Coronary circulation source only from guyton and ganong
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the necessary content from both textbooks. Let me compile a thorough, well-organized response.
Coronary Circulation
Sources: Guyton & Hall (14th Ed.) + Ganong's Review of Medical Physiology (26th Ed.)
1. Physiological Anatomy of Coronary Blood Supply
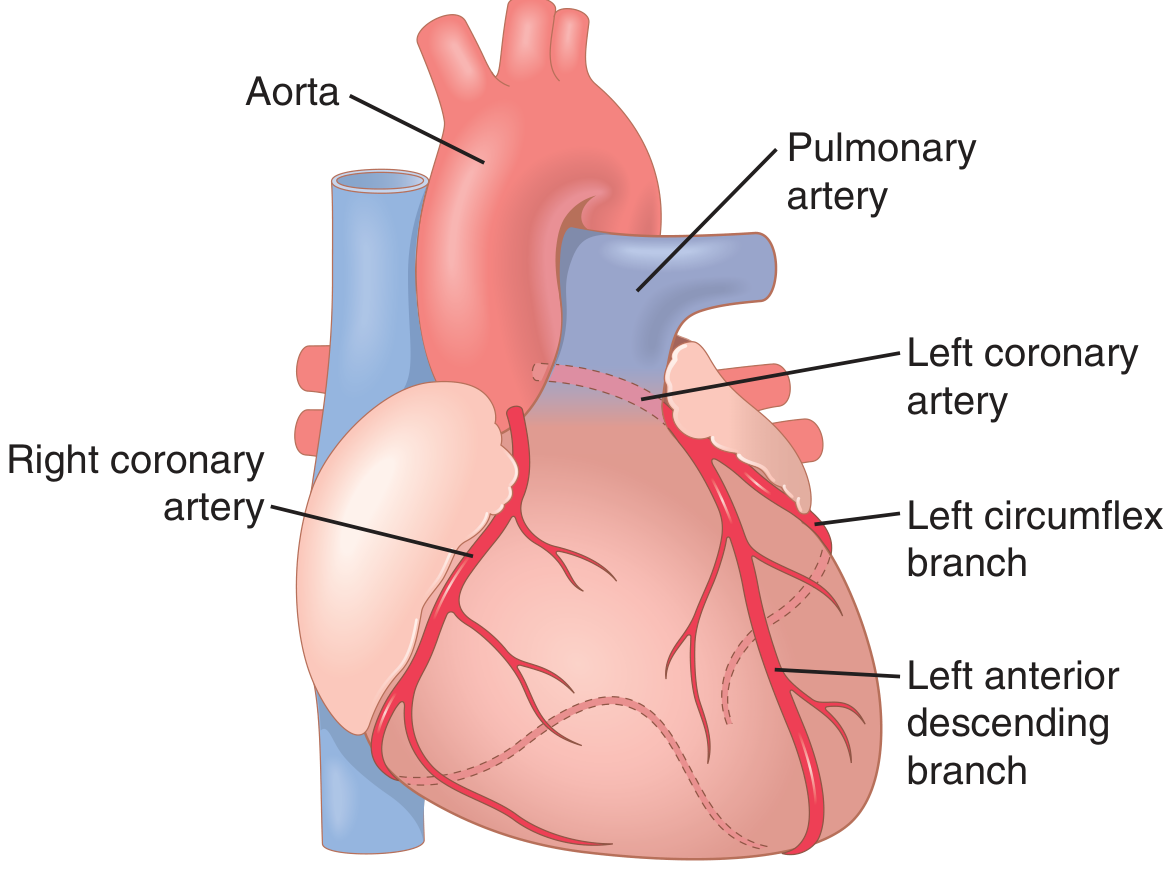
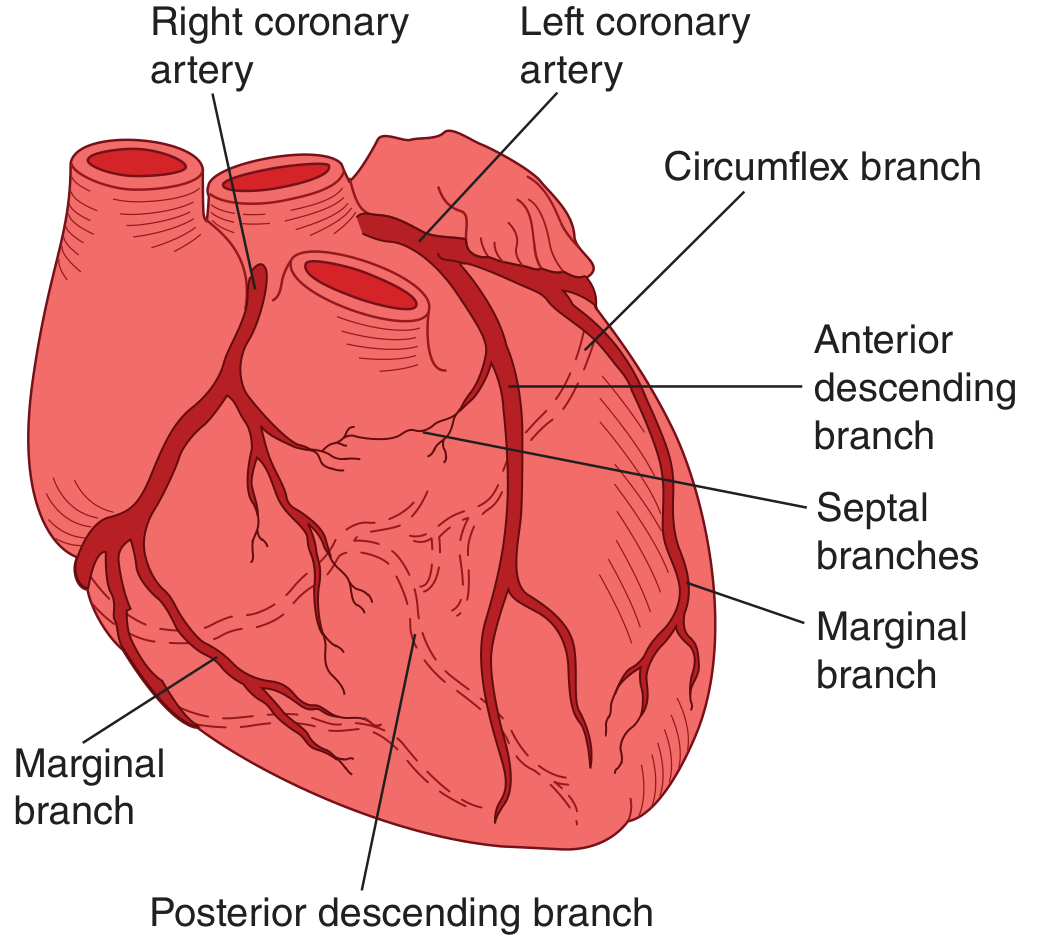
Arterial Supply
The two coronary arteries arise from sinuses behind two cusps of the aortic valve at the root of the aorta. The main coronary arteries lie on the surface of the heart, and smaller penetrating arteries go into the cardiac muscle mass. Only the inner 0.1 mm of the endocardial surface receives nutrition directly from blood in the cardiac chambers - this contribution is miniscule.
Left coronary artery supplies mainly:
- Anterior and left lateral portions of the left ventricle
- Branches: Left anterior descending (LAD), Circumflex, Septal branches
Right coronary artery supplies:
- Most of the right ventricle
- Posterior part of the left ventricle in 80-90% of people
- Posterior descending branch, marginal branches
(Guyton & Hall, Fig. 21.3)
(Ganong, Fig. 33-11)
Venous Drainage
| Route | Origin | Drains Into |
|---|---|---|
| Coronary sinus | ~75% of left ventricular venous blood | Right atrium |
| Anterior cardiac veins | Right ventricular muscle | Right atrium (directly, not via coronary sinus) |
| Thebesian veins | Small amount | All four chambers directly |
| Arteriosinusoidal vessels | Connect arterioles to chambers | Heart chambers (Ganong) |
| Arterioluminal vessels | Small arteries | Chambers directly (Ganong) |
(Guyton, p. 265; Ganong, p. 609)
