Mitral stenosis medicine notes along with the homeopathic approach.
Reading File
Finding Sources
Searching the Web
mitral stenosis homeopathic treatment remedies
Searching PubMed
"mitral stenosis"[MeSH Terms] AND management
Reading File
Reading File
Reading Web Page
https://hpathy.com/cause-symptoms-treatment/mitral-stenosis/
Finding Sources
Searching Images
mitral stenosis echocardiography chest X-ray diagram
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive information from Harrison's, Braunwald's, and Fuster & Hurst's, along with homeopathic sources. Let me compile the complete notes.
Mitral Stenosis — Complete Medicine Notes with Homeopathic Approach
OVERVIEW
Mitral stenosis (MS) is a narrowing of the mitral valve orifice that obstructs blood flow from the left atrium (LA) to the left ventricle (LV) during diastole. Normal mitral valve area (MVA) is 4–6 cm². Symptoms typically appear when MVA falls below 2 cm², and severe obstruction exists at <1.5 cm² (critical: <1.0 cm²).
ETIOLOGY
| Cause | Notes |
|---|---|
| Rheumatic fever (most common) | ~90% of cases; group A β-hemolytic streptococcal infection triggers autoimmune valve damage; 3:1 female preponderance |
| Degenerative (Mitral Annular Calcification) | Increasing in developed nations; age-related; more in older women |
| Congenital MS | Rare; parachute mitral valve, supravalvular ring |
