Carcinogen in tobacco and its action involved in carcinoma of oral cavity
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tobacco" AND "oral cavity carcinoma" AND "carcinogen"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the data needed for a comprehensive answer. Here it is:
Carcinogens in Tobacco and Their Role in Oral Cavity Carcinoma
Overview
Approximately 95% of cancers of the oral cavity are squamous cell carcinomas (oral SCC). Tobacco - both smoked and smokeless - is the single most important risk factor. The carcinogens differ slightly depending on whether tobacco is smoked or chewed.
Carcinogens in Tobacco: Oral Cavity-Specific
Robbins & Kumar provides a dedicated organ-specific table of tobacco carcinogens (Robbins & Kumar Basic Pathology, Table 7.4):
| Form of Tobacco | Carcinogens |
|---|---|
| Smoking | Polycyclic aromatic hydrocarbons (PAHs), Nicotine-derived nitrosamine ketone (NNK), N'-Nitrosonornicotine (NNN) |
| Chewing tobacco | NNK, NNN, ²¹⁰Polonium |
Key Carcinogens Explained
-
Polycyclic Aromatic Hydrocarbons (PAHs) - e.g., benzopyrene
- Generated by combustion of tobacco
- Metabolized by cytochrome P450 enzymes into reactive epoxide intermediates
- These intermediates form bulky DNA adducts at guanine bases
- Result: point mutations in critical oncogenes and tumor suppressor genes (especially TP53)
-
Tobacco-Specific Nitrosamines (TSNAs)
- NNK (4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone) - present in both smoked and smokeless tobacco
- NNN (N'-nitrosonornicotine) - particularly high in smokeless/chewing tobacco
- Mechanism: nitrosamines are metabolically activated to methylating and pyridyloxobutylating agents that alkylate DNA (O6-methylguanine), leading to G→A transition mutations and miscoding
-
²¹⁰Polonium - a radioactive alpha-emitter present in smokeless tobacco; causes direct DNA strand breaks
-
Nicotine - not directly a carcinogen, but acts as a tumor promoter - stimulates nicotinic acetylcholine receptors, activates anti-apoptotic pathways, and promotes angiogenesis and tumor cell proliferation
