Make a poster on mucosal fold middle ear
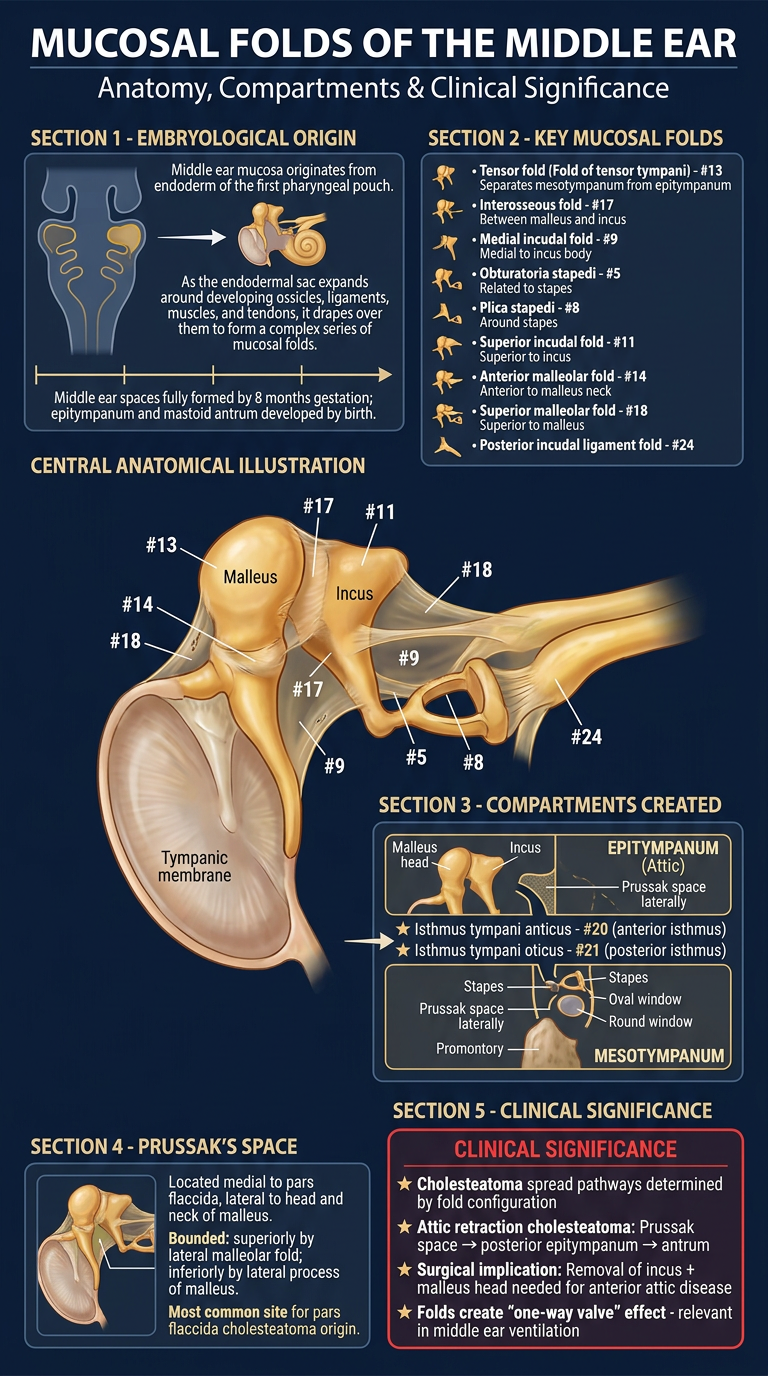
Medical education poster titled "Mucosal Folds of the Middle Ear" for ENT/otolaryngology students. The poster should include: TITLE at top: "Mucosal Folds of the Middle Ear" with subtitle "Anatomy, Compartments & Clinical Significance" SECTION 1 - EMBRYOLOGICAL ORIGIN: - Middle ear mucosa originates from endoderm of the first pharyngeal pouch - As the endodermal sac expands around developing ossicles, ligaments, muscles, and tendons, it drapes over them to form a complex series of mucosal folds - Middle ear spaces fully formed by 8 months gestation; epitympanum and mastoid antrum developed by birth SECTION 2 - KEY MUCOSAL FOLDS (list with icons): • Tensor fold (Fold of tensor tympani) - #13: Separates mesotympanum from epitympanum • Interosseous fold - #17: Between malleus and incus • Medial incudal fold - #9: Medial to incus body • Obturatoria stapedi - #5: Related to stapes • Plica stapedi - #8: Around stapes • Superior incudal fold - #11: Superior to incus • Anterior malleolar fold - #14: Anterior to malleus neck • Superior malleolar fold - #18: Superior to malleus • Posterior incudal ligament fold - #24 SECTION 3 - COMPARTMENTS CREATED: Box diagram showing: - EPITYMPANUM (Attic): Contains malleus head, incus body; subdivided into Prussak space laterally - MESOTYMPANUM: Medial to TM; contains stapes, oval window, round window, promontory - Only two openings remain after partitioning: ★ Isthmus tympani anticus - #20 (anterior isthmus) ★ Isthmus tympani oticus - #21 (posterior isthmus) SECTION 4 - PRUSSAK'S SPACE: - Located medial to pars flaccida, lateral to head and neck of malleus - Bounded: superiorly by lateral malleolar fold; inferiorly by lateral process of malleus - Most common site for pars flaccida cholesteatoma origin SECTION 5 - CLINICAL SIGNIFICANCE (red-highlighted box): ★ Cholesteatoma spread pathways determined by fold configuration ★ Attic retraction cholesteatoma: Prussak space → posterior epitympanum → antrum ★ Surgical implication: Removal of incus + malleus head needed for anterior attic disease ★ Folds create "one-way valve" effect - relevant in middle ear ventilation COLOR SCHEME: Deep navy blue background, gold/amber anatomical highlights, white text, red accent for clinical pearls. Professional medical poster style with clean sections and anatomical illustration placeholder in center showing ossicles with numbered fold labels.
What the Poster Covers
- Middle ear mucosa derives from endoderm of the first pharyngeal pouch. As it expands around the ossicles, ligaments, muscles, and tendons, it drapes over them, creating a complex series of mucosal folds. The middle ear spaces are fully formed by 8 months' gestation.
- Tensor fold (#13) - the most important; separates mesotympanum from epitympanum
- Interosseous fold (#17) - between malleus and incus
- Medial incudal fold (#9) - medial to incus body
- Plica stapedi (#8) and Obturatoria stapedi (#5) - around stapes