| Infective endocarditis | Vegetation rarely causing obstruction |
| Radiotherapy-induced MS | Fibrotic commissural fusion post-thoracic radiation |
Epidemiology: ~39 million cases of rheumatic heart disease worldwide; MS prevalent in developing nations (20–30/1000 school children on echo screening). In developed nations, prevalence is 0.02% due to antibiotic prophylaxis and improved socioeconomic conditions. — Fuster & Hurst's The Heart, 15th Ed.
PATHOPHYSIOLOGY
The sequence of hemodynamic events:
- Commissural fusion, leaflet thickening & calcification → ↓ MVA
- Persistent diastolic pressure gradient across the mitral valve (LA > LV)
- Left atrial enlargement and elevated LA pressure
- Pulmonary venous hypertension → pulmonary edema (dyspnea)
- Reactive pulmonary arterial hypertension (PAH) → RV hypertrophy and failure
- LA dilation + stasis → atrial fibrillation (AF) and thromboembolism (stroke)
Key hemodynamic formulae:
- Transmitral gradient increases with tachycardia (less diastolic filling time)
- CO can be normal at rest but fails to increase with exercise
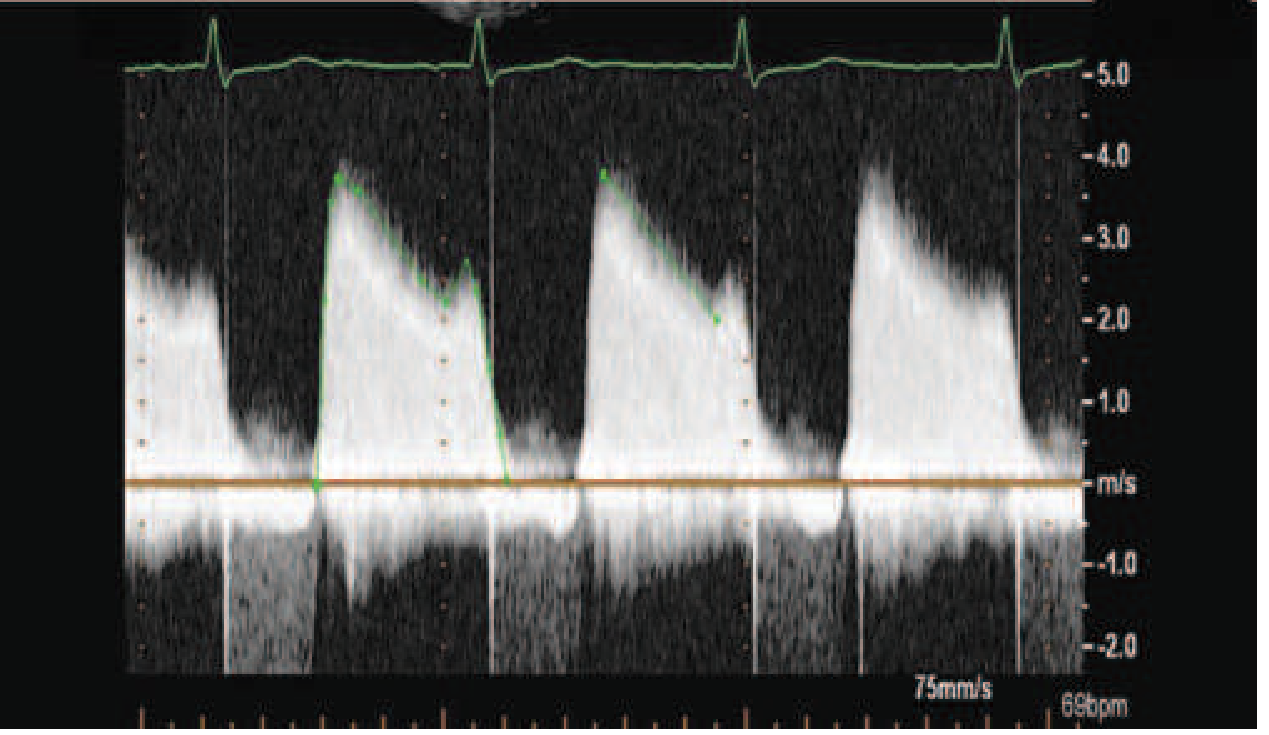
- MVA by pressure half-time (PHT): MVA = 220 / PHT
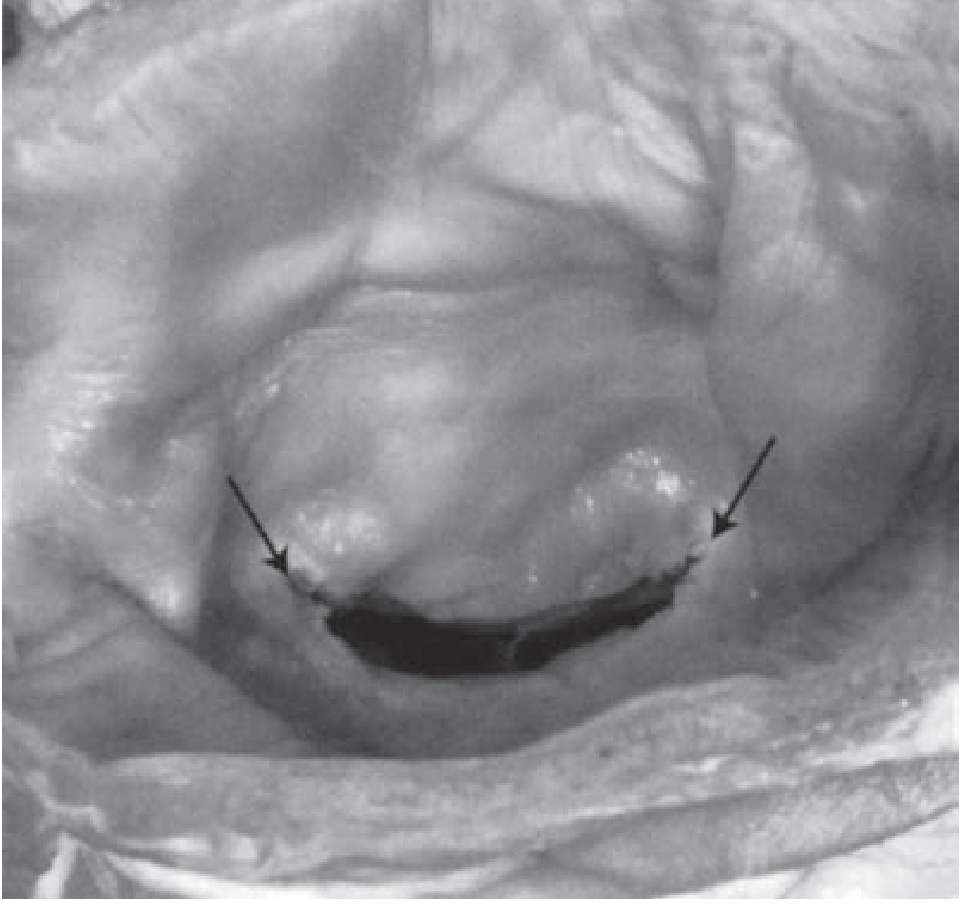
The "fish mouth" appearance of the stenotic valve on gross pathology is characteristic (shown in Fuster & Hurst below).
