakness |
| Femoral | Protrudes through the femoral canal, inferior to the inguinal ligament; higher incarceration rate (~45%); more common in women |
| Umbilical | Through a defect at the umbilicus; common in infants and obese/multiparous women |
| Incisional / Ventral | At sites of prior surgical incisions; occurs in ~20% of laparotomy patients |
| Epigastric | Through linea alba above the umbilicus |
| Spigelian | Through the spigelian fascia at the lateral edge of the rectus muscle; high incarceration risk |
| Obturator | Through the obturator canal; classic in frail elderly women; high perforation rate >50%, mortality ~20% |
| Hiatal / Diaphragmatic | Stomach or abdominal organs herniate through the diaphragm into the thorax |
| Pantaloon | Combined direct + indirect inguinal hernia |
| Richter hernia | Only the antimesenteric border of the bowel wall is trapped; can strangulate without complete obstruction |
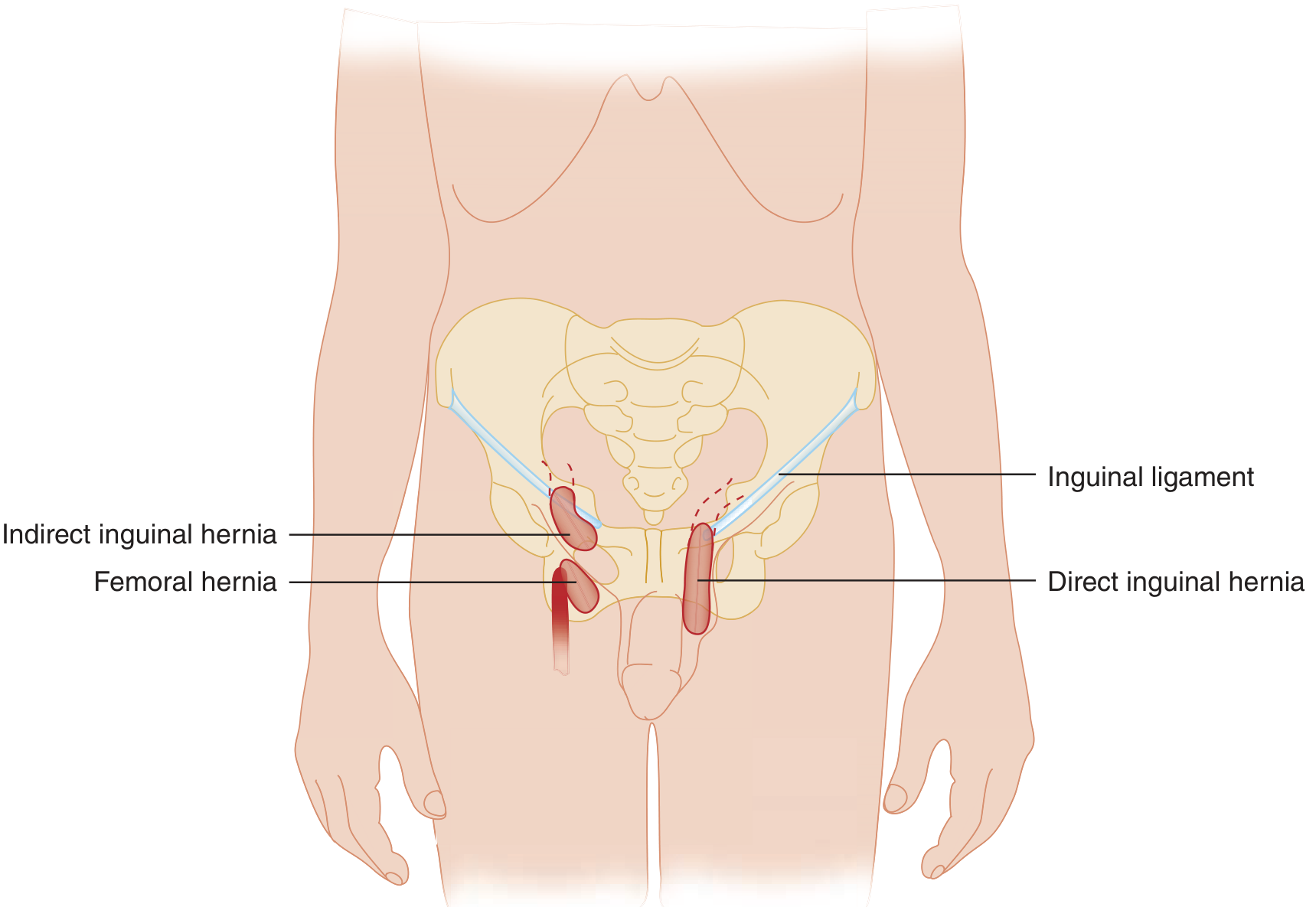
Groin hernia anatomy — Tintinalli's Emergency Medicine
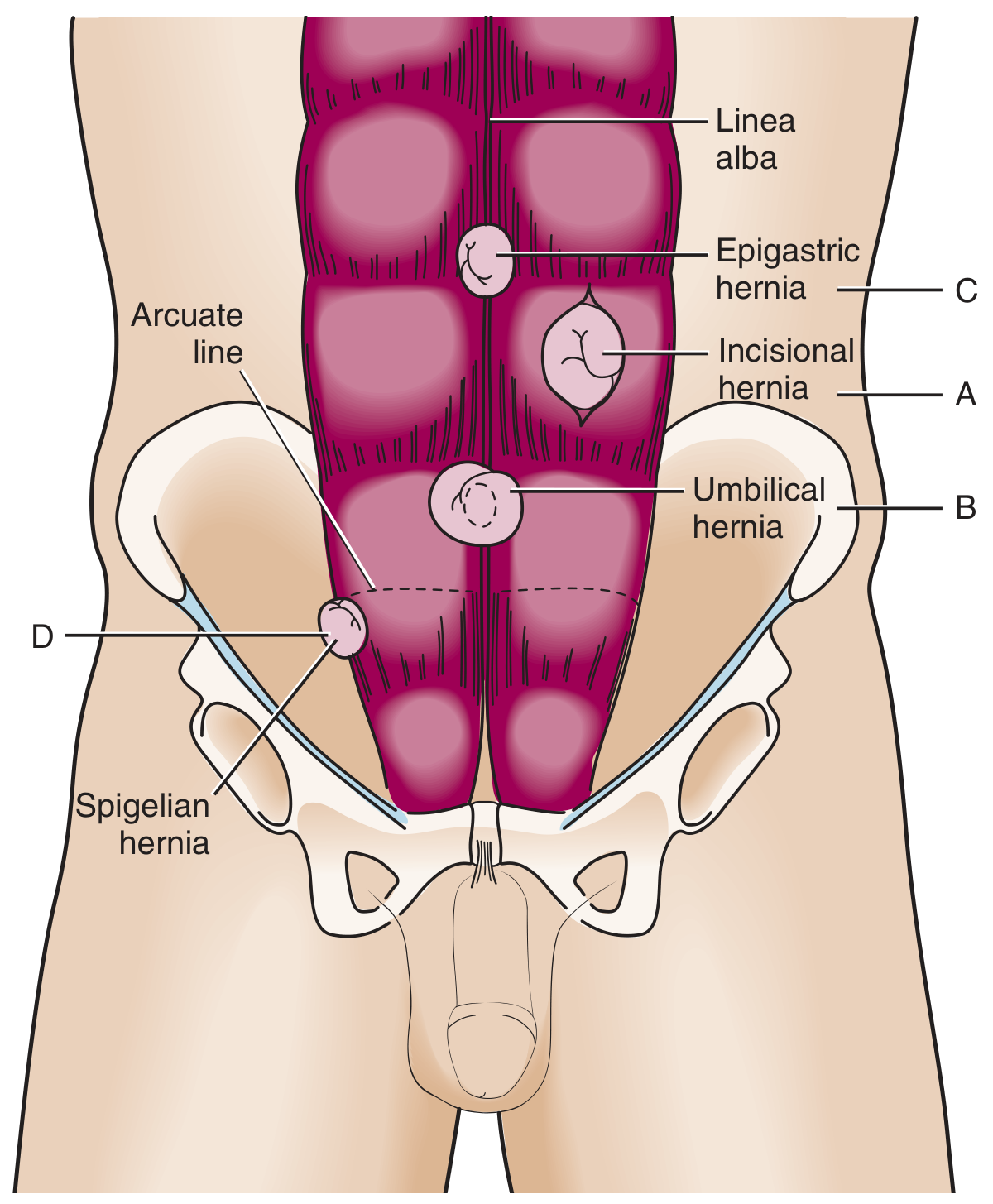
Ventral hernia types — Roberts and Hedges' Clinical Procedures in Emergency Medicine
3. Causes & Pathophysiology
Indirect Inguinal Hernia
- Failure of closure of the processus vaginalis (a peritoneal diverticulum that accompanies the testis into the scrotum during fetal development)
- Explains the high incidence in premature infants (closure normally occurs before birth)
- By definition, all congenital hernias in children are indirect
Acquired Hernias (Direct, Femoral, Ventral)
- Weakness or defects in the abdominal wall fascia/musculature due to:
- Degenerative changes in connective tissue (collagen metabolism defects)
- Prior surgery → incisional hernias
- Infection → poor wound healing
- Increased intra-abdominal pressure (chronic straining, obesity, pregnancy)
4. Risk Factors
| Category | Risk Factors |
|---|---|
| Demographics | Male sex (inguinal hernia 10:1 male:female), advanced age, prematurity |
| Congenital | Patent processus vaginalis, connective tissue disorders |
| Increased IAP | Chronic cough (COPD), constipation/straining, heavy lifting, ascites, pregnancy, obesity |