- Superior/anterior malleolar folds (#18, #14) - around malleus
- Superior incudal fold (#11) and Posterior incudal ligament fold (#24)
- Together, these folds partition the middle ear, leaving only two critical openings: the Isthmus tympani anticus (#20) and Isthmus tympani oticus (#21) - the sole communication channels between mesotympanum and epitympanum
- The key epitympanic sub-compartment lateral to the malleus neck, medial to pars flaccida - the most common origin site for acquired cholesteatoma
- Fold anatomy dictates the spread pathways of cholesteatoma
- Relevant to middle ear aeration and surgical planning
Change the poster design and make light colour poster
Medical education poster titled "Mucosal Folds of the Middle Ear" for ENT/otolaryngology students. Light, clean, modern design with white and soft pastel background. TITLE at top: "Mucosal Folds of the Middle Ear" in dark teal bold font, subtitle "Anatomy, Compartments & Clinical Significance" in gray SECTION 1 - EMBRYOLOGICAL ORIGIN (light blue card): - Middle ear mucosa originates from endoderm of the first pharyngeal pouch - Endodermal sac drapes over ossicles, ligaments, muscles and tendons → complex series of mucosal folds - Middle ear spaces fully formed by 8 months gestation SECTION 2 - KEY MUCOSAL FOLDS (light green card, two columns): • Tensor fold (#13) — separates mesotympanum from epitympanum • Interosseous fold (#17) — between malleus and incus • Medial incudal fold (#9) — medial to incus body • Plica stapedi (#8) — around stapes • Obturatoria stapedi (#5) — stapes region • Superior incudal fold (#11) — superior to incus • Anterior malleolar fold (#14) — anterior malleus neck • Superior malleolar fold (#18) — superior malleus • Posterior incudal ligament fold (#24) SECTION 3 - COMPARTMENTS CREATED (light yellow card): Neat diagram/table showing: EPITYMPANUM (Attic): malleus head, incus body, Prussak space laterally MESOTYMPANUM: stapes, oval window, round window, promontory, sinus tympani Two critical openings only: ★ Isthmus tympani anticus (#20) — anterior ★ Isthmus tympani oticus (#21) — posterior SECTION 4 - PRUSSAK'S SPACE (light lavender card): - Medial to pars flaccida, lateral to malleus head/neck - Superiorly: lateral malleolar fold; Inferiorly: lateral process of malleus - Primary site of pars flaccida cholesteatoma SECTION 5 - CLINICAL PEARLS (soft coral/peach card with bold red text for pearls): ★ Folds dictate cholesteatoma spread pathway ★ Attic cholesteatoma: Prussak space → posterior epitympanum → antrum → mastoid ★ Surgery: incus + malleus head removal needed for anterior attic disease ★ Isthmus blockage impairs middle ear aeration COLOR SCHEME: White background, soft pastel section cards (light blue, light green, light yellow, lavender, peach), dark teal headings, charcoal body text, coral red for clinical pearls. Minimalist clean medical infographic style. Central anatomical illustration of middle ear ossicles with colored arrows indicating folds.