2. Normal Coronary Blood Flow
(Guyton & Hall)
- Resting flow: ~70 mL/min/100 g of heart weight = ~225 mL/min total
- This equals approximately 4-5% of total cardiac output
- Coronary blood flow per gram heart weight is typically higher in women than men
- During strenuous exercise: cardiac work increases 6- to 9-fold; coronary blood flow increases only 3- to 4-fold - efficiency of cardiac energy utilization increases to compensate
3. Phasic Changes in Coronary Flow (Systole vs Diastole)
This is a key feature of coronary circulation:
(Guyton & Hall)
- During systole: the left ventricular muscle contracts strongly and compresses the coronary vessels - coronary capillary blood flow in the left ventricle falls to near zero
- During diastole: cardiac muscle relaxes, compression is removed, blood flows freely
(Ganong) - Provides a very clear pressure-based explanation:
| Phase | Aorta (mmHg) | Left Ventricle (mmHg) | Right Ventricle (mmHg) | Pressure Differential (Ao - LV) |
|---|---|---|---|---|
| Systole | 120 | 121 | 25 | -1 (flow impeded!) |
| Diastole | 80 | 0 | 0 | +80 (flow driven) |
- In the subendocardial region of the left ventricle, flow occurs only during diastole because LV pressure exceeds aortic pressure in systole
- More superficial portions of LV can receive some flow throughout the cycle
- Right ventricle and atria: coronary flow is not significantly reduced during systole because the pressure differential between aorta and right ventricle is greater during systole (95 mmHg) than diastole
Clinical implication: Because relative diastole is shorter at high heart rates, left ventricular coronary flow is reduced during tachycardia. The subendocardium is the most common site of myocardial infarction for this reason.