-
Phenol - another tumor promoter found in tobacco tar; causes mucosal irritation and promotes initiated cells
Mechanism of Carcinogenesis in Oral Cavity
Step 1 - Initiation (DNA Mutation)
PAHs and nitrosamines are metabolized in oral mucosal epithelial cells. The reactive metabolites form DNA adducts, causing:
- TP53 mutations (most common) - loss of apoptosis and cell cycle arrest
- RAS gene mutations - uncontrolled proliferation
- NOTCH gene mutations - impaired squamous differentiation
DNA sequencing of tobacco-associated oral cancers consistently shows a mutational signature characteristic of carcinogen exposure.
Step 2 - Field Cancerization
Years of chronic mucosal exposure to tobacco carcinogens lead to the concept of "field cancerization" - multiple independent neoplastic clones develop across wide areas of the oral mucosa. This explains:
- Multiple simultaneous primary tumors
- Development of new primary tumors at 3-7% per year after initial diagnosis
Step 3 - Precancerous Lesions
The carcinogen-induced mutations accumulate, producing:
- Leukoplakia (white plaques) - 5-25% are dysplastic; tobacco use (including smokeless) is the most important risk factor
- Erythroplakia (red velvety patches) - malignant transformation in >50% of cases
- Both show a spectrum from hyperkeratosis → dysplasia → carcinoma in situ
Step 4 - Invasive Carcinoma
Fully established oral SCC shows:
- Invasion through the basement membrane into connective tissue stroma
- Histologically: nests and islands of malignant keratinocytes with keratin pearl formation (in well-differentiated tumors)
- Preferential sites for carcinogen-associated cancers: ventral surface of tongue, floor of mouth, lower lip, soft palate, and gingiva
Gross and Histological Appearance
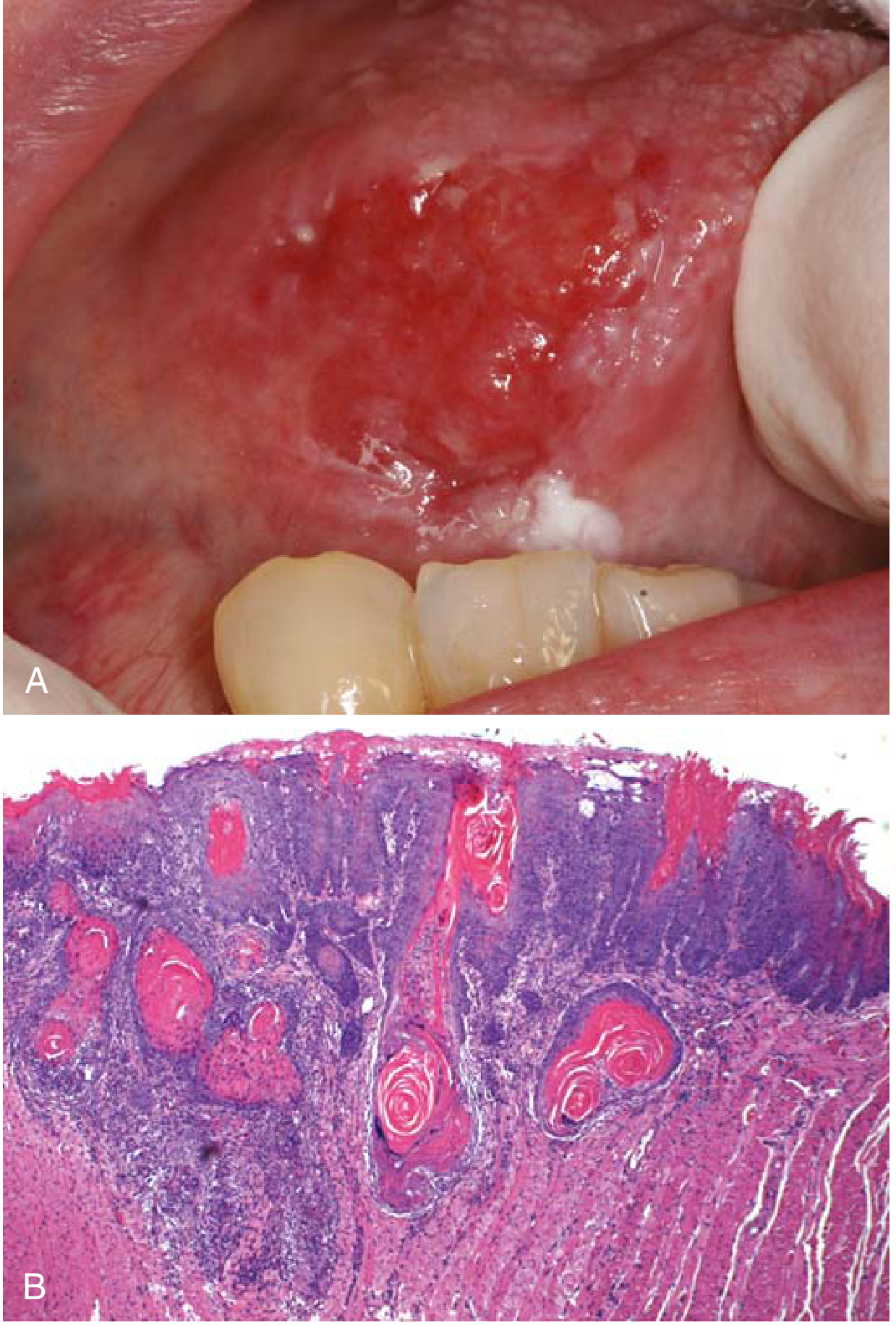
FIG. 13.4 Oral squamous cell carcinoma. (A) Gross appearance - ulceration and induration of oral mucosa. (B) Histologic appearance - nests and islands of malignant keratinocytes invading the connective tissue stroma with keratin pearls.