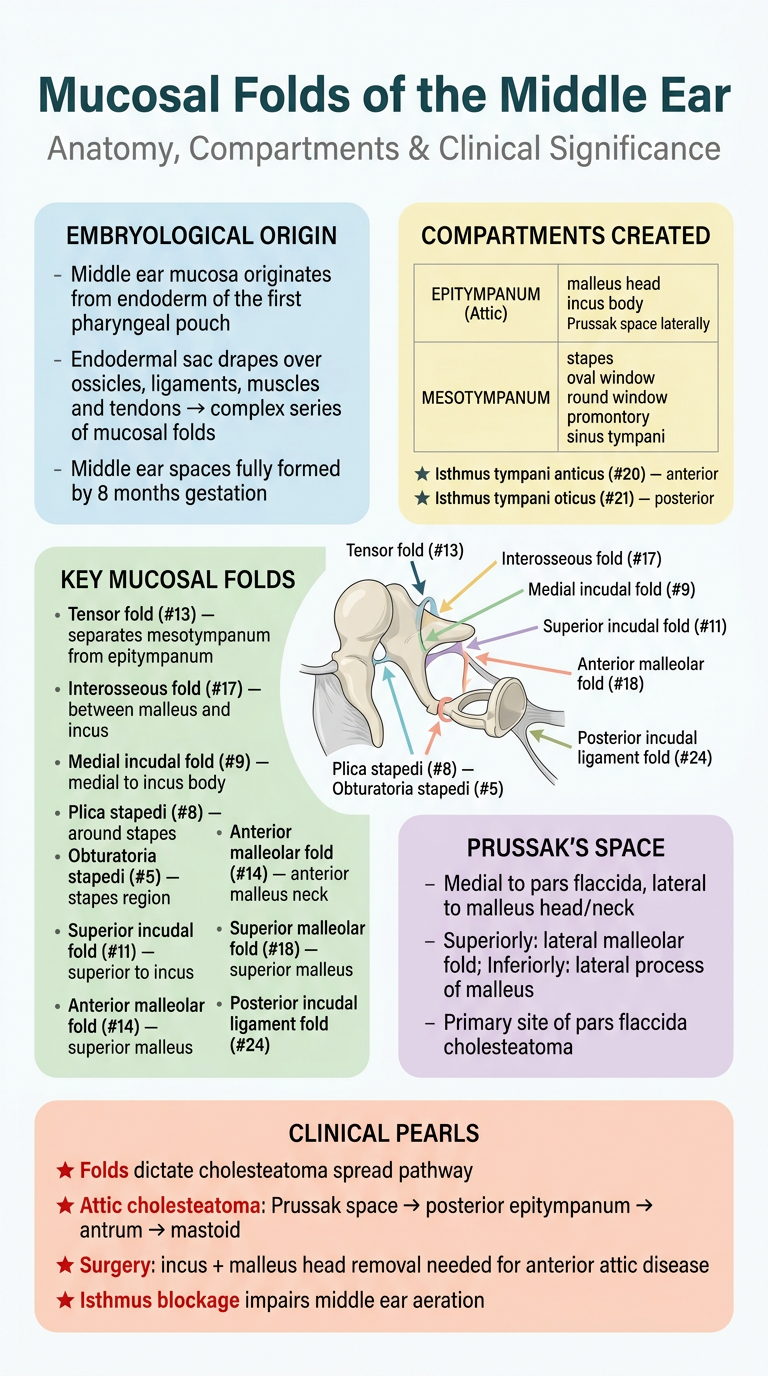
- White background with soft pastel section cards
- Dark teal headings for easy readability
- Color-coded sections - blue for embryology, green for fold names, yellow for compartments, lavender for Prussak's space, and peach for clinical pearls
- Minimalist modern style - much easier on the eyes compared to the dark version
Make light colour poster on petrous bone anatomy
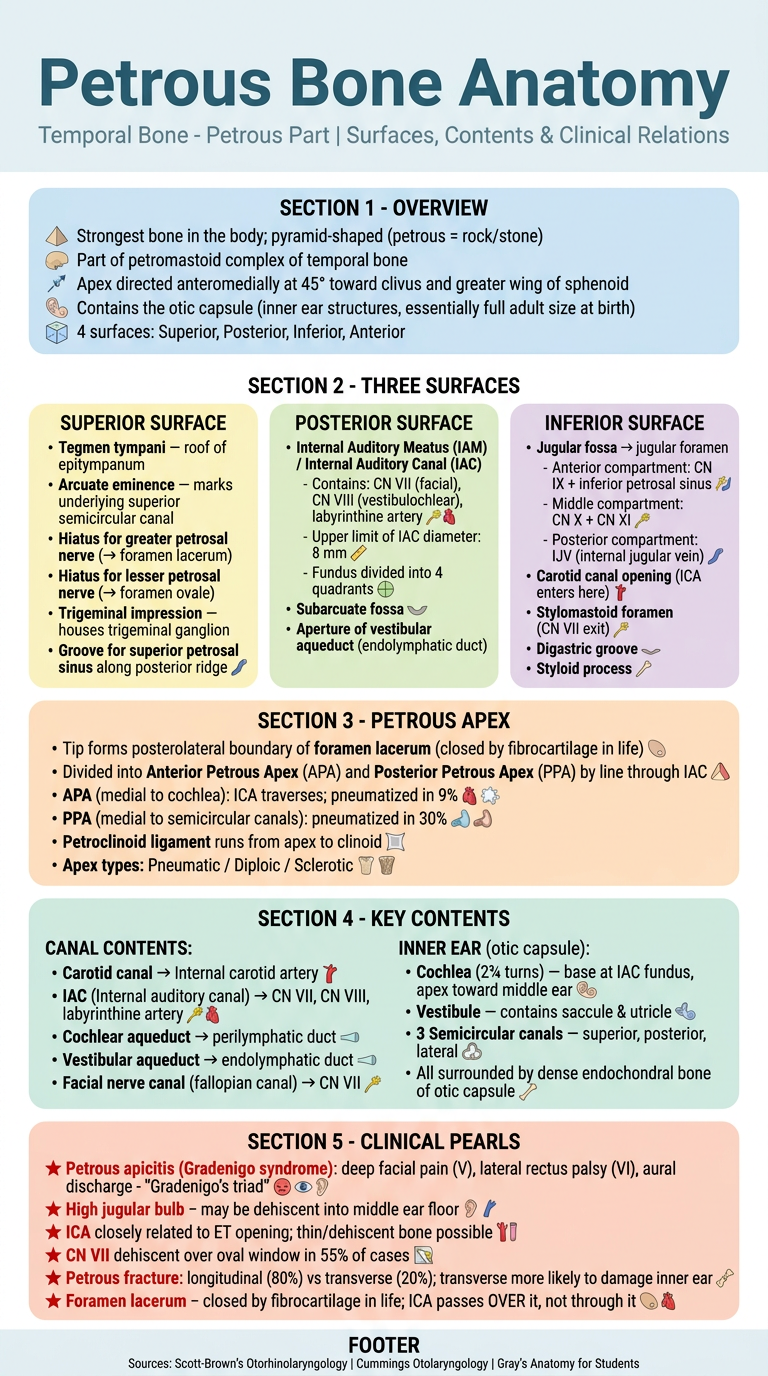
Light colour medical education poster titled "Petrous Bone Anatomy" for ENT/otolaryngology and anatomy students. Clean, bright, professional infographic style with white background and pastel colour sections. HEADER: Large bold title "Petrous Bone Anatomy" in dark teal. Subtitle: "Temporal Bone - Petrous Part | Surfaces, Contents & Clinical Relations" in slate gray. SECTION 1 - OVERVIEW (soft sky blue card): - Strongest bone in the body; pyramid-shaped (petrous = rock/stone) - Part of petromastoid complex of temporal bone - Apex directed anteromedially at 45° toward clivus and greater wing of sphenoid - Contains the otic capsule (inner ear structures, essentially full adult size at birth) - 4 surfaces: Superior, Posterior, Inferior, Anterior SECTION 2 - THREE SURFACES (three adjacent light pastel cards, horizontal row): [SUPERIOR SURFACE - light yellow card]: • Tegmen tympani — roof of epitympanum • Arcuate eminence — marks underlying superior semicircular canal • Hiatus for greater petrosal nerve (→ foramen lacerum) • Hiatus for lesser petrosal nerve (→ foramen ovale) • Trigeminal impression — houses trigeminal ganglion • Groove for superior petrosal sinus along posterior ridge [POSTERIOR SURFACE - light green card]: • Internal Auditory Meatus (IAM) / Internal Auditory Canal (IAC) - Contains: CN VII (facial), CN