Cataract differential diagnosis, investigation, management
Reading File
Finding Sources
Searching PubMed
cataract diagnosis management surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from Kanski's Clinical Ophthalmology. Let me compile the full answer.
Cataract: Differential Diagnosis, Investigation, and Management
Primary source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Goldman-Cecil Medicine
Definition & Overview
A cataract is any opacification of the crystalline lens. It is the commonest cause of reversible visual disability in the world. There is no medical treatment to prevent its development or progression - phacoemulsification with intraocular lens (IOL) implantation is the only effective treatment and is the most commonly performed surgical procedure worldwide.
Symptoms
The effect on vision depends on the type, extent, and position of the opacity. Key symptoms include:
- Reduced visual acuity - initially correctable with spectacles
- Loss of contrast sensitivity
- Change in colour perception - particularly impaired perception of blue colours
- Glare - from light scattering; worse with posterior subcapsular types; difficulty with night driving
- Monocular diplopia - especially with point sources of light
- "Second sight" - paradoxical improvement in near vision in nuclear sclerotic cataract due to increased refractive index causing acquired myopia
Classification & Differential Diagnosis
A. Age-Related (Acquired) Cataract
The most common form. Three main morphological subtypes:
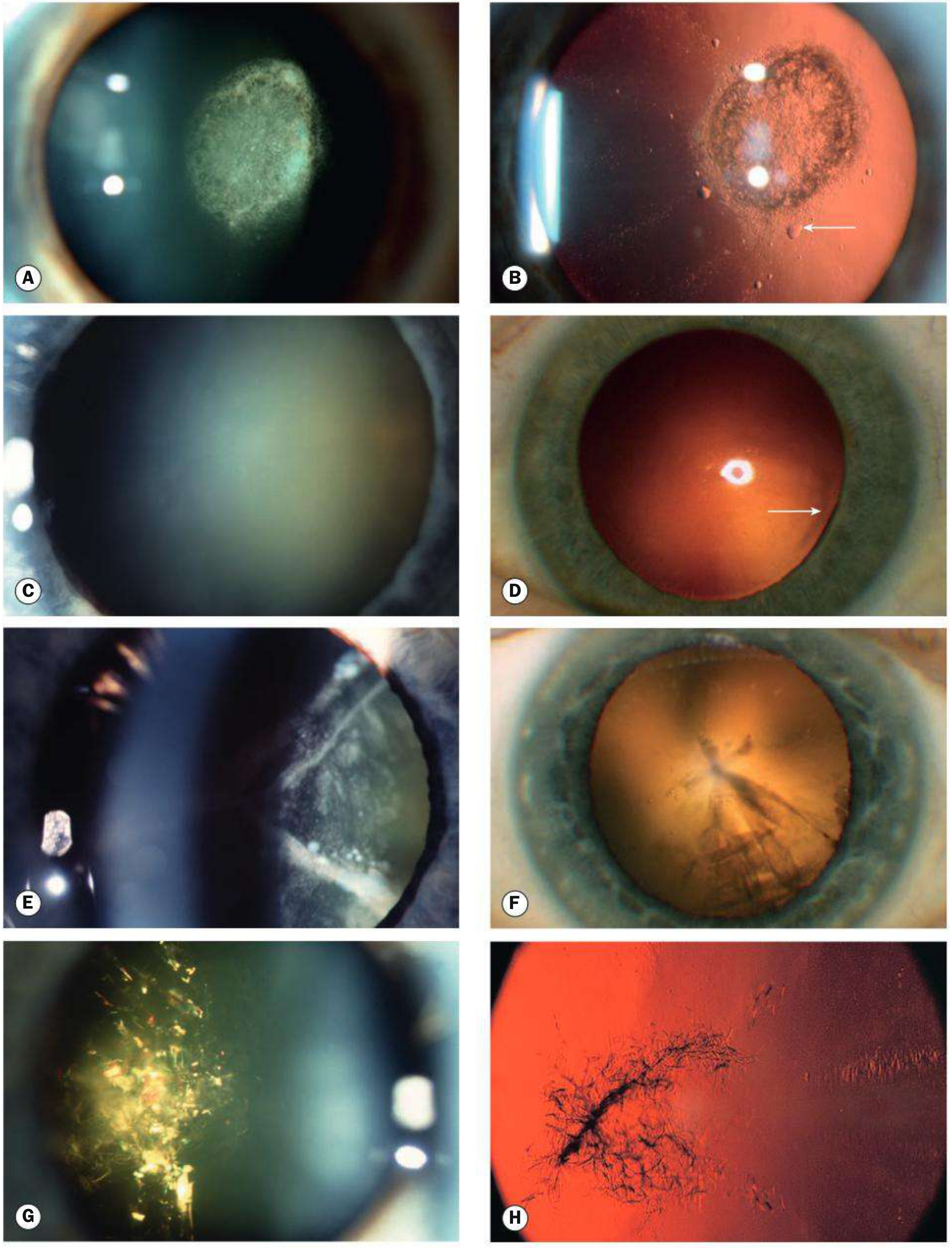
1. Posterior Subcapsular (PSC) Cataract
- Granular or plaque-like opacity just in front of the posterior capsule
- On retroillumination: appears black and vacuolated (Wedl/bladder cells)
- Located at the nodal point - disproportionately profound effect on vision
- Worse symptoms: glare, near vision difficulty (miosis makes it worse in bright light and near tasks)
- Strong association with: corticosteroids, diabetes, radiation, uveitis, retinitis pigmentosa
2. Nuclear Sclerotic Cataract
- Exaggeration of normal ageing
- Yellowish-brown hue from urochrome pigment deposition
- Best assessed with oblique slit-lamp beam
- Retroillumination: good red reflex but subtle nucleus-cortex distinction
- When advanced: brunescent (brown) or rarely black (nigra) cataract
- Associated with acquired myopia ("second sight of the aged")
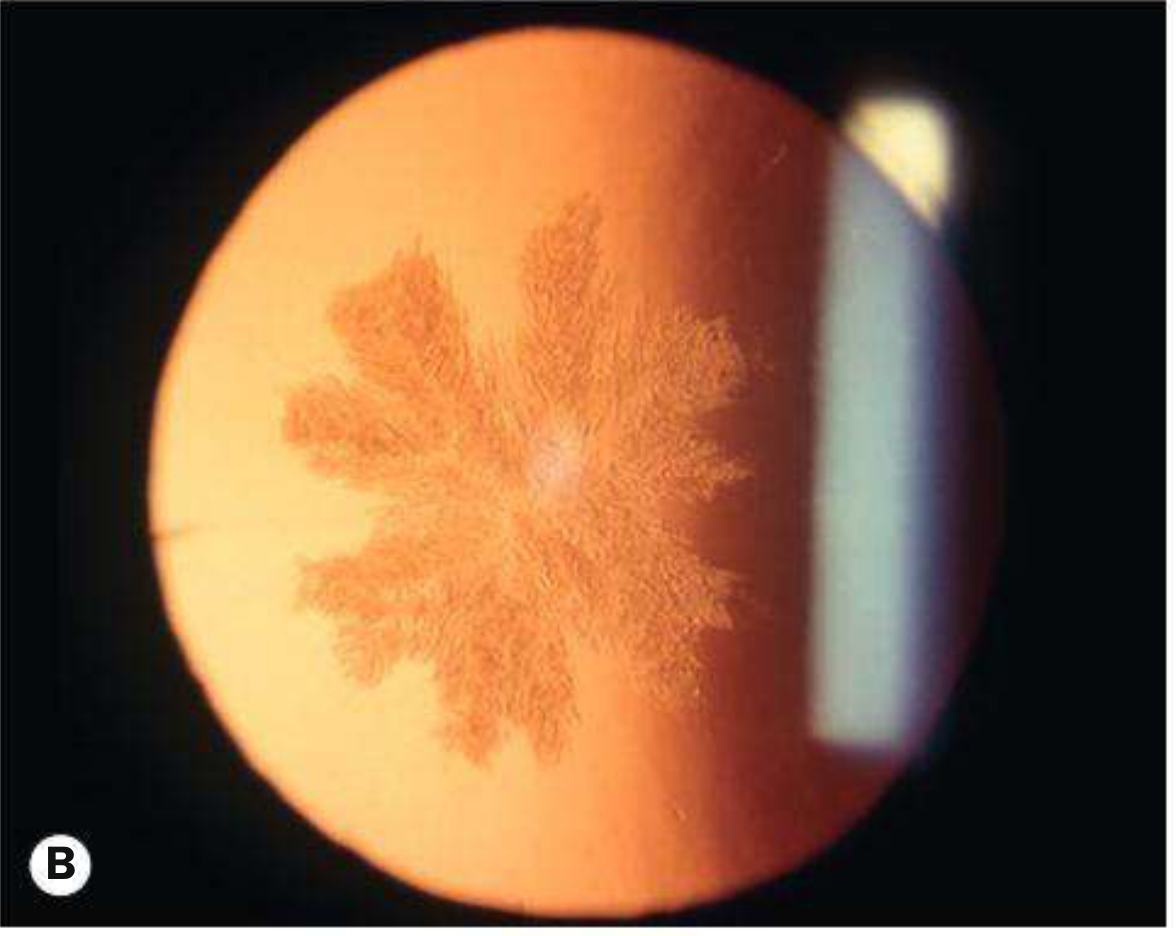
3. Cortical Cataract
- Involves anterior, posterior, or equatorial cortex
