Inguinal hernia 101
Reading File
Finding Sources
Searching the Web
inguinal hernia anatomy types management overview 2024
Reading File
Reading File
Reading File
Searching Images
inguinal hernia anatomy direct indirect canal
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material to write a thorough overview. Let me compile the answer.
Inguinal Hernia 101
Definition & Epidemiology
An inguinal hernia is a protrusion of abdominal contents through a defect in the inguinal region of the abdominal wall. They are the most common type of hernia, accounting for 75% of all hernias, with two-thirds of those being indirect type. There is a clear male predominance (~10:1 male:female for indirect hernias). They occur at all ages — from premature neonates to the elderly.
Anatomy of the Inguinal Canal
The inguinal canal is an oblique passage (~4 cm long) through the lower anterior abdominal wall, running from the deep (internal) inguinal ring to the superficial (external) inguinal ring in the external oblique aponeurosis.
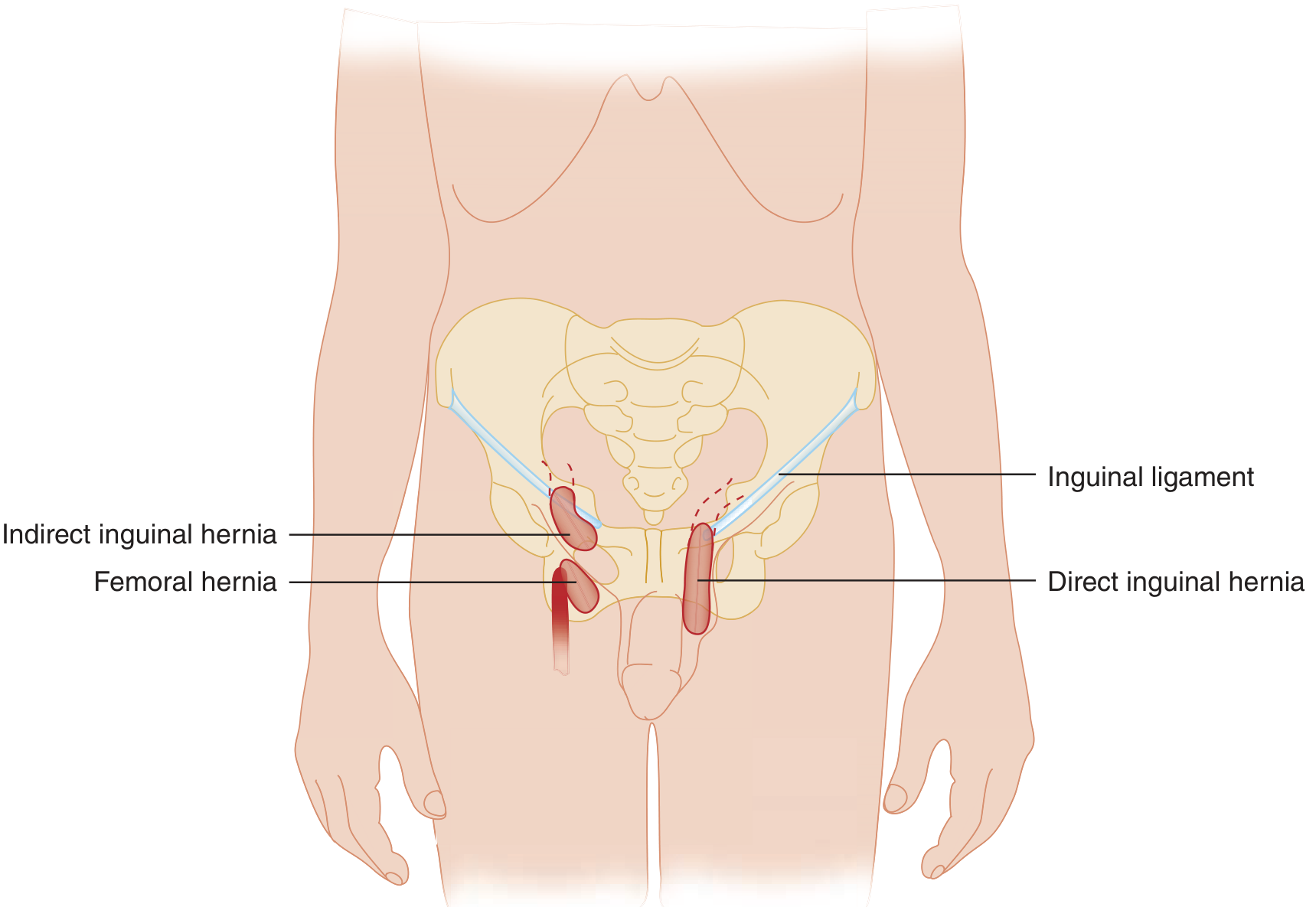
The inguinal triangle (Hesselbach's triangle) is the key landmark:
- Inferior: Inguinal ligament
- Superolateral: Inferior epigastric artery
- Medial: Lateral edge of the rectus abdominis
Contents of the inguinal canal in males: spermatic cord (vas deferens, testicular vessels, genital branch of the genitofemoral nerve, ilioinguinal nerve). In females: round ligament.