SEVERITY GRADING (AHA/ACC)
| Severity | MVA (cm²) | Mean Gradient (mmHg) | PASP (mmHg) |
|---|---|---|---|
| Mild | >1.5 | <5 | <30 |
| Moderate | 1.0–1.5 | 5–10 | 30–50 |
| Severe | <1.0 | >10 | >50 |
CLINICAL FEATURES
Symptoms
- Dyspnea on exertion → orthopnea → PND (earliest and most common)
- Hemoptysis — due to rupture of pulmonary-bronchial venous anastomoses
- Palpitations — AF is the most common arrhythmia
- Systemic embolism — stroke, TIA (especially with AF)
- Hoarseness — Ortner's syndrome: LA enlargement compressing recurrent laryngeal nerve
- Chest pain — uncommon; due to PAH or coexistent CAD
- Fatigue — low cardiac output state
- Recurrent bronchitis
Signs
- Malar flush ("mitral facies") — dilated capillaries in the cheeks due to low CO
- Tapping apex — palpable loud S1
- Parasternal heave — RV enlargement (sign of PAH)
- Diastolic thrill (rare)
Auscultation (Classic Triad)
- Loud S1 — due to abrupt tensing of stiffened mitral leaflets
- Opening Snap (OS) — follows A2 by 0.05–0.12 s; shorter A2–OS interval = more severe MS
- Low-pitched mid-diastolic rumbling murmur — best heard at apex with bell, patient in left lateral decubitus, accentuated by mild exercise; presystolic accentuation in sinus rhythm
Other sounds:
- Loud P2, closely split S2 (PAH)
- Graham Steell murmur — high-pitched, early diastolic decrescendo along left sternal border (pulmonary regurgitation due to PAH)
- Functional TR murmur (pansystolic, louder on inspiration — Carvallo's sign)
Note: In severe MS with very low CO, the murmur may become inaudible ("silent MS"). — Harrison's Principles of Internal Medicine, 22nd Ed.
INVESTIGATIONS
ECG
- P-mitrale (bifid P in lead II, width >0.12 s) — LA enlargement in sinus rhythm
- Tall, peaked P in lead V1 (negative terminal deflection)
- AF — most common arrhythmia in established MS
- RV hypertrophy pattern (right axis deviation, dominant R in V1) if PAH
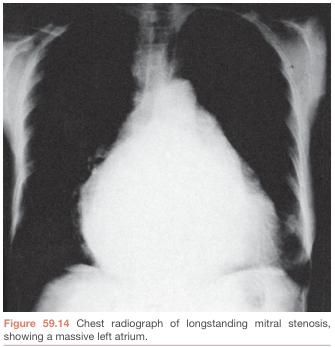
Chest X-Ray
- LA enlargement — double shadow at right heart border, elevated left main bronchus, left atrial appendage prominence (straightening of left heart border)
- Pulmonary venous hypertension — upper lobe diversion, Kerley B lines, interstitial edema
- Mitral valve calcification
- RV enlargement (loss of retrosternal airspace on lateral)
Echocardiography (Investigation of Choice)
- 2D echo: Doming ("hockey stick") of anterior mitral leaflet; restricted posterior leaflet; commissural fusion; calcification; Wilkins score
- Doppler: Mean transmitral gradient, PHT-derived MVA; assess PAH (TR jet velocity)
- Planimetry: Direct MVA measurement
- TEE: Exclude LA appendage thrombus before valvuloplasty or cardioversion
Wilkins Echocardiographic Score (each criterion scored 0–4, max 16):
- Leaflet mobility
- Leaflet thickening
- Subvalvular thickening
- Calcification
Score ≤8: favorable for Balloon Mitral Valvotomy (BMV)
Cardiac Catheterization
- Reserved when echo inconclusive or discordant with symptoms
- Pre-op coronary angiography in those with risk factors or age >40
NATURAL HISTORY
- Long asymptomatic latent period (20–40 years in developed nations; can be as short as 5 years in developing nations)
- Once symptoms develop, untreated prognosis is poor:
- NYHA II: 10-year survival 69%
- NYHA III: 10-year survival 33%
- NYHA IV: 10-year survival 0%
- MVA declines ~0.09 cm²/year on average
- Complications: AF (~30–40%), systemic embolism, pulmonary hypertension, RV failure
MANAGEMENT
A. Medical Management
1. Prevention (Primary & Secondary)
- Penicillin prophylaxis against Group A Strep (rheumatic fever secondary prevention) — lifelong in at-risk patients
- Infective endocarditis prophylaxis in high-risk patients
2. Symptom Relief
- Salt restriction + oral diuretics (loop diuretics: furosemide; thiazides) — reduce pulmonary congestion, relieve dyspnea
- Avoid strenuous exertion
3. Rate Control in AF (critical — tachycardia worsens hemodynamics)
- Beta-blockers (metoprolol, bisoprolol) — first line; also useful during pregnancy
- Non-DHP calcium channel blockers — verapamil, diltiazem
- Digoxin — useful in AF with heart failure, less effective for exercise-induced tachycardia
4. Rhythm Control
- Cardioversion (electrical or pharmacological) in recent-onset AF
- Requires ≥3 weeks of therapeutic anticoagulation (INR 2–3) OR TEE to exclude LA thrombus before cardioversion
- Less successful if LA markedly enlarged or AF >1 year
5. Anticoagulation
- Warfarin (Vitamin K antagonist), target INR 2–3 — indicated in:
- MS + AF (paroxysmal or permanent)
- Prior thromboembolism
- LA thrombus on echo
- ⚠️ NOACs (e.g., rivaroxaban) are NOT recommended in rheumatic MS with AF — a randomized trial showed significantly higher mortality compared to warfarin (Harrison's 22nd Ed.)