| Prior surgery | Abdominal operations → incisional hernia (up to 20% incidence); poor wound healing |
| Infection | Wound infection increases risk of incisional hernia significantly |
| Systemic | Immunosuppression, corticosteroid use, collagen vascular disease, smoking |
| Family history | First-degree relatives with hernia |
5. Symptoms & Clinical Presentation
Reducible Hernia
- Groin or abdominal bulge that appears with standing, coughing, straining (Valsalva)
- Disappears on lying down or with manual pressure
- Dull ache or pressure sensation at the site
- May be asymptomatic and noticed incidentally
Incarcerated Hernia
- Firm, tender, non-reducible bulge
- Pain at the hernia site
- Signs of intestinal obstruction: nausea, vomiting, abdominal distension, cessation of flatus/stool
- In infants: fussiness, irritability, firm groin mass
Strangulated Hernia
- Severe, constant pain at the hernia site
- Overlying skin changes: erythema, edema
- Systemic signs: fever, tachycardia, toxic appearance, peritonitis, sepsis
- Vomiting and complete obstruction
- Surgical emergency — bowel necrosis may follow rapidly
"Is the hernia easily reducible or incarcerated? Is the vascular supply to the bowel strangulated? A patient with an easily reducible hernia can be discharged safely for outpatient follow-up and elective repair, whereas an acutely incarcerated and strangulated hernia is [a surgical emergency]." — Roberts and Hedges' Clinical Procedures in Emergency Medicine
6. Diagnosis
Clinical Assessment (Primary)
- History: location, onset, aggravating factors, obstructive symptoms
- Physical examination: Standing and supine; Valsalva maneuver to bring out the bulge
- Palpate the inguinal canal by invaginating scrotal skin
- Impulse felt at fingertip = indirect hernia; at pulp of finger = direct hernia
- Assess reducibility and tenderness
Laboratory Studies
- Routine CBC, electrolytes, urinalysis — minimal diagnostic value for uncomplicated hernia; useful for pre-operative clearance or ruling out alternative diagnoses
Imaging
| Modality | Role |
|---|---|
| Plain X-ray | Not required unless bowel obstruction suspected; may show dilated loops or free air |