Types of Inguinal Hernia
Indirect Inguinal Hernia
- Passes through the deep inguinal ring, lateral to the inferior epigastric vessels, then travels along the inguinal canal, exits via the superficial ring, and can descend into the scrotum (or labium majus)
- Most common hernia overall (~66% of all inguinal hernias)
- In children: caused by a patent processus vaginalis (failure of closure before birth) — all pediatric hernias are by definition indirect
- In adults: also occurs due to the persistent processus vaginalis or acquired weakness
- Higher risk of incarceration due to narrow neck at the deep ring
Direct Inguinal Hernia
- Passes directly through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to the inferior epigastric vessels
- Does not travel down the inguinal canal
- Acquired weakness — caused by aging and repetitive stress from increased intra-abdominal pressure
- Typically has a wide neck → lower incarceration risk
- Common in older men
| Feature | Indirect | Direct |
|---|---|---|
| Location | Lateral to inferior epigastric vessels | Medial to inferior epigastric vessels |
| Mechanism | Patent processus vaginalis / deep ring | Acquired posterior wall weakness |
| Age group | Any (especially children, young adults) | Middle-aged/elderly |
| Neck | Narrow (higher incarceration risk) | Wide (lower incarceration risk) |
| Enters scrotum? | Yes (can) | Rarely |
Reducibility Classification
| State | Definition |
|---|---|
| Reducible | Contents can be returned to the abdomen manually |
| Incarcerated | Contents are not reducible without surgery; hernia sac swollen |
| Strangulated | Incarcerated + compromised blood supply → ischemia/necrosis → surgical emergency |
The natural history of strangulation: venous/lymphatic compression occurs first (thin walls), then arterial occlusion follows → intestinal obstruction, perforation, peritonitis.
Clinical Presentation
- Groin bulge — appears or enlarges with standing, coughing (Valsalva), or straining; reduces when lying flat
- Pain/discomfort — pressure, sharp, or referred pain to scrotum/testicle/inner thigh (from nerve compression)
- Sudden onset pain → concerning for incarceration or strangulation
- Children: parents notice bulge during diaper change; infants are at high risk for incarceration due to narrow ring
Examination
- Inspect standing patient — look for bulge in groin/scrotum
- Palpate — advance index finger through scrotum toward the external inguinal ring, ask patient to cough (Valsalva):
- Impulse at the tip of finger → indirect hernia
- Impulse on the dorsum of finger → direct hernia
- (Note: clinical accuracy is only slightly better than chance — ~50%)
- Inguinal occlusion test — block the deep ring with a finger; controlled impulse on cough = indirect (blocked), persistent bulge = direct
- Femoral hernias: palpable below the inguinal ligament, lateral to the pubic tubercle
Differential diagnosis of a groin mass: lymphadenopathy, hydrocele, varicocele, epididymitis, testicular torsion/tumor, femoral artery aneurysm, psoas abscess, undescended testis, sebaceous cyst, saphenous varix, cyst of the canal of Nuck (female).