VIII (vestibulochlear), labyrinthine artery - Upper limit of IAC diameter: 8 mm - Fundus divided into 4 quadrants • Subarcuate fossa • Aperture of vestibular aqueduct (endolymphatic duct) [INFERIOR SURFACE - light lavender card]: • Jugular fossa → jugular foramen - Anterior compartment: CN IX + inferior petrosal sinus - Middle compartment: CN X + CN XI - Posterior compartment: IJV (internal jugular vein) • Carotid canal opening (ICA enters here) • Stylomastoid foramen (CN VII exit) • Digastric groove • Styloid process SECTION 3 - PETROUS APEX (light orange/peach card): • Tip forms posterolateral boundary of foramen lacerum (closed by fibrocartilage in life) • Divided into Anterior Petrous Apex (APA) and Posterior Petrous Apex (PPA) by line through IAC • APA (medial to cochlea): ICA traverses; pneumatized in 9% • PPA (medial to semicircular canals): pneumatized in 30% • Petroclinoid ligament runs from apex to clinoid • Apex types: Pneumatic / Diploic / Sclerotic SECTION 4 - KEY CONTENTS (two-column light mint card): Left column - CANAL CONTENTS: • Carotid canal → Internal carotid artery • IAC (Internal auditory canal) → CN VII, CN VIII, labyrinthine artery • Cochlear aqueduct → perilymphatic duct • Vestibular aqueduct → endolymphatic duct • Facial nerve canal (fallopian canal) → CN VII Right column - INNER EAR (otic capsule): • Cochlea (2¾ turns) — base at IAC fundus, apex toward middle ear • Vestibule — contains saccule & utricle • 3 Semicircular canals — superior, posterior, lateral • All surrounded by dense endochondral bone of otic capsule SECTION 5 - CLINICAL PEARLS (soft coral card, bold red highlights): ★ Petrous apicitis (Gradenigo syndrome): deep facial pain (V), lateral rectus palsy (VI), aural discharge - "Gradenigo's triad" ★ High jugular bulb - may