- Begins as clefts and vacuoles due to cortical hydration
- Classic cuneiform (wedge-shaped) or radial spoke-like opacities
- Often starts in the inferonasal quadrant
- Glare is a prominent symptom
4. Christmas Tree Cataract (Uncommon)
- Polychromatic needle-like formations in deep cortex and nucleus
- Often associated with myotonic dystrophy
Advanced States of Maturity
| Stage | Features |
|---|---|
| Immature | Partial opacification; iris shadow seen |
| Mature | Complete opacification; no iris shadow; white/grey appearance |
| Hypermature | Wrinkling of anterior capsule as lens shrinks |
| Morgagnian | Liquefaction of cortex; nucleus sinks inferiorly |
B. Cataract in Systemic Disease
| Disease | Cataract Type |
|---|---|
| Diabetes mellitus | "Snowflake" (bilateral, rapid-onset cortical opacities in young T1DM); also early nuclear sclerosis |
| Myotonic dystrophy | PSC spokes assuming a stellate morphology; Christmas tree; often bilateral |
| Atopic dermatitis | Shield-like anterior subcapsular opacity; 10% of severe cases; 2nd-4th decades |
| Neurofibromatosis type 2 | PSC opacity |
| Wilson's disease | Sunflower cataract (anterior subcapsular deposits from copper) |
| High myopia | PSC and early nuclear sclerosis |
| Galactosaemia | "Oil droplet" opacity (AR, GALT enzyme deficiency) |
| Lowe syndrome | Congenital cataract (universal); X-linked recessive |
| Mannosidosis | Spoke-like posterior cortical punctate opacities (AR) |
| Hypo/pseudohypoparathyroidism | Bilateral subcapsular opacities |
C. Secondary (Complicated) Cataract
Caused by other ocular disease:
- Uveitis - anterior plaque opacities; extensive posterior synechiae
- Glaucoma - Glaukomflecken: anterior subcapsular grey-white opacities after acute angle-closure attack
- Retinitis pigmentosa / Leber congenital amaurosis / Gyrate atrophy / Stickler syndrome - PSC opacity
- Medications: systemic and topical corticosteroids (PSC); chlorpromazine (anterior star-shaped opacity)
D. Traumatic Cataract
- Most common cause of unilateral cataract in young people
- Penetrating trauma: direct lens capsule breach
- Blunt trauma: classic flower-shaped opacity (Vossius ring imprint)
- Electric shock/lightning: diffuse milky-white or multiple snowflake stellate subcapsular opacities
- Infrared radiation ("glassblower's cataract"): true exfoliation of anterior lens capsule
- Ionizing radiation: PSC opacity (delayed, months-years post-exposure)
E. Congenital Cataract
- Incidence: ~3 in 10,000 live births