Imaging
Imaging is not needed for obvious hernias. Use when the diagnosis is uncertain:
| Modality | Notes |
|---|---|
| Ultrasound | First-line, no radiation; sensitivity 86%, specificity 77%; operator-dependent; requires dynamic assessment (Valsalva) |
| CT | Best for obese patients, occult hernias, complications; excellent anatomical detail |
| MRI | Static detail; useful in athletes (sports hernia/athletic pubalgia) |
Management
Watchful Waiting
- An option for asymptomatic/minimally symptomatic reducible inguinal hernias in adults, though morbidity is higher with emergency vs elective repair
- Not appropriate in children — spontaneous resolution does not occur; repair is always indicated once diagnosed
Surgical Repair — Key Principles
Repair is herniorrhaphy (closing the defect) in children; hernioplasty (floor reconstruction ± mesh) in adults.
Open Anterior Approaches
| Technique | Features |
|---|---|
| Lichtenstein (tension-free mesh) | Standard of care; polypropylene mesh placed over the inguinal floor; mesh sutured to inguinal ligament, conjoint tendon; tails wrap the cord to recreate the deep ring. Low recurrence (~1%) |
| Bassini | Historic tissue repair; triple-layer (transversalis fascia + transversus abdominis + internal oblique) to inguinal ligament; higher recurrence |
| Shouldice | Multi-layer transversalis fascia repair; lower recurrence than Bassini; preferred tissue repair when mesh is contraindicated |
| McVay (Cooper's ligament repair) | Fixes transversalis fascia to Cooper's ligament; also addresses femoral hernias; requires relaxing incision |
Tissue repairs are used when mesh is contraindicated (contaminated field, emergency with uncertain bowel viability).
Posterior/Preperitoneal Approaches
- Rives-Stoppa: Large mesh in preperitoneal space via infraumbilical incision; good for bilateral/recurrent hernias
- Open preperitoneal: Transverse incision above deep ring; enters preperitoneal space directly
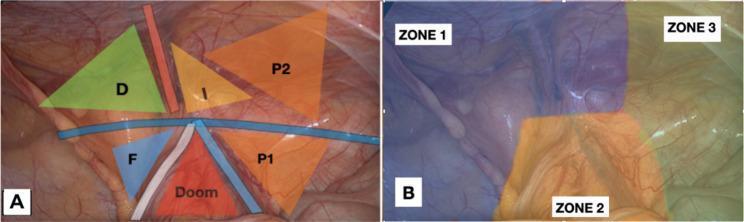
Laparoscopic Approaches
- TEP (Totally Extraperitoneal) and TAPP (Transabdominal Preperitoneal)
- Mesh placed in the preperitoneal space covering the direct, indirect, and femoral spaces
- Key landmarks: Triangle of Doom (contains external iliac vessels — no fixation here), Triangle of Pain (contains genitofemoral nerve and lateral cutaneous nerve of the thigh)
Special Populations
Pediatric
- All pediatric hernias are indirect (patent processus vaginalis)
- Higher incidence in premature infants (closure of processus normally occurs months before birth)
- Incarceration occurs in 30% of hernias in children < 3 months
- If incarcerated but reducible → repair within 24–48 hours
- If unreducible or strangulated → emergency surgery
- In females: check for ovary in sac; rule out testicular feminization (androgen insensitivity)
Adults
- Females: rare inguinal hernias need to be distinguished from femoral hernias (higher strangulation risk)
- Obesity makes examination difficult and increases false-negative/false-positive rates
- Recurrent hernias: prefer preperitoneal mesh approach (Rives-Stoppa or laparoscopic) to avoid scarred anterior field
Complications of Repair
- Chronic groin pain (most common long-term complaint) — from nerve entrapment (ilioinguinal, iliohypogastric, genital branch of genitofemoral)
- Recurrence — lower with mesh (~1%) vs. tissue repair (~10–15%)
- Wound infection / mesh infection
- Injury to vas deferens or testicular vessels → infertility or testicular atrophy
- Hematoma / seroma
Sources: Schwartz's Principles of Surgery 11e, Sabiston Textbook of Surgery, Tintinalli's Emergency Medicine, Roberts and Hedges' Clinical Procedures in Emergency Medicine, Gray's Anatomy for Students, Campbell-Walsh-Wein Urology
I'm in surgery, inguinal hernia 101 include paeds
Finding Sources
Searching the Web
pediatric inguinal hernia surgery repair technique 2024 guidelines
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
pediatric inguinal hernia repair high ligation processus vaginalis surgical technique
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Intestinal obstruction 101
Reading File
Finding Sources
Searching the Web
intestinal obstruction small bowel large bowel management surgery 2024
Reading File
Reading File
Finding Sources
Searching Images
intestinal obstruction abdominal X-ray dilated bowel loops air fluid levels
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
sigmoid volvulus abdominal X-ray coffee bean sign CT scan
Reading File
Loading Image
Reading File
Loading Image
Excellent material gathered. Now compiling the comprehensive guide.