- Controversial in sinus rhythm with LA >5.5 cm
Medical therapy relieves symptoms but does NOT correct the underlying mechanical obstruction. Definitive treatment requires intervention. — Fuster & Hurst's The Heart, 15th Ed.
B. Interventional / Surgical Management
Indications for intervention (AHA/ACC):
- Symptomatic (NYHA II–IV) severe MS (MVA <1.5 cm²)
- Asymptomal severe MS with new-onset AF, PAH (PASP >50 mmHg), or desire for pregnancy
1. Percutaneous Mitral Balloon Commissurotomy (PMBC) / Balloon Mitral Valvotomy (BMV)
- Procedure of choice when anatomy is favorable
- Technique: Inoue balloon inflated across mitral valve via transseptal puncture
- Contraindications: MVA >1.5 cm², LA thrombus, MR >grade 2, severe calcification (Wilkins score >8), significant commissural calcification
- Results: MVA doubles, mean gradient halves
- Complications: MR (~3%), tamponade (~1%), embolism (~1%), mortality (<1%)
- Long-term: 80–90% event-free survival at 5–7 years with favorable anatomy
2. Surgical Mitral Commissurotomy (Closed / Open)
- Open commissurotomy: direct visualization on cardiopulmonary bypass
- Preferred when BMV contraindicated but valve not too diseased for repair
3. Mitral Valve Replacement (MVR)
- Indicated when leaflets too calcified/distorted for commissurotomy
- Options: mechanical valve (lifelong anticoagulation) vs. bioprosthetic valve
- Perioperative mortality: 1–3% (higher in older patients with PAH or LV dysfunction)
- Transcatheter mitral replacement (TMVR) under evaluation for degenerative MS/MAC
Management Flowchart (Harrison's 22nd Ed.):
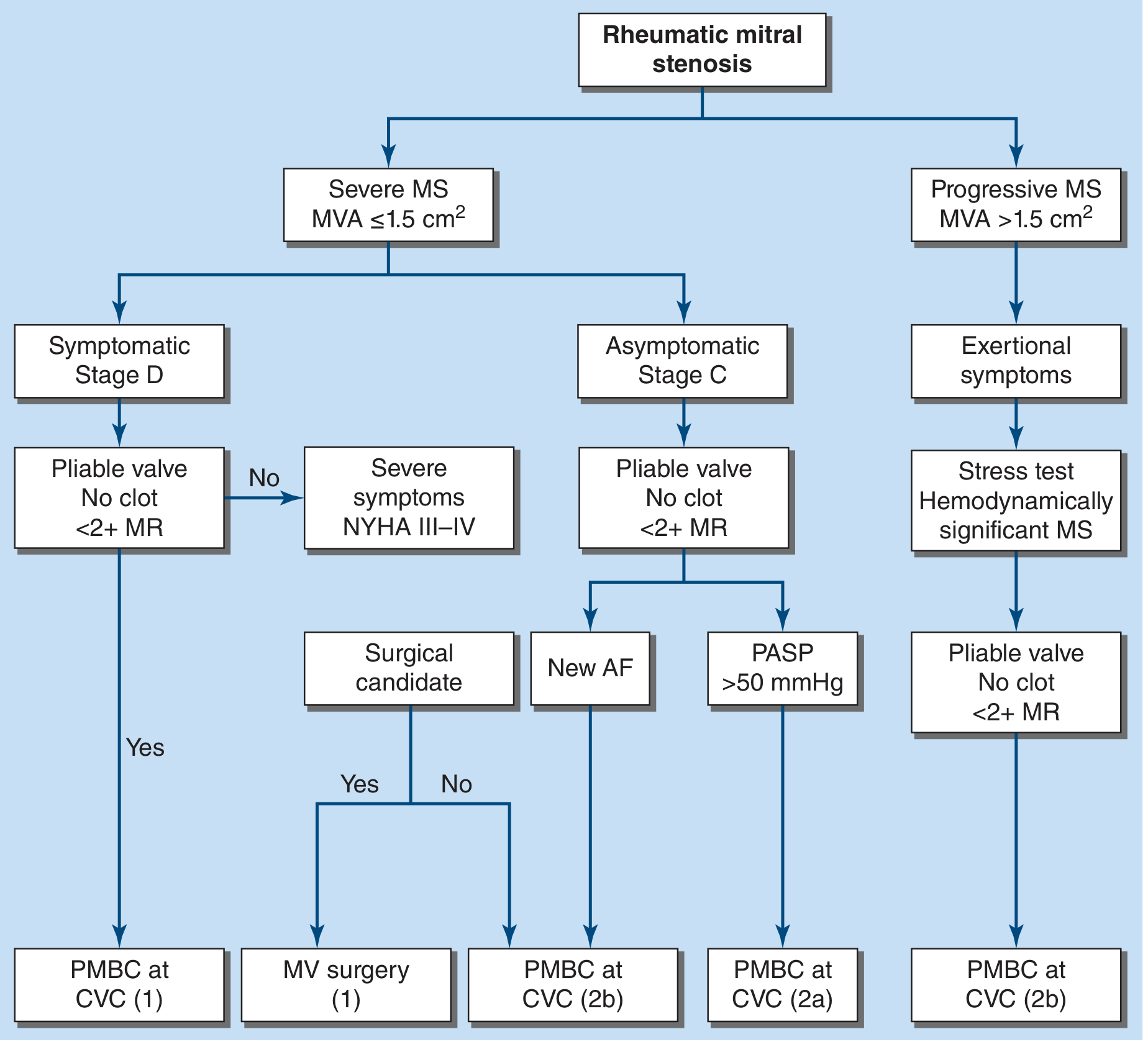 Rheumatic MS management flowchart per ACC/AHA 2021 guidelines — Harrison's 22nd Ed.