- Aetiology: 1/3 systemic disease; 1/3 inherited (most commonly autosomal dominant); 1/3 unknown
- 2/3 bilateral (cause found in ~50%); unilateral cases usually sporadic
Intrauterine infections (TORCH):
- Rubella: pearly nuclear or diffuse bilateral opacity (~15%)
- Toxoplasmosis: cataract + chorioretinitis
- CMV: cataract + chorioretinitis + microcephaly
- Varicella: cataract + microphthalmos
Metabolic causes:
- Galactosaemia: oil-droplet opacity (reversible with dietary exclusion of galactose)
- Lowe syndrome: universal cataract + microphakia + congenital glaucoma in 50%
- Mannosidosis: posterior cortical spoke-like opacities
Differential Diagnosis of Leukocoria (White Pupil)
When a cataract causes leukocoria, particularly in children, always exclude:
| Condition | Key differentiating features |
|---|---|
| Retinoblastoma | Most urgent to exclude; irregular white pupil reflex; intraocular mass on USS/MRI |
| Persistent Foetal Vasculature (PFV) | Unilateral; fibrovascular stalk from disc; microphthalmos |
| Retinopathy of prematurity | History of prematurity; temporal retinal traction |
| Coats disease | Unilateral; subretinal exudates; telangiectatic vessels |
| Toxocara chorioretinitis | Peripheral granuloma; serology |
| Corneal opacity/leucoma | Superficial - on slit-lamp vs intra-lenticular |
| Vitreous haemorrhage | Absent red reflex; B-scan ultrasound |
| Endophthalmitis | Acute inflammatory; painful; hypopyon |
Investigation
Ophthalmic Assessment (Pre-operative)
| Investigation | Purpose |
|---|---|
| Visual acuity (Snellen/LogMAR) | Baseline and indication for surgery |
| Glare testing | Functional impact assessment |
| Slit-lamp biomicroscopy | Type, morphology, maturity of cataract |
| Retroillumination | Better delineation of PSC and cortical cataracts |
| Dilated fundus examination | Exclude posterior pole pathology (AMD, diabetic retinopathy, macular disease) that would limit visual gain |
| Biometry (optical/IOL Master) | Axial length + keratometry for IOL power calculation |
| Keratometry/corneal topography | Planning toric IOL or astigmatism correction |
| Specular microscopy | Corneal endothelial cell count - important if Fuchs' dystrophy or prior corneal surgery |
| Optical coherence tomography (OCT) | Macular assessment prior to surgery |
| B-scan ultrasound | When fundus view is obscured by dense cataract |
| Electrophysiology (ERG/VEP) | Retinal function assessment in dense cataracts when no fundal view possible |