Intestinal Obstruction 101
Definition & Classification
Intestinal obstruction = failure of intestinal contents to pass aborally due to a physical barrier (mechanical) or failure of propulsion (functional/ileus).
Primary Classification
| Type | Mechanism | Examples |
|---|---|---|
| Mechanical | Physical block | Adhesions, hernia, tumour, volvulus |
| Functional (Ileus / Pseudo-obstruction) | Motility failure without a lesion | Post-op ileus, electrolyte disturbance, sepsis |
By Anatomical Location
| Small Bowel Obstruction (SBO) | Large Bowel Obstruction (LBO) | |
|---|---|---|
| Most common cause | Adhesions (~75%) | Colorectal carcinoma (80–90%) |
| Next most common | Hernias, Crohn's, malignancy | Diverticulitis, volvulus |
| Pain character | Colicky, central | Colicky, lower/lateral |
| Vomiting | Early, prominent | Late or absent |
| Distension | Moderate (central) | Marked (peripheral) |
| Obstipation | Present in complete | Usually present |
Causes — A Surgical Framework
The obstructing lesion sits in one of three anatomical relationships to the bowel wall:
1. Intraluminal — Foreign body, gallstone ileus, meconium, bezoar, parasites
2. Intramural — Crohn's stricture, carcinoma, radiation stricture, haematoma, Meckel's diverticulum
3. Extrinsic (most common) — Adhesions, hernias (external & internal), carcinomatosis, volvulus
Common SBO Causes (in order of frequency)
- Adhesions (post-op) — #1, up to 75%
- Incarcerated hernia — #2
- Malignancy (carcinomatosis, direct invasion)
- Crohn's disease
- Volvulus / intussusception
- Gallstone ileus, radiation stricture, Meckel's
Common LBO Causes
- Colorectal carcinoma — #1
- Diverticulitis
- Volvulus (sigmoid > caecal)
- Metastatic disease
- Hernia (rare)
Pathophysiology
With onset of obstruction, gas and fluid accumulate proximal to the obstruction:
- Most gas = swallowed air + some intraluminal production
- Fluid = swallowed liquids + GI secretions (obstruction stimulates epithelial secretion)
- Bowel initially hyperactive → trying to overcome obstruction (accounts for colicky pain and paradoxical diarrhoea early on)
- Rising intraluminal pressure → impaired microvascular perfusion → ischaemia → necrosis (strangulation)
- Bacterial overgrowth and translocation occur; flora change from near-sterile to polymicrobial
Closed-Loop Obstruction
Bowel obstructed both proximally and distally (e.g., volvulus, herniated loop). Gas and fluid cannot decompress in either direction → rapid pressure rise → rapid progression to strangulation. High risk of perforation.