Rheumatic MS management flowchart per ACC/AHA 2021 guidelines — Harrison's 22nd Ed.
Special Situations
Pregnancy + MS
- Physiological increases in HR and blood volume → may precipitate acute decompensation
- Beta-blockers are the mainstay for symptom control
- BMV is preferred intervention if needed; preferably after 20 weeks, with fetal lead shielding
- MVR carries high fetal risk
COMPLICATIONS
| Complication | Mechanism |
|---|---|
| Atrial fibrillation | LA dilation → conduction remodeling |
| Systemic thromboembolism | LA stasis, especially in AF |
| Pulmonary arterial hypertension | Reactive pulmonary vasoconstriction |
| Right heart failure | Chronic PAH |
| Infective endocarditis | Turbulent flow, abnormal endothelium |
| Hemoptysis | Pulmonary venous hypertension |
| Ortner's syndrome | Hoarseness from LA compression of left RLN |
HOMEOPATHIC APPROACH TO MITRAL STENOSIS
Important clinical note: Homeopathy does not reverse structural valve stenosis or calcification. In the homeopathic framework, remedies are selected based on individualization — matching the totality of physical, mental, and general symptoms of the patient (not just the disease label). Homeopathic care is considered supportive/complementary; all patients with moderate-to-severe MS must receive conventional cardiological management.
Commonly Indicated Homeopathic Remedies
| Remedy | Key Indications in Cardiac/MS Context |
|---|---|
| Digitalis purpurea | Slow, very irregular, weak pulse; extreme exhaustion on slight motion; cardiac failure; cyanosis; patient fears heart will stop |
| Naja tripudians | Chronic valvular lesions; hypertrophied heart; oppression of chest; pulse irregular in force but regular in rhythm; sympathetic cough in rheumatic carditis; prostration; mental depression |
| Cactus grandiflorus | Constriction as of an iron band around chest; mitral insufficiency; cardiac incompetence; palpitations; precordial dullness; endocarditis |
| Spigelia anthelmia | Violent palpitation; trembling sensation in the chest; dyspnea; pain radiating to left arm; worse motion, left side; stitching pains in chest |
| Laurocerasus | Cyanosis; dyspnea with gasping; feeble, irregular pulse; cardiac failure; cold extremities; cold sweat |
| Kalmia latifolia | Cardiac symptoms after rheumatism; sharp pain in heart with extreme dyspnea and anguish; palpitation worse leaning forward; bradycardia (35–40 bpm) |
| Apis mellifica | Edema; anasarca; general fluid retention; oliguria; "feels each breath will be the last"; mitral insufficiency; organic heart disease |
| Aurum metallicum | Palpitation and cardiac hypertrophy; oppressive sensation; hypertension with heart disease; depression, tendency to despair |
| Adonis vernalis | Mitral and aortic regurgitation; rheumatic endocarditis; fatty heart; pericarditis; rapid irregular pulse; dyspnea; cardiac asthma |
| Arsenicum album | Prostration; anxiety and restlessness; dyspnea worse lying down; edema; palpitations with anxiety; worse at midnight |
| Spongia tosta | Dyspnea and wheezing (cardiac asthma); valvular disease; palpitation on ascending stairs |
| Lithium carbonicum | Rheumatic soreness in cardiac region; sudden shock in heart; throbbing and dull stitch in cardiac region; pains before urination |
| Rhus toxicodendron | Cardiac damage after rheumatic fever; palpitations; restlessness; valvular disease; worse cold and damp |
| Baryta carbonica | Elderly patients with hypertension and valve disease; palpitation; weakness |
| Crataegus oxyacantha | "Hawthorn" — cardiac tonic; strengthens heart muscle; used in cardiac failure, valvular disease; dyspnea on exertion |
Repertory References for Valvular Disease
From the Homoeopathic Repertory:
- Circulatory system – valvular disease: Acon., Adon. v., Apoc., Ars., Ars. iod., Aur. br., Aur. iod., Aur. m., Cact., Calc. fl., Camph., Conv., Crat., Dig., Ferr., Galanth., Glon., Iod., Kal., Lach., Laur., Lith. c., Lycop., Naja, Ox. ac., Phos., Plumb., Rhus. t., Sang., Serum ang., Spig., Spong., Stigm., Stroph., Thyr., Viscum.