| Potential acuity meter / laser interferometry | Predict post-operative VA when retinal view is obscured |
Systemic Workup (Pre-operative)
- Routine tests (bloods, ECG) are not required for local anaesthesia
- If general anaesthesia planned: U&E, random blood glucose, FBC, ECG
- Relevant medication review: alpha-blockers (intraoperative floppy iris syndrome - IFIS), anticoagulants (INR check within 72 hours), metformin (if contrast planned)
Investigation for Congenital Cataract
- TORCH serology (rubella IgM, CMV, toxoplasma)
- Urine for reducing substances (galactosaemia)
- Urine amino acids (Lowe syndrome)
- Serum galactose-1-phosphate uridyltransferase
- Chromosomal karyotype if dysmorphic features
- Paediatric/genetics referral
Management
Conservative (Non-Surgical) Measures
- Refractive correction: spectacles or contact lenses may help in early cataract
- Pupil dilation (mydriatic drops) can transiently improve vision in PSC cataracts by allowing light around the opacity
- Lifestyle advice: increase lighting, magnification aids
- No proven pharmacological therapy to prevent or reverse cataract
Surgical Indications
- Visual indications: opacity sufficient to interfere with daily activities (driving, reading, occupation)
- Medical indications:
- Phacolytic glaucoma (mature cataract leaking protein causing macrophage-mediated trabecular obstruction)
- Phacomorphic glaucoma (intumescent lens causing angle-closure)
- Improved fundus view for monitoring/treating posterior segment disease
Surgical Options
1. Phacoemulsification with IOL Implantation (Gold Standard)
The standard procedure worldwide. Steps:
- Preparation: topical antiseptic (povidone-iodine 5%), draping, speculum
- Incisions: corneal side port + main clear corneal incision (typically temporal)
- Viscoelastic injection into anterior chamber
- Continuous curvilinear capsulorhexis (CCC): circular opening in anterior capsule
- Hydrodissection: fluid injection under capsule to separate nucleus from cortex
- Nuclear division: "Divide and conquer" (two perpendicular grooves, cracking into quadrants) or "Phaco chop" (faster, lower energy)
- Emulsification and aspiration of nuclear quadrants
- Cortex aspiration: irrigation-aspiration (I/A) handpiece
- IOL implantation into capsular bag
- Wound closure: typically self-sealing
Anaesthesia options:
- Topical (drops/gel ± intracameral lidocaine) - most common; no akinesia
- Sub-Tenon block - good anaesthesia, variable akinesia