Partial vs. Complete
- Partial: some gas/fluid still passes; slower progression; strangulation less likely
- Complete: no passage; high risk of strangulation; requires more urgent intervention
Clinical Presentation
Classic tetrad:
- Colicky abdominal pain — central (SBO) or lower (LBO)
- Vomiting — early and frequent in proximal SBO; late/faeculent in distal SBO; late/absent in LBO
- Distension — absent in proximal SBO; massive in distal/LBO
- Absolute constipation / obstipation — complete obstruction; note that early on, some stool/flatus may still pass
Bowel Sounds
- Early mechanical obstruction: high-pitched, tinkling, frequent rushes
- Late / strangulation / ileus: diminished or absent
Signs of Strangulation (urgent surgical flag)
- Pain disproportionate to examination findings
- Tachycardia, fever
- Localised peritonism / guarding / rigidity
- Marked leukocytosis (>15–20 × 10⁹/L)
- Metabolic acidosis
- Irreducible tender mass (hernia context)
Diagnosis
Goals of diagnostic evaluation:
- Distinguish mechanical obstruction from ileus
- Determine SBO vs. LBO
- Discriminate partial from complete
- Detect strangulation or closed loop
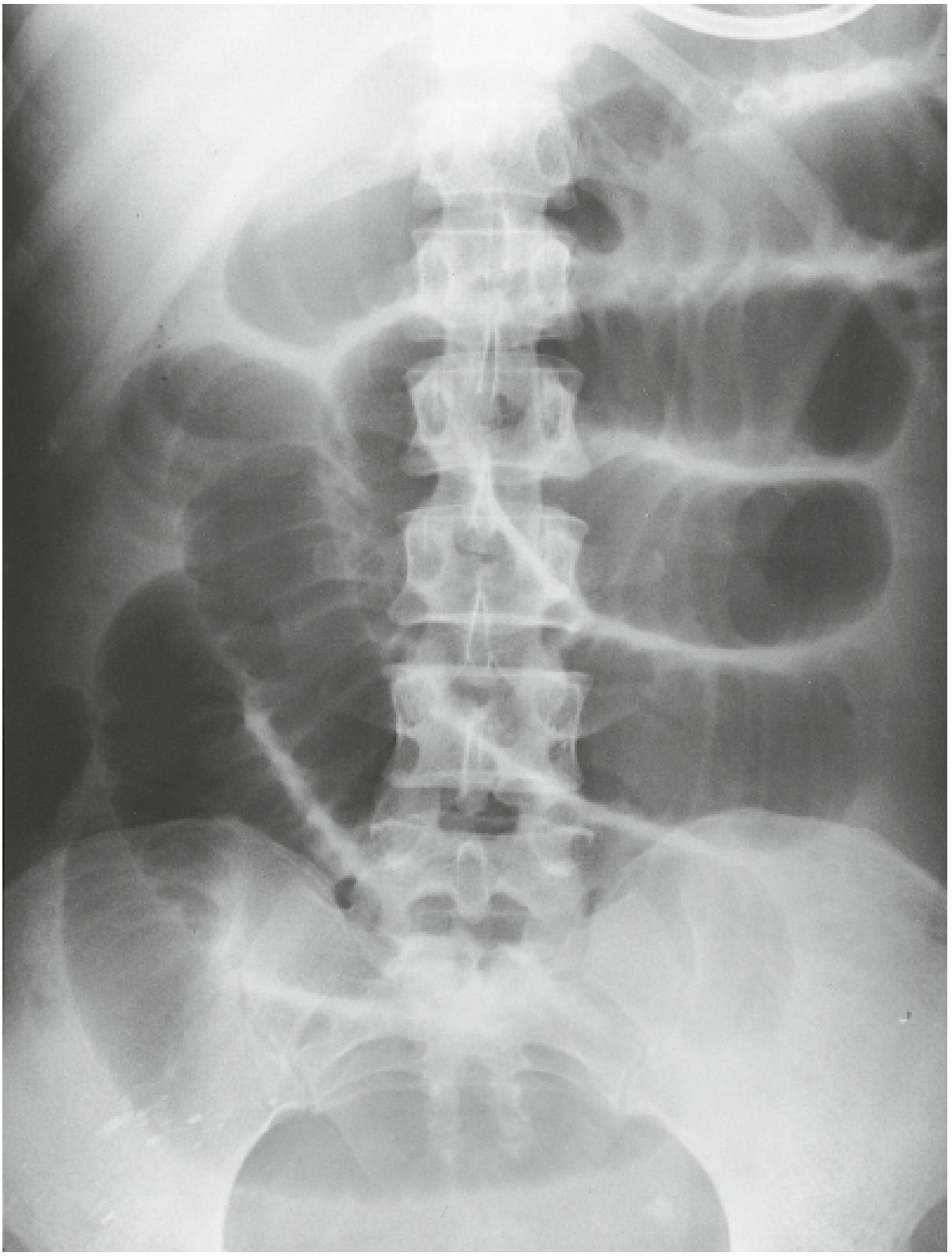
Plain Abdominal Radiograph (AXR)
Performed as erect + supine ± CXR (to exclude free air)
| Feature | Small Bowel | Large Bowel |
|---|---|---|
| Loop location | Central | Peripheral (frame-like) |
| Fold markings | Valvulae conniventes — complete, closely spaced, traverse full width | Haustra — incomplete, widely spaced |
| Diameter | >3 cm = dilated | >6 cm = dilated; >9 cm caecum = critical |
| Classic finding | "Stepladder" air-fluid levels | Peripheral colonic distension ± competent/incompetent ileocaecal valve |
| Paucity of distal gas | Colon empty | Rectum/sigmoid empty |
Sensitivity of AXR for SBO: 70–80%. Specificity low (ileus and LBO can mimic).