Homeopathic Principles Applied to MS
- Individualization — Remedy selection is based on the complete symptom picture (mental, general, local), not on the diagnosis alone
- Miasmatic understanding — Rheumatic MS is viewed through the Psora-Sycosis-Syphilis miasmatic framework; Sycotic and Syphilitic miasms often implicated in structural degeneration
- Constitutional remedies — A deep-acting constitutional remedy (e.g., Aurum met., Calc. carb., Lycopodium) may be indicated for the underlying predisposition
- Organotropic remedies — Naja, Digitalis, Cactus, Crataegus are considered specific to the heart
- Intercurrent / Anti-miasmatic remedies — Medorrhinum, Syphilinum, Tuberculinum may be needed intercurrently
SUMMARY TABLE
| Domain | Key Points |
|---|---|
| Most common cause | Rheumatic fever (Group A Strep) |
| Hallmark murmur | Low-pitched mid-diastolic rumble at apex + loud S1 + OS |
| Best investigation | 2D/Doppler echocardiography |
| Medical Rx: rate | Beta-blockers, verapamil, diltiazem, digoxin |
| Medical Rx: HF | Diuretics + salt restriction |
| Anticoagulation | Warfarin (INR 2–3) for AF/embolism; NOACs avoided |
| Intervention of choice | BMV/PMBC (if Wilkins score ≤8, no LA clot, MR ≤2+) |
| Surgery | MVR for unsuitable anatomy |
| Homeopathic pillars | Naja, Digitalis, Cactus, Spigelia, Crataegus, Aurum met. |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) — Management, physical findings, treatment algorithm
- Fuster & Hurst's The Heart, 15th Ed. — Etiology, pathophysiology, natural history, BMV
- Braunwald's Heart Disease, 10th Ed. — Pathology, diagnosis, treatment
- Homeobook.com / Hpathy.com — Homoeopathic management (Dr. Naziya G.M. Naik; Dr. Manisha Sachdeva)
Find me the flashcard of aortic regurgitation.
Reading File
Searching the Web
aortic regurgitation flashcard medical mnemonics key points
Finding Sources
Reading Web Page
https://www.medicowesome.com/2016/01/signs-seen-in-aortic-re…
Finding Sources
Searching Images
aortic regurgitation peripheral signs echocardiography diagnosis
Reading File
Reading File
Finding Sources
I now have all the key content needed. Here is the complete Aortic Regurgitation flashcard:
🃏 AORTIC REGURGITATION — FLASHCARD
CARD 1 — DEFINITION & BASICS
| Definition | Incompetence of the aortic valve → backflow of blood from aorta into LV during diastole |
| Also called | Aortic insufficiency (AI) |
| Prevalence | ~4.9% overall; moderate-severe ~0.5% (Framingham data) |
| Key haemodynamic lesion | Volume overload of the LV (± afterload excess) |
CARD 2 — ETIOLOGY
Mnemonic: "CREAM" for valve leaflet causes + aortic root causes
Valve Leaflet Causes
| Cause | Notes |
|---|---|
| Bicuspid aortic valve | Most common congenital cause |
| Infective endocarditis | Most common cause of acute AR |
| Rheumatic heart disease | Often with mitral disease |
| Calcific degeneration | Degenerative, elderly |
| Dopamine/serotonin agonists | Drug-induced |
Aortic Root Causes
| Cause | Notes |
|---|---|
| Marfan syndrome | Annuloaortic ectasia |
| Hypertension | Aortic root dilation |
| Aortic dissection | Acute AR → emergency |
| Syphilis | Obliterative endarteritis of vasa vasorum |
| Ankylosing spondylitis / Psoriatic arthritis | Seronegative arthropathy |
| Idiopathic root dilation | Most common cause in developed nations |