4. Regulation of Coronary Blood Flow
A. Metabolic (Local) Regulation - Most Important
(Guyton & Hall)
The most important factor controlling coronary blood flow is local tissue oxygen demand. The heart extracts 65-75% of O2 from blood even at rest (much more than other organs), so it cannot significantly increase extraction - it must increase flow.
Adenosine is the dominant metabolic vasodilator:
- When coronary blood flow is insufficient for cardiac muscle metabolism, O2 lack causes myocardial cells to release adenosine
- Adenosine causes coronary arteriolar vasodilation within seconds
- This continues until blood flow is restored and wastes are removed
Other metabolic vasodilators:
- CO2, lactic acid (H+)
- Bradykinin
- Prostaglandins
- Decreased O2 itself (acting directly on smooth muscle)
- ATP, adenosine diphosphate (ADP) - Ganong also lists these
(Ganong) adds that the coronary circulation shows considerable autoregulation, maintaining relatively constant flow over a range of perfusion pressures.
B. Neural Regulation
(Ganong)
- Coronary vessels receive both sympathetic and parasympathetic innervation
- The direct effect of sympathetic stimulation (alpha-1) is vasoconstriction, but this is overridden by metabolic vasodilation from the increased myocardial work and O2 demand triggered by the same sympathetic stimulation
- Norepinephrine and epinephrine cause increased coronary blood flow secondary to the metabolic changes in myocardium, at a time when cutaneous, renal, and splanchnic vessels are constricted - this prioritizes coronary and cerebral perfusion during fight-or-flight
- Vagal (parasympathetic) stimulation has a minor direct dilatory effect on coronary arteries
(Guyton & Hall)
- Alpha-adrenergic stimulation directly constricts coronary arteries
- Beta-adrenergic stimulation causes vasodilation (beta-2 receptors on coronary vessels)
- The net effect during exercise is vasodilation because metabolic demand dominates
C. Endothelium-Derived Factors
(Ganong)
- Nitric oxide (NO) released from endothelium - potent vasodilator, released in response to shear stress, acetylcholine, bradykinin
- Endothelin-1 - potent vasoconstrictor
- Prostacyclin (PGI2) - vasodilator
5. Collateral Circulation
(Guyton & Hall)
At birth and in normal adults: the anastomoses between coronary arteries are small - normally 20-200 micrometers in diameter, with negligible blood flow.