| Ultrasound (US) | First-line for confirmation, especially in children and pregnant women; dynamic assessment with Valsalva; identifies free fluid (incarceration), absent peristalsis, Doppler vascular flow. Operator-dependent; limited by body habitus |
| CT scan | Gold standard imaging; best for identifying occult hernias (Spigelian, obturator), contents, complications (incarceration/strangulation); essential for obturator hernia diagnosis |
| MRI | Used in athletic pubalgia/sports hernia workup; MRI with Valsalva in prone position |
CT is the best-performing radiographic test for hernia diagnosis and can identify uncommon hernia types as well as demonstrate incarceration and strangulation. — Tintinalli's Emergency Medicine
Ultrasound Signs of Strangulation:
- Free fluid in the hernia sac
- Hyperechoic fat
- Wall thickening of herniated bowel
- Absence of peristalsis
- Loss of venous/lymphatic Doppler signal
7. Treatment
Conservative (Non-Surgical)
- Watchful waiting is acceptable for asymptomatic or minimally symptomatic reducible inguinal hernias in men — risk of incarceration is low (~0.2%/year)
- Truss (mechanical support) — not recommended as definitive treatment; does not prevent progression
- Weight loss, cough treatment to reduce intra-abdominal pressure
- Note: Spontaneous resolution does NOT occur in children after infancy; children with inguinal hernia should undergo elective repair
Emergency Treatment (Incarcerated/Strangulated)
- Attempted manual reduction (taxis) — for incarcerated hernias WITHOUT signs of strangulation:
- NPO status
- Adequate IV narcotic analgesia
- Cold packs to reduce swelling
- Grasp and elongate hernia neck with one hand; apply steady pressure proximally at the fascial defect
- One or two attempts; consult surgery if unsuccessful
- If strangulated: No reduction attempts; immediate surgical consultation; IV antibiotics; fluid resuscitation; urgent OR
- Beware "reduction en masse" — apparent reduction but bowel remains incarcerated within the sac inside the peritoneal cavity; persistent pain despite apparent reduction requires imaging
Surgical Treatment
Surgery is the definitive treatment. The primary decision is tissue repair (herniorrhaphy) vs. mesh repair (hernioplasty).