Acute AR causes: Endocarditis + Aortic Dissection (remember: "E-D")
CARD 3 — PATHOPHYSIOLOGY
Chronic AR (Compensated → Decompensated)
Incompetent aortic valve
↓
LV receives normal LA inflow + regurgitant volume
↓
Volume overload → Eccentric LV hypertrophy (LV dilates)
↓
↑ Stroke volume → ↑ Systolic BP → Wide pulse pressure
↓
Afterload excess → Concentric + eccentric hypertrophy
↓ (years later)
LV systolic dysfunction → Heart failure symptoms
Acute AR (Decompensated from the start)
- No time for LV compensation → sudden ↑ LVEDP
- ↓ Cardiac output + ↑ pulmonary pressure → Pulmonary oedema + shock
- Reflex vasoconstriction raises SVR (makes it worse)
- Medical emergency — early surgery needed
CARD 4 — SYMPTOMS
| Chronic AR | Acute AR |
|---|---|
| Long asymptomatic period | Sudden severe dyspnoea |
| Dyspnoea on exertion (first symptom) | Cardiogenic shock |
| Orthopnoea, PND | Pulmonary oedema |
| Fatigue | Tachycardia, hypotension |
| Angina (less common than AS) | Rapidly fatal if untreated |
| Palpitations (awareness of heartbeat) | |
| Carotid artery pain | |
| Neck pulsations |
CARD 5 — PERIPHERAL SIGNS (The Famous Eponyms)
Mnemonic: "WCDQ-MT" — Water hammer, Corrigan, De Musset, Quincke, Müller, Traube
| Sign | Description | How to Elicit |
|---|---|---|
| Corrigan's pulse (Water hammer pulse) | Rapid rise + sharp collapse of carotid/radial pulse | Feel the radial pulse with wrist elevated |
| De Musset's sign | Head nodding/bobbing with each heartbeat | Observe head at rest |
| Quincke's sign | Capillary pulsations at proximal nail bed | Press lightly on fingernail tip — alternating flush/blanch |
| Duroziez's sign | Systolic + diastolic bruit ("to-and-fro") over femoral artery | Press stethoscope on femoral artery |
| Traube's sign | Pistol-shot sound over the femoral artery | Auscultation over femoral |
| Müller's sign | Pulsation of the uvula | Inspect open mouth |
| Hill's sign | Popliteal BP > brachial BP by >20 mmHg (>60 mmHg = severe) | BP in arm and leg |
| Landolfi's sign | Alternating constriction and dilation of the pupil | Inspect pupils |
| Becker's sign | Visible pulsations of retinal arterioles | Fundoscopy |
| Lighthouse sign | Flushing and blanching of the forehead | Observe forehead |
| Mayne's sign | >15 mmHg drop in diastolic BP on raising arm | BP measurement |
| Rosenbach's sign | Pulsating liver | Palpate liver |
All these signs reflect the wide pulse pressure and hyperdynamic circulation from the high stroke volume.
CARD 6 — CARDIAC EXAMINATION
| Feature | Finding |
|---|---|
| Apex beat | Displaced downward & laterally; hyperdynamic, volume-overloaded character |
| S1 | Normal or soft |
| S2 | Soft A2 (leaflet not closing properly) |
| Murmur | High-pitched, blowing, early diastolic decrescendo murmur at left lower sternal border (LLSB) / 3rd ICS |
| Best heard | Patient sitting forward, breath held in expiration |
| Austin Flint murmur | Low-pitched mid-diastolic rumble at apex (regurgitant jet impinges on mitral valve causing it to vibrate — mimics mitral stenosis but no OS) |
| Systolic murmur | May be present (high flow ejection murmur across aortic valve — does NOT mean AS) |
In acute AR: murmur is short and soft (LV pressure rises rapidly, equalizes with aorta early in diastole) — easily missed!