"String of pearls" sign — tiny gas bubbles along superior margin of fluid-filled SBO loops (seen on upright/decubitus).
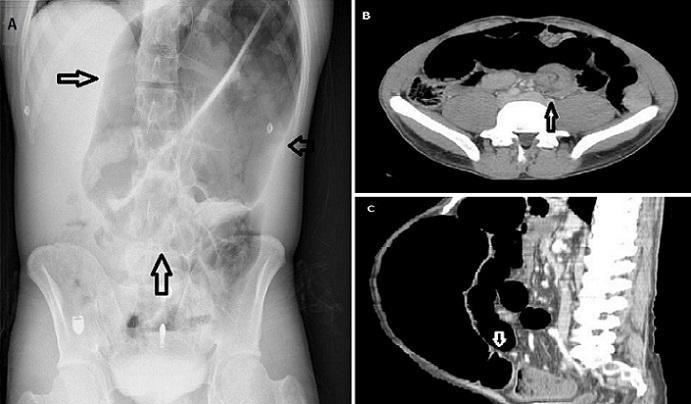
CT Abdomen/Pelvis (with oral contrast)
First-line definitive imaging — 80–90% sensitive, 70–90% specific for SBO.
CT findings of obstruction:
- Discrete transition zone — dilated proximal, collapsed distal
- Intraluminal contrast does not pass the transition point
- Colon contains little gas or fluid
CT signs of closed-loop obstruction:
- C-shaped or U-shaped dilated loop
- Radial distribution of mesenteric vessels converging toward a torsion point (whirl sign)
CT signs of strangulation:
- Bowel wall thickening
- Pneumatosis intestinalis (air in bowel wall)
- Portal venous gas
- Mesenteric haziness/"fat stranding"
- Poor IV contrast enhancement of bowel wall
Water-Soluble Contrast (Gastrografin / Omnipaque)
Used both diagnostically and therapeutically in adhesive SBO:
- Appearance of contrast in the colon within 24 hours predicts non-operative resolution with sensitivity 92%, specificity 93%
- Has osmotic effect that may reduce oedema and promote resolution
- Preferred over barium if perforation suspected
Specific Types
Sigmoid Volvulus
- Most common site of colonic volvulus
- Predisposed: elderly, chronic constipation, redundant sigmoid on long mesentery, institutionalised patients
- AXR: "coffee bean" sign — massively distended sigmoid loop rising from the pelvis, midline crease
- CT: "whirl sign" (mesenteric torsion) + "bird's beak" sign (tapering at point of twist)
- Management: Flexible sigmoidoscopy/rigid proctoscopy for detorsion (first line if no peritonitis) → tube decompression → elective sigmoid resection after bowel prep; emergency Hartmann's if perforated/gangrenous
Caecal Volvulus
- Younger patients; axial twisting of mobile caecum
- AXR: distended oval structure in left upper quadrant ("coffee bean" pointing to LUQ)
- Management: right hemicolectomy (detorsion alone has high recurrence; caecostomy if too unstable)
- Caecal dilation >12–14 cm = surgical emergency (high perforation risk)
Gallstone Ileus
- Rare; large gallstone erodes through cholecystoduodenal fistula into small bowel
- Rigler's triad: SBO + pneumobilia + ectopic gallstone (usually at terminal ileum)
- Treatment: enterotomy and stone extraction ± cholecystectomy/fistula repair (staged)
Ileus vs. Mechanical Obstruction
| Feature | Mechanical Obstruction | Ileus |
|---|---|---|
| Cause | Physical block | Motility failure (surgery, sepsis, electrolytes, drugs) |
| Pain | Colicky, severe | Diffuse, dull or absent |
| Bowel sounds | High-pitched rushes → silent | Diminished/absent |
| AXR | Transition zone; stepladder | Diffuse gaseous distension; gas throughout incl. rectum |
| CT | Transition point present | No transition; gas throughout all segments |
| Management | Intervention usually required | Treat underlying cause; conservative |
Ileus Causes (common)
- Post-operative (normal ≤5 days after laparotomy)
- Small bowel recovers: 24 hours; Stomach: 48 hours; Colon: 2–5 days
- Bowel sounds returning is NOT a reliable indicator — flatus/stool is
- Sepsis, peritonitis, intra-abdominal abscess
- Electrolyte disturbance: hypokalaemia (most common), hypomagnesaemia, hyponatraemia
- Drugs: opiates, anticholinergics, phenothiazines, tricyclics, calcium channel blockers