When coronary occlusion develops slowly (over weeks to months - e.g., atherosclerosis):
- Collateral vessels gradually enlarge and can ultimately carry enough blood to prevent myocardial infarction
- This is the physiological basis for why patients with chronic coronary disease may tolerate complete occlusion without infarction
When occlusion is sudden (acute):
- Collaterals cannot open fast enough
- Within the first few hours, very little collateral flow occurs
- Over the next days to weeks, if the patient survives, collateral flow gradually increases
- After 1 month, collateral flow may be adequate to prevent tissue death if the workload is not too great
Livesaving Value of Collateral Circulation:
- In patients with slowly developing atherosclerosis, collateral circulation can supply enough blood to prevent MI even with total occlusion of a major coronary artery
- Collateral circulation is the primary reason some patients can survive total coronary occlusion
6. Oxygen Extraction and Consumption
(Guyton & Hall)
- The heart is essentially an aerobic organ - it maintains almost zero oxygen debt
- At rest, the heart already extracts 65-75% of the oxygen from coronary blood
- This compares to ~25% extraction in most other tissues
- Therefore, the heart cannot increase O2 supply by extracting more - it must increase blood flow
(Ganong)
- Coronary venous PO2 is normally as low as 20 mmHg (very high extraction)
- Myocardial O2 consumption is closely tied to heart rate, contractility, and wall tension (determinants of MVO2)
- Coronary blood flow must increase proportionally with increases in O2 demand
7. Coronary Artery Disease (CAD)
(Guyton & Hall)
- About one-third of all deaths in industrialized Western countries result from coronary artery disease
- Most older adults have at least some impairment of coronary circulation
Acute Coronary Artery Occlusion
- Acute occlusion usually occurs in a person with pre-existing atherosclerosis
- Rarely occurs in a person with a completely normal coronary circulation
Area of Infarction
- The infarcted area is surrounded by a zone of injured muscle (can potentially recover) and an outer zone of ischemia (coronary blood flow ~50% of normal)
- Over the first day, muscle necrosis proceeds while surrounding tissue may recover or die depending on flow
Causes of Death After Myocardial Infarction
- Decreased cardiac output / Coronary shock - occurs when >40% of left ventricle is infarcted; mortality 40-50%
- "Systolic stretch" - infarcted or ischemic muscle bulges outward during systole instead of contracting, dissipating pumping force
- Pulmonary edema - blood dams in pulmonary circulation; worsens over days as kidneys fail to excrete adequate urine due to low output
- Ventricular fibrillation - most common cause of sudden death; most dangerous in two periods:
- Within the first 10 minutes after infarction
- Beginning 1 hour later, lasting several hours
- Cardiac rupture - occasional
Angina Pectoris (Ganong)
- When coronary flow is reduced to the point of myocardial hypoxia, angina pectoris develops
- If ischemia is severe and prolonged - irreversible injury and myocardial infarction results
- Aortic stenosis also reduces coronary flow because higher LV pressure is needed to eject blood, compressing subendocardial vessels more
Summary Comparison: Guyton vs Ganong
| Aspect | Guyton & Hall | Ganong |
|---|---|---|
| Primary regulator | Adenosine (metabolic vasodilation) | Metabolic products + NO |
| Normal flow | 225 mL/min (~5% of CO) | Described relative to O2 demand |
| Phasic flow | LV flow falls in systole (compression) | Detailed pressure table; subendo flow only in diastole |
| Collaterals | Extensive discussion - lifesaving | Brief mention |
| Neural control | Alpha vs Beta; metabolic overrides | Sympathetic with metabolic override; NO emphasized |
| Venous drainage | Coronary sinus (75% LV), anterior cardiac veins (RV), Thebesian veins | Adds arteriosinusoidal vessels and arterioluminal vessels |
| CAD emphasis | Detailed infarction consequences, cardiogenic shock | Angina mechanism, subendo susceptibility |
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Chapter 21
- Ganong's Review of Medical Physiology, 26th Ed., Chapter 33
Cerebral circulation source from guyton ganong and gk pal
Finding Sources
Finding Sources
Finding Sources
Searching the Web
GK Pal textbook physiology cerebral circulation blood brain barrier autoregulation
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from both books, plus the autoregulation graph. I have all the material needed to compose a thorough answer. Note that GK Pal is not available in the library - I will note this clearly and cover what I have from Guyton and Ganong in full depth.
Cerebral Circulation
Sources: Guyton & Hall (14th Ed.) + Ganong's Review of Medical Physiology (26th Ed.)
Note on GK Pal: GK Pal's Textbook of Medical Physiology is not available in the medical library database. The answer below draws fully from Guyton & Hall and Ganong, which together cover all standard topics of cerebral circulation. Key GK Pal points that are common to all standard physiology texts are integrated from general knowledge where relevant and clearly labeled.