CARD 7 — INVESTIGATIONS
ECG
- LV hypertrophy pattern (tall R in V5–V6, deep S in V1–V2)
- Left axis deviation
- ST-T changes (strain pattern)
- Normal in early/mild AR
Chest X-Ray
- Cardiomegaly — enlarged LV ("boot-shaped" or globular heart)
- Aortic root dilation (prominent aortic knuckle)
- In acute AR: pulmonary oedema with near-normal heart size
Echocardiography (Gold Standard)
- 2D: LV dilation, LV function, aortic root size, leaflet morphology, vegetations
- Colour Doppler: regurgitant jet width/area in LVOT
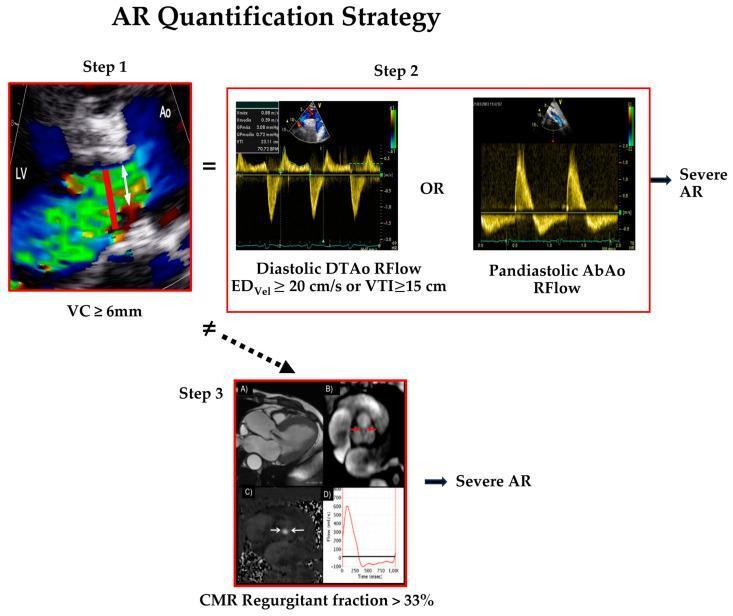
- Vena contracta ≥6 mm → severe AR
- Holodiastolic flow reversal in descending/abdominal aorta → severe AR
- Pressure half-time (PHT) <200 ms → severe AR (rapid equalization)
- LV dimensions: LVESD >50 mm or LVEDD >65 mm → surgical threshold
Cardiac Catheterization
- Aortography when echo is inconclusive
- Coronary angiography pre-op (age >40 or risk factors)
CARD 8 — SEVERITY GRADING
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Vena contracta (cm) | <0.3 | 0.3–0.6 | >0.6 |
| Regurgitant fraction | <30% | 30–50% | >50% |
| Regurgitant volume (mL/beat) | <30 | 30–60 | >60 |
| PHT (ms) | >500 | 200–500 | <200 |
| Holodiastolic reversal | Absent/brief | Present | Pandiastolic |
CARD 9 — MANAGEMENT
Acute AR — Emergency
- IV vasodilators (sodium nitroprusside) + inotropes (dobutamine)
- No IABP (contraindicated — worsens regurgitation in diastole)
- Urgent/Emergency aortic valve replacement (AVR) — medical management alone = high mortality
- Treat underlying cause (antibiotics for endocarditis, surgery for dissection)
Chronic AR — Medical
| Drug | Indication |
|---|---|
| Vasodilators (ACE inhibitors, nifedipine, hydralazine) | Symptomatic AR not yet ready for surgery; asymptomatic with LV dilation/hypertension |
| Beta-blockers | Avoid in pure AR (slow HR → longer diastole → more regurgitation time); used in Marfan syndrome for aortic root protection |
| Diuretics / Digoxin | Symptomatic heart failure relief |
| Penicillin prophylaxis | Secondary prevention of rheumatic fever |
| Endocarditis prophylaxis | High-risk patients per guidelines |
Note: Vasodilators reduce afterload, decrease regurgitant volume and are the cornerstone of medical management. — Goldman-Cecil Medicine
Chronic AR — Surgical: Indications for AVR (AHA/ACC)
| Indication | Class |
|---|---|
| Symptomatic severe AR (NYHA II–IV) | I |
| Asymptomatic severe AR + LVEF <55% | I |
| Asymptomatic severe AR + LVESD >50 mm or LVEDD >65 mm | IIa |
| Severe AR undergoing other cardiac surgery | I |
| Severe AR + aortic root ≥5.5 cm (Marfan: ≥5.0 cm) | I |
Valve replacement should occur before irreversible ventricular dysfunction — serial echo surveillance is key. — Fuster & Hurst's The Heart, 15th Ed.
CARD 10 — ACUTE vs. CHRONIC: QUICK COMPARISON
| Feature | Chronic AR | Acute AR |
|---|---|---|
| Onset | Gradual | Sudden |
| LV size | Enlarged | Normal |
| Pulse pressure | Wide | Normal/slightly wide |
| Murmur | Long, prominent | Short, soft (easily missed) |
| Apex | Displaced, hyperdynamic | Normal position |
| Compensation | Eccentric hypertrophy | None |
| Presentation | Exertional dyspnoea | Shock + pulmonary oedema |
| Urgency | Elective | Emergency |
CARD 11 — KEY MNEMONICS
Causes mnemonic: "CREAM + MHSAI"
- Congenital (bicuspid), Rheumatic, Endocarditis, Ankylosing spondylitis, Marfan's
- Marfan, Hypertension, Syphilis, Aortic dissection, Idiopathic
Peripheral signs mnemonic: "WCDQ + TMB"
- Water hammer, Corrigan, De Musset, Quincke, Traube, Müller, Becker
Austin Flint vs. MS:
Austin Flint = no Opening Snap, no LA enlargement, no P-mitrale on ECG
Murmur location memory:
AR = After S2 → At Left Lower Sternal Border = "A-LLSB"
Sources: Goldman-Cecil Medicine; Rosen's Emergency Medicine; Fuster & Hurst's The Heart, 15th Ed.; Morgan & Mikhail's Clinical Anaesthesiology, 7th Ed.; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.