- Retroperitoneal haematoma, spinal cord injury, MI, mesenteric ischaemia
Reducing Post-op Ileus
- Minimise bowel handling
- Laparoscopic approach
- Restrict intraoperative fluids
- Avoid NG tubes (if not essential)
- NSAIDs (ketorolac) + reduce opioids
- Thoracic epidural analgesia
- Chewing gum / early mobilisation / early feeding (ERAS protocols)
Management
Initial Resuscitation (All Obstruction)
- NBM
- IV access — fluid resuscitation (often dehydrated from vomiting + third-spacing)
- Correct electrolytes (especially K⁺)
- NG tube if vomiting/distension (decompression)
- Urinary catheter (fluid balance)
- Serial examinations — watch for strangulation features
- Bloods: FBC, U&E, LFTs, amylase, lactate, group & save, clotting
SBO — Non-operative Management (drip and suck)
Appropriate for partial/incomplete SBO without strangulation, especially adhesive:
- IV fluids, NGT, NBM
- Close monitoring (6-hourly obs, serial abdominal exams)
- Gastrografin challenge — therapeutic + prognostic
- Most adhesive SBOs (70–80%) resolve with conservative management
- Trial up to 48–72 hours for partial; less tolerance for complete
Indications for Emergency Surgery
- Signs of strangulation (peritonism, fever, tachycardia, rising lactate)
- Complete obstruction that fails conservative management
- Closed-loop obstruction
- Incarcerated/strangulated hernia (irreducible)
- Free perforation (pneumoperitoneum)
- Caecal diameter >12 cm (LBO)
- Volvulus with gangrenous bowel
Operative Options
| Scenario | Procedure |
|---|---|
| Adhesive SBO | Laparoscopy/laparotomy + lysis of adhesions |
| Non-viable bowel | Resection ± primary anastomosis ± stoma |
| LBO — resectable carcinoma | Hartmann's (most common emergency) or resection + primary anastomosis if bowel prepped |
| LBO — palliation | Self-expanding metal stent (SEMS) — bridge to surgery or definitive palliation |
| Sigmoid volvulus with gangrene | Hartmann's procedure |
| Caecal volvulus | Right hemicolectomy |
| Gallstone ileus | Enterotomy + stone extraction |
Adhesion Prevention
- Good surgical technique, minimise peritoneal exposure to foreign material
- Laparoscopic surgery (4× lower risk of SBO vs. open at 5 years)
- Hyaluronan-based membrane (Seprafilm) reduces adhesion formation; effect on SBO incidence less clear; avoid wrapping anastomoses (increased leak rate)
Prognosis / Complications
- Strangulated obstruction carries significant mortality (~10–20% in delayed cases)
- Malignant bowel obstruction: median survival 3–4 months
- ~25–30% of patients with cancer and bowel obstruction have a benign cause (adhesions) — don't assume malignancy
- Post-op SBO recurrence risk after adhesiolysis remains significant; 30%+ hospital readmission rate within 10 years after colorectal/pelvic surgery
Sources: Schwartz's Principles of Surgery 11e, Mulholland and Greenfield's Surgery 7e, Yamada's Textbook of Gastroenterology 7e, Harrison's Principles of Internal Medicine 22e, Sleisenger & Fordtran's GI & Liver Disease, Tintinalli's Emergency Medicine
Urolithiasis, Prostate & Urinary Tract Infections
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
kidney stone CT scan renal calculus ureter
Reading File
Reading File
Loading Image
Reading File
Reading File
Searching Images
benign prostatic hyperplasia BPH TURP prostate anatomy bladder obstruction
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.