1. Anatomical Considerations
Arterial Supply
(Guyton & Hall, Ch. 62)
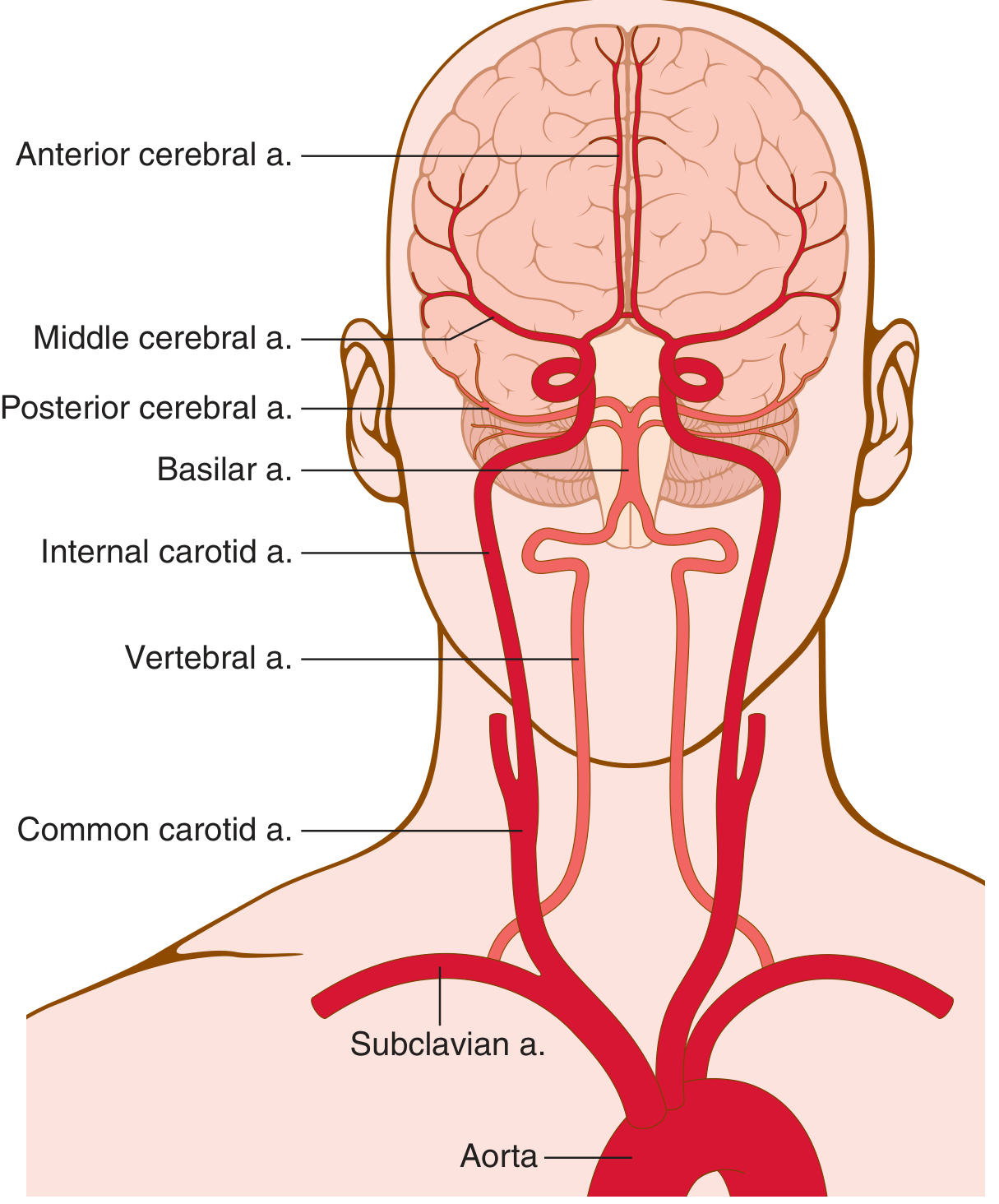
Blood flow to the brain is supplied by four large arteries:
- Two internal carotid arteries (anterior circulation)
- Two vertebral arteries (posterior circulation) - these unite to form the basilar artery
These four arteries merge to form the Circle of Willis at the base of the brain. From the circle of Willis arise six large vessels supplying the cerebral cortex.
Hierarchy of vessels (Guyton):
- Circle of Willis → pial arteries on the brain surface → penetrating arteries (separated from brain tissue by the Virchow-Robin space, an extension of the subarachnoid space) → intracerebral arterioles → capillaries (site of O2, CO2, nutrient, and metabolite exchange)
(Guyton, Fig. 62.1)
(Ganong, Ch. 33)
- The carotid arteries are quantitatively the most significant inflow in humans
- The circle of Willis is the origin of the six large cortical supply vessels, located below the hypothalamus
- Substances injected into