8. Hernioplasty
Definition
Hernioplasty refers to the reconstruction of the inguinal floor (or other fascial defect) using prosthetic mesh to reinforce or bridge the defect — contrasted with herniorrhaphy, which closes the defect using native tissue sutures alone.
"The herniorrhaphy performed in children involves closing off the patent processus vaginalis. This is to be contrasted with the hernioplasty performed in adults, which requires reconstruction of the inguinal floor." — Schwartz's Principles of Surgery, 11e
Open (Anterior) Approaches
A. Lichtenstein Tension-Free Repair (Gold Standard for Adults)
- A flat polypropylene mesh is placed over the inguinal floor and sutured into position, creating a tension-free repair
- Mesh covers Hesselbach's triangle and extends to the internal ring
- A slit in the mesh allows passage of the spermatic cord and creates a new internal ring
- Advantages: low recurrence (<1%), low tension, can be done under local anesthesia
- Current recommendation: open tissue repair preferred in contaminated/emergency cases; mesh reserved for elective/recurrent repairs
B. Plug and Patch (Rutkow-Robbins / Gilbert)
- A modification of Lichtenstein; a 3D polypropylene plug is placed into the internal inguinal ring (for indirect hernia) or the direct defect, followed by a flat mesh patch over the inguinal floor
C. Bassini Repair (Tissue — Historical)
- Classic tissue repair: transversalis fascia, transversus abdominis, and internal oblique muscles are sutured to the inguinal ligament
- Higher tension and recurrence compared to mesh repairs
D. Shouldice Repair (Best Tissue Repair)
- Four-layer running suture repair of the posterior wall (transversalis fascia)
- Best tissue repair technique; low recurrence in specialized centers
- Uses no mesh; preferred when mesh is contraindicated
E. McVay (Cooper's Ligament) Repair
- Transversalis fascia sutured to Cooper's ligament; also repairs femoral hernia
- Requires a relaxing incision to reduce tension
F. Desarda Repair (Mesh-Free)
- Strip of external oblique aponeurosis sutured to the inguinal ligament as a mesh substitute
- Introduced 2001; mesh-free option
Laparoscopic (Posterior) Approaches
| Technique | Description |
|---|---|
| TAPP (Trans-Abdominal Pre-Peritoneal) | Laparoscopic; peritoneum opened; mesh placed in preperitoneal space; peritoneum re-closed over mesh |
| TEP (Totally Extraperitoneal) | Laparoscopic; entirely in the preperitoneal space without entering peritoneal cavity; mesh placed; steep learning curve |
Advantages of laparoscopic repair: Less postoperative pain, faster return to activity, better for bilateral and recurrent hernias, excellent visualization of anatomy
Disadvantages: Higher technical difficulty, risk of bowel/vascular injury, cannot be done under local anesthesia
Mesh Considerations
- Synthetic permanent mesh (polypropylene): most common; excellent long-term results
- Biologic mesh: for contaminated fields (bowel resection, infection)
- In contaminated/emergency cases: mesh use is controversial; tissue repair preferred to avoid mesh infection
- Risk with mesh: infection, chronic groin pain, mesh migration, ischemic orchitis (0.2–1%), seroma
Key Complications of Hernia Repair
| Complication | Notes |
|---|---|
| Recurrence | 0.5–2% with mesh; 10–15% with tissue repair |
| Chronic groin pain | Most common long-term complaint |
| Urinary retention | More common with general/spinal anesthesia (13%) vs. local (0.2%) |
| Ischemic orchitis / testicular atrophy | ~1% |
| Wound infection / seroma | More common with mesh in contaminated field |
| Nerve injury | Ilioinguinal, iliohypogastric, genitofemoral nerves |
Summary Table
| Feature | Detail |
|---|---|
| Most common hernia | Indirect inguinal (75% of all hernias) |
| Most common in women | Femoral hernia |
| Highest incarceration risk | Femoral (45%), obturator (>50%) |
| Gold standard imaging | CT scan |
| Gold standard repair in adults | Lichtenstein tension-free hernioplasty |
| Best tissue repair | Shouldice repair |
| Herniorrhaphy (children) | High ligation of sac; no floor reconstruction |
| Hernioplasty (adults) | Mesh reinforcement of inguinal floor |
| Emergency hernia treatment | IV antibiotics, fluid resus, urgent surgery |
Sources: Schwartz's Principles of Surgery 11e · Mulholland and Greenfield's Surgery 7e · Tintinalli's Emergency Medicine · Roberts and Hedges' Clinical Procedures in Emergency Medicine · Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.