Systemic Effects of Tobacco (broader context)
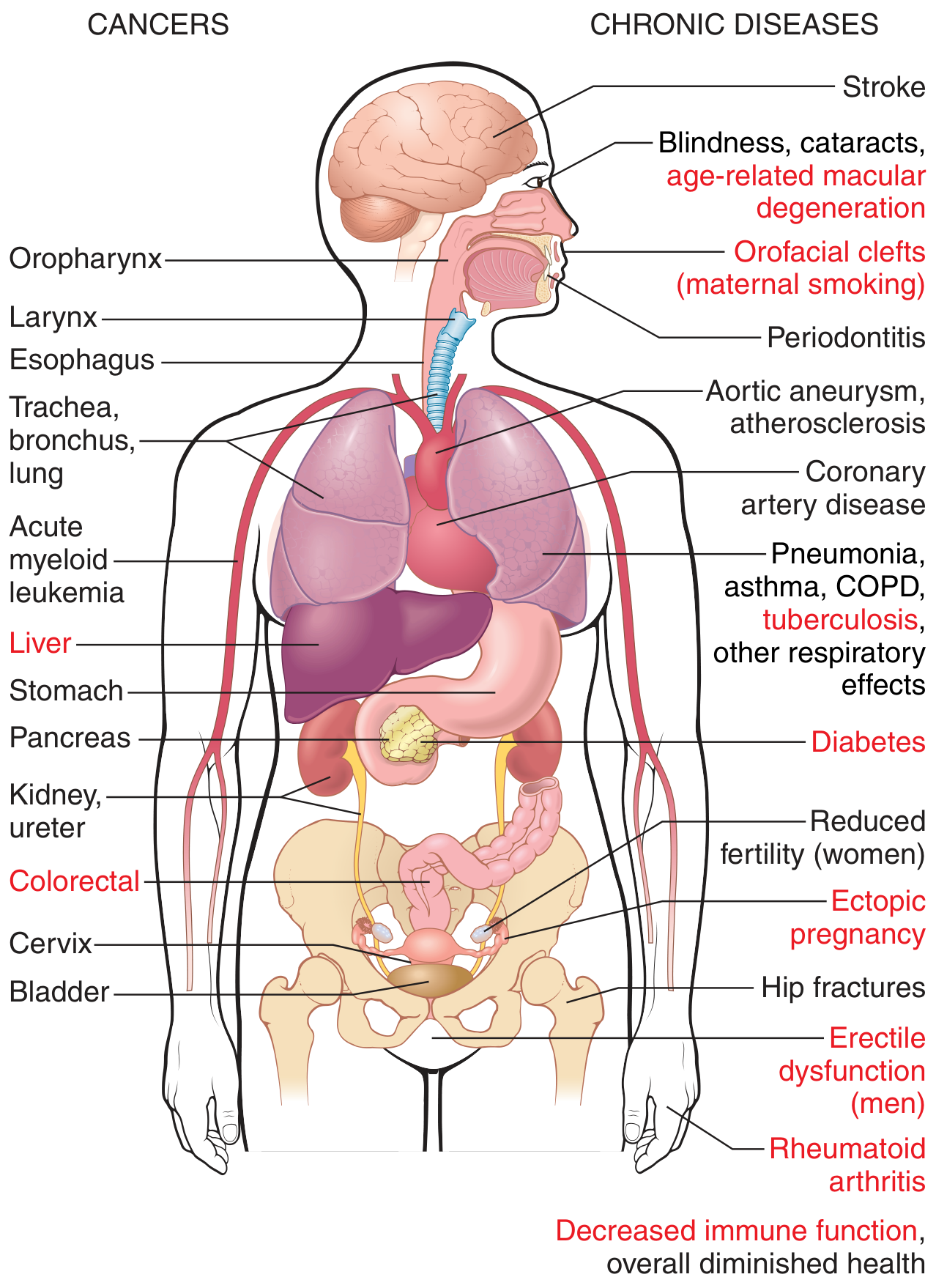
FIG. 7.9 Cancers and chronic diseases causally linked to smoking, including oropharynx, larynx, and esophagus.
Two Pathogenic Pathways of Oral SCC (Contrast)
| Feature | Tobacco/Carcinogen-Associated | HPV-Associated |
|---|---|---|
| Main cause | Tobacco, alcohol, betel nut (paan) | High-risk HPV (especially HPV-16) |
| Mechanism | DNA adducts → TP53/RAS/NOTCH mutations | E6 inhibits p53; E7 inhibits RB |
| Mutation burden | High | Low |
| p16 expression | Absent/low | Overexpressed |
| Location | Ventral tongue, floor of mouth, lip | Tonsil, base of tongue |
| Response to immunotherapy | Good (high neoantigen burden) | Better prognosis overall |
Clinical Features & Prognosis
- Overall 5-year survival is only 50%, largely due to late diagnosis
- Treated with surgery + radiation ± chemotherapy
- Carcinogen-associated tumors respond to immune checkpoint inhibitors due to high tumor neoantigen burden
- Tobacco cessation is the most effective primary prevention strategy
Sources: Robbins & Kumar Basic Pathology (Table 7.3, Table 7.4, pp. 540-541); Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.