be dehiscent into middle ear floor ★ ICA closely related to ET opening; thin/dehiscent bone possible ★ CN VII dehiscent over oval window in 55% of cases ★ Petrous fracture: longitudinal (80%) vs transverse (20%); transverse more likely to damage inner ear ★ Foramen lacerum - closed by fibrocartilage in life; ICA passes OVER it, not through it FOOTER: Small text "Sources: Scott-Brown's Otorhinolaryngology | Cummings Otolaryngology | Gray's Anatomy for Students" DESIGN: White background, soft pastel section cards (sky blue, yellow, green, lavender, peach, mint, coral), dark teal headings, charcoal body text. Clean grid layout, rounded corners on cards, small anatomical icons. Modern medical infographic style. No dark or black backgrounds.
Poster Contents
- Pyramid-shaped, the strongest bone in the body; "petrous" means rock/stone
- Part of the petromastoid complex of the temporal bone, apex directed anteromedially at 45°
- Superior surface (middle cranial fossa floor): tegmen tympani, arcuate eminence (superior SCC), grooves for greater/lesser petrosal nerves, trigeminal impression
- Posterior surface (posterior fossa): IAC (CN VII + VIII + labyrinthine artery), vestibular aqueduct aperture, subarcuate fossa
- Inferior surface: jugular fossa/foramen (CN IX, X, XI, IJV), carotid canal, stylomastoid foramen
- Divided into anterior (medial to cochlea) and posterior (medial to SCCs) by a line through the IAC
- Three types: pneumatic, diploic, or sclerotic
- Carotid canal, IAC, cochlear and vestibular aqueducts, fallopian canal (CN VII), full otic capsule with cochlea, vestibule, and semicircular canals
- Gradenigo's triad (petrous apicitis), high jugular bulb, foramen lacerum (ICA passes over - not through), CN VII dehiscence over oval window, petrous fracture patterns