- Peribulbar block - effective anaesthesia and akinesia; avoid in long eyes (axial >25 mm)
- General anaesthesia - children, uncooperative patients, tremor, dementia
2. Femtosecond Laser-Assisted Cataract Surgery (FLACS)
- Laser performs incisions, CCC, and nuclear fragmentation
- Standard phacoemulsification provides equivalent results in most studies
3. Small Incision Cataract Surgery (SICS) / Manual ECCE
- Used in low-resource settings or very hard nuclei
Intraocular Lens (IOL) Types
| IOL Type | Feature |
|---|---|
| Monofocal | Standard; one focal point (usually distance); reading glasses needed |
| Toric | Corrects pre-existing corneal astigmatism |
| Multifocal/Extended depth-of-focus (EDOF) | Near + distance correction; may cause halos/glare |
| Accommodating | Attempts to restore accommodation |
| Light-adjustable IOL | UV irradiation post-implant fine-tunes refractive power |
Post-operative Care
- Topical antibiotic + steroid drops (e.g., 4-6 weeks)
- Review at Day 1, Week 1, 4-6 weeks
- Refraction at ~6 weeks for spectacle prescription
Complications of Cataract Surgery
Intraoperative
- Posterior capsular rupture with vitreous loss (<1% experienced surgeons)
- Zonular dehiscence
- Dropped nucleus (~0.2%)
- IFIS (with alpha-blockers)
Early Post-operative
- IOP spike
- Iridocyclitis
- Corneal oedema
- Wound leak
Late Post-operative
- Posterior capsular opacification (PCO): most common late complication; Elschnig pearl formation or fibrosis-type PCO; treated with Nd:YAG laser posterior capsulotomy
- Cystoid macular oedema (CMO)
- Retinal detachment (<1%)
- IOL dislocation/subluxation
- Endophthalmitis (0.1%) - most serious infectious complication
PCO Treatment (Nd:YAG Capsulotomy)
- Indication: reduced VA or glare from PCO
- Power: start at 1 mJ/pulse; cruciate or circumferential pattern; opening ~4-5 mm
- Complications: IOL pitting, IOP spike, retinal detachment risk (warn myopes), CMO
Congenital Cataract Management
- Timing is critical - amblyopia risk means surgery should not be delayed
- Bilateral visually-significant cataracts: surgery within first weeks of life
- Unilateral: surgery within 6-10 weeks, followed by aggressive patching of the fellow eye
- Optical correction post-surgery (contact lenses in infants, glasses when older)
- Amblyopia treatment (occlusion/patching) is essential
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 308-344; Goldman-Cecil Medicine, International Edition, p. 4131
This is a shared conversation. Sign in to Orris to start your own chat.