Diabetic retinopathy complete detailed information for rguhs university exams refer ak khurana
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
diabetic retinopathy fundus classification proliferative
Finding Sources
I now have all the material needed for a comprehensive answer. Let me compile the complete detailed information on Diabetic Retinopathy for RGUHS exams, structured in AK Khurana style.
Diabetic Retinopathy — Complete Detailed Notes (RGUHS Exam Format)
Based on AK Khurana's Comprehensive Ophthalmology & Kanski's Clinical Ophthalmology 10th Ed.
INTRODUCTION
Diabetic retinopathy (DR) is the commonest cause of new blindness in most industrialised countries in working-age adults. With effective screening and treatment (ETDRS guidelines + anti-VEGF), the risk of severe visual loss can be reduced to less than 5%.
OPHTHALMIC COMPLICATIONS OF DIABETES
Common
- Diabetic maculopathy (oedema + ischaemia)
- Retinopathy (neovascularisation of disc/retina, vitreous haemorrhage)
- Unstable refraction (osmotic lens changes)
Uncommon
- Recurrent styes; xanthelasma
- Accelerated age-related cataract
- Tractional retinal detachment
- Neovascularization of iris and angle → Neovascular glaucoma (NVG)
- Ocular motor nerve palsies (3rd, 4th, 6th)
- Reduced corneal sensitivity
Rare
- Diabetic papillopathy
- Acute-onset cataract
- Wolfram syndrome (optic atrophy + neurological abnormalities)
- Rhino-orbital mucormycosis
PREVALENCE
- DR occurs in approximately 40% of all diabetics
- Type 2 diabetes: 67% prevalence at 10 years after diagnosis; 10% will have proliferative disease
- More common in Type 1 than Type 2 diabetes
RISK FACTORS (AK Khurana Mnemonic: DOGS-HP)
| Risk Factor | Details |
|---|---|
| Duration | Most important predictor. Rarely develops within 5 years of onset or before puberty |
| Obesity / glycaemia | Poor control — higher HbA1c = greater risk. DCCT/UKPDS trials confirm tight control prevents/delays DR |
| Genetics | Familial predisposition |
| Systemic hypertension | Accelerates progression of retinopathy; linked to macular oedema |
| Hyperlipidaemia | Increased risk of exudate formation and maculopathy |
| Pregnancy | Can accelerate DR (especially in pre-existing Type 1) |
Other factors: Anaemia, renal disease (nephropathy parallels retinopathy), smoking.
⚠️ A sudden improvement in diabetic control may paradoxically cause progression of retinopathy.
PATHOGENESIS
DR is primarily a microangiopathy — small blood vessels are particularly vulnerable to damage from chronic hyperglycaemia.
Key Mechanisms:
1. Biochemical Pathways of Hyperglycaemia-Induced Damage:
- Polyol pathway activation → sorbitol accumulation → osmotic damage
- Advanced Glycation End-products (AGEs) → basement membrane thickening
- Protein Kinase C (PKC) activation → increased vascular permeability
- Hexosamine pathway → endothelial dysfunction
- Oxidative stress → free radical damage
2. Structural Vascular Changes:
- Pericyte loss → earliest histological change; pericytes maintain capillary integrity and autoregulation
- Basement membrane thickening → barrier dysfunction
- Endothelial cell loss → breakdown of blood-retinal barrier
- Formation of acellular capillaries → capillary occlusion
3. Ischaemia & Neovascularization:
- Capillary occlusion → retinal ischaemia
- Ischaemia → upregulation of Vascular Endothelial Growth Factor (VEGF) (most important angiogenic mediator)
- VEGF → neovascularization (new vessel formation — abnormal, fragile, leaky)
CLASSIFICATION
ETDRS Classification (Modified Airlie House Classification — most widely used internationally):
| Category | Features | Management |
|---|---|---|
| No DR | No abnormalities | Review in 12 months |
| Very Mild NPDR | Microaneurysms only | Review in 12 months |
| Mild NPDR | Microaneurysms, retinal haemorrhages, exudates, CWS — up to moderate level; no IRMA | Review 6–12 months |
| Moderate NPDR | Severe haemorrhages (>ETDRS photo 2A) in 1 quadrant; CWS; mild IRMA | Review ~6 months |
| Severe NPDR (4-2-1 Rule) | Severe haemorrhages in 4 quadrants; venous beading in ≥2 quadrants; IRMA in ≥1 quadrant | Refer to ophthalmologist; PRP considered |
| Very Severe NPDR | Two or more of the above criteria | Early PRP recommended |
| PDR | Neovascularization (NVD/NVE) | PRP / anti-VEGF |
| High-Risk PDR | See below | Urgent PRP + anti-VEGF |
Simplified Clinical Classification (AK Khurana):
| Type | Features |
|---|---|
| Background DR (BDR) | Microaneurysms, dot & blot haemorrhages, hard exudates |
| Diabetic Maculopathy | Any retinopathy at macula; may be focal, diffuse, or ischaemic |
| Preproliferative DR (PPDR) | Cotton-wool spots, venous beading, IRMA, moderate-severe haemorrhages |
| Proliferative DR (PDR) | NVD (new vessels at disc), NVE (new vessels elsewhere) |
| Advanced Diabetic Eye Disease | Tractional RD, vitreous haemorrhage, neovascular glaucoma |
SIGNS — DETAILED
1. Background Diabetic Retinopathy
Microaneurysms:
- Earliest clinically detectable sign
- Small, round, red dots (~15–60 µm); lie in inner nuclear layer
- FA: early bright hyperfluorescence (leakage)
Dot & Blot Haemorrhages:
- Dot haemorrhages: in inner nuclear layer (may look like microaneurysms)
- Blot haemorrhages: in inner nuclear/outer plexiform layer; larger, darker
Flame-shaped haemorrhages: Nerve fibre layer haemorrhages (more common in hypertension)
Hard exudates (HE):
- Yellow-white deposits with sharp margins at outer plexiform layer
- Lipid/protein leakage from abnormal vessels
- Often arranged in rings (circinate pattern) around leaking microaneurysms
- FA: hypofluorescent (block fluorescence)
2. Diabetic Maculopathy (Clinically Significant Macular Oedema — CSMO)
ETDRS Definition of CSMO (any one of the following):
- Retinal thickening within 500 µm of centre of fovea
- Hard exudates within 500 µm of centre with adjacent retinal thickening
- Retinal thickening ≥1 disc area within 1 disc diameter of fovea
Types:
- Focal maculopathy: Ring of exudates temporal to macula; FA shows focal leakage at centre of ring
- Diffuse maculopathy: Diffuse retinal thickening, dot/blot haemorrhages throughout posterior pole; FA shows extensive hyperfluorescence
- Ischaemic maculopathy: Good fundal appearance but poor VA; FA shows enlarged foveal avascular zone (FAZ) with capillary dropout — worst prognosis
- Mixed maculopathy: Combination of oedematous + ischaemic
3. Preproliferative DR (PPDR)
Indicates severe retinal ischaemia with high risk of progression to PDR.
Cotton-Wool Spots (CWS):
- Fluffy white superficial lesions; nerve fibre layer infarcts
- Axoplasmic flow obstruction at capillary occlusions
Venous Changes:
- Generalised dilatation and tortuosity
- Venous beading (focal narrowing and dilatation — most specific sign of PPDR)
- Looping and sausage-like segmentation
IRMA (Intraretinal Microvascular Abnormalities):
- Arteriolar-venular shunts bypassing capillary bed
- Fine, irregular red intraretinal lines running from arterioles to venules
- FA: hypofluorescence (capillary dropout) — no leakage (unlike NV)
- OCT: IRMA do not breach the internal limiting membrane (ILM) — distinguishes from NV
4-2-1 Rule for Severe NPDR:
- Severe haemorrhages in 4 quadrants
- Venous beading in 2 quadrants
- IRMA in 1 quadrant
- (Any one = severe NPDR; two or more = very severe NPDR)
4. Proliferative DR (PDR)
Characterized by neovascularization — new vessel formation on inner retinal surface or optic disc.
NVD (New Vessels at Disc):
- On or within 1 disc diameter of optic disc
- Arise from disc or peripapillary vessels
- FA: early, profuse, irregular fluorescein leakage from disc
NVE (New Vessels Elsewhere):
- Beyond 1 disc diameter of disc
- Arise from venules, often adjacent to areas of capillary non-perfusion
High-Risk PDR — any one of:
- Presence of vitreous haemorrhage or preretinal haemorrhage
- Presence of any active neovascularization
- NV at or within 1 disc diameter of optic disc
- NVD > 1/3 disc area OR NVE > 1/2 disc area
5. Advanced Diabetic Eye Disease
- Vitreous haemorrhage: Preretinal (retrohyaloid) or intragel; can form "ochre membrane"
- Tractional retinal detachment: Contraction of fibrovascular membranes; incomplete PVD due to strong adhesions
- Rubeosis iridis (NVI): Iris neovascularization → angle closure → Neovascular glaucoma (NVG)
- Diabetic papillopathy: Disc oedema without significant haemorrhage or exudate; usually self-limiting
INVESTIGATIONS
| Investigation | Purpose |
|---|---|
| Fundus Photography | Documentation; screening |
| Fluorescein Angiography (FA) | Gold standard; detects leakage, NV, capillary non-perfusion, FAZ enlargement |
| OCT (Optical Coherence Tomography) | Quantifies macular oedema, SRF, epiretinal membrane, ILM breach |
| OCT-Angiography | Non-invasive assessment of retinal vasculature |
| B-scan Ultrasonography | Dense vitreous haemorrhage — rule out TRD |
| Electroretinography (ERG) | Assess retinal function in ischaemic disease |
| Systemic workup | HbA1c, blood pressure, lipid profile, renal function |
TREATMENT
A. Systemic Control (Medical Management)
- Glycaemic control: Target HbA1c < 7% (DCCT/UKPDS evidence); reduces onset and progression
- BP control: Target < 130/80 mmHg; ACE inhibitors preferred (Ramipril — EURODIAB study)
- Lipid control: Fenofibrate reduces hard exudate formation (FIELD study)
- Anaemia correction
B. Laser Photocoagulation
1. Focal/Grid Laser (for CSMO/Maculopathy):
- Focal laser: Treat specific leaking microaneurysms within 500–3000 µm of fovea
- Grid laser: For diffuse maculopathy; grid pattern over thickened retina
- Burns: 50–100 µm, 0.05–0.1 sec, 50–100 mW
- Traditional gold standard (now largely replaced by anti-VEGF)
2. Panretinal Photocoagulation (PRP) / Scatter Laser (for PDR):
- 1200–1800 burns applied beyond major vascular arcades
- Destroys ischaemic retina → reduces VEGF production → regression of NV
- Burns: 500 µm, 0.1–0.2 sec, white-grey burns
- Indications: High-risk PDR, any PDR with poor follow-up, severe NPDR progressing
- Pattern: Start inferior fundus first (haemorrhage gravitates inferiorly)
- Avoid areas of vitreoretinal traction
- Side effects: Peripheral field constriction, reduced night vision, macular oedema, choroidal detachment
Indicators of regression after PRP: Blunting of vessel tips, shrinking/disappearance of NV (leaving ghost vessels), regression of IRMA, decreased venous changes, disc pallor
3. Targeted Retinal Photocoagulation (TRP):
- Wide-field FA delineates peripheral non-perfusion
- Selective treatment of these areas — preserves more field than PRP
C. Anti-VEGF Therapy
| Drug | Mechanism |
|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF-A Fab fragment |
| Bevacizumab (Avastin) | Full anti-VEGF-A antibody (off-label) |
| Aflibercept (Eylea) | VEGF-A, VEGF-B, PlGF trap |
| Faricimab (Vabysmo) | Anti-VEGF-A + Ang-2 bispecific |
For Diabetic Macular Oedema:
- First-line treatment (superior to laser for CSMO)
- Protocol T (DRCR.net): Aflibercept superior to ranibizumab/bevacizumab at 1 year for worse VA; equivalent at 2 years
- Intravitreal injection every 4 weeks × 5 loading doses, then PRN/treat-and-extend
For PDR:
- DRCR.net Protocol S: Intravitreal ranibizumab as effective as PRP at 5 years for high-risk PDR
- Macular oedema rate reduced with anti-VEGF
- PRP preferred if follow-up is unreliable or cost is an issue
Pre-vitrectomy use: Anti-VEGF given 5–7 days before vitrectomy to reduce intraoperative bleeding
D. Intravitreal Steroids (for DME)
- Triamcinolone acetonide (off-label)
- Dexamethasone implant (Ozurdex) — 6-month biodegradable implant
- Fluocinolone acetonide implant (ILUVIEN) — 36-month sustained release
- Used in: Pseudophakic eyes, steroid-responder evaluation, non-responders to anti-VEGF
E. Vitreoretinal Surgery (Pars Plana Vitrectomy — PPV)
Indications:
- Dense, non-clearing vitreous haemorrhage (>3 months in Type 2; >1 month in Type 1)
- Tractional retinal detachment (TRD) involving/threatening macula
- Combined TRD + rhegmatogenous RD
- Macular traction with significant oedema
- Epiretinal membrane formation
Procedure: 23/25-gauge PPV; membranectomy; endolaser PRP; tamponade with gas or silicone oil if needed
SCREENING PROTOCOL (AK Khurana / National Guidelines)
| Diabetes Type | When to Screen | Frequency |
|---|---|---|
| Type 1 DM | 5 years after diagnosis (not before puberty) | Annually |
| Type 2 DM | At diagnosis | Annually; 6-monthly if DR present |
| Pregnancy (pre-existing DM) | At booking; 28 weeks | As indicated |
| Gestational DM | No specific DR screening needed | — |
Method: 7-field stereoscopic colour fundus photography (gold standard for screening); digital imaging ± slit-lamp biomicroscopy
DIABETIC PAPILLOPATHY
- Rare complication; disc oedema without significant disc pallor or haemorrhage
- Occurs in both Type 1 and Type 2 DM
- Usually unilateral; mild visual disturbance
- FA: disc hyperfluorescence
- Typically self-limiting over months; prognosis generally good
- Must be distinguished from AION and papilloedema
IMPORTANT CLINICAL TRIALS (RGUHS Exam High-Yield)
| Trial | Contribution |
|---|---|
| DCCT (1993) | Tight glycaemic control reduces DR risk in Type 1 DM |
| UKPDS (1998) | Tight control reduces DR in Type 2 DM |
| ETDRS | Focal laser for CSMO; aspirin does not worsen retinopathy |
| DRS (Diabetic Retinopathy Study) | PRP reduces severe visual loss by 50% in high-risk PDR |
| DRCR.net Protocol T | Aflibercept > ranibizumab/bevacizumab for severe DME at 1 year |
| DRCR.net Protocol S | Ranibizumab = PRP for PDR up to 5 years |
| FIELD study | Fenofibrate reduces laser treatments for DR |
| EURODIAB | ACE inhibitors reduce DR progression |
FUNDUS IMAGES
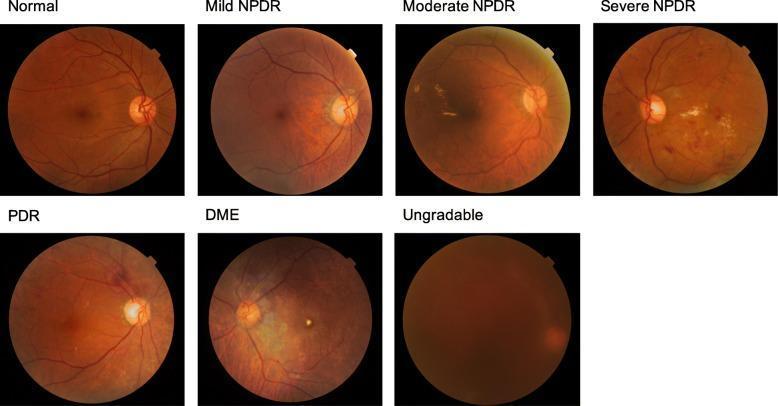
Classification of Diabetic Retinopathy stages: Normal → Mild NPDR → Moderate NPDR → Severe NPDR → Proliferative DR → Diabetic Macular Oedema
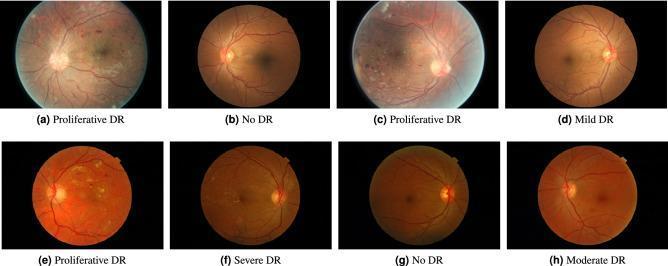
Five-level DR grading: No DR through Proliferative DR — showing microaneurysms, haemorrhages, NVD/NVE, exudates
QUICK REVISION — EXAM MNEMONICS
| Key Point | Mnemonic/Rule |
|---|---|
| Earliest histological change | Pericyte loss |
| Earliest clinical sign | Microaneurysms |
| Most important angiogenic factor | VEGF |
| Severe NPDR criteria | 4-2-1 Rule |
| High-risk PDR | Any one of: VH + NV present + NVD location + NVD > 1/3 DA |
| First-line for CSMO | Anti-VEGF (intravitreal ranibizumab/aflibercept) |
| PRP burns number | 1200–1800 burns |
| Screening starts (Type 1) | 5 years after diagnosis |
| Screening starts (Type 2) | At diagnosis |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. (ISBN 9780443110993); AK Khurana's Comprehensive Ophthalmology principles; ETDRS, DRS, DCCT, DRCR.net Protocol S & T trial data.
This is a shared conversation. Sign in to Orris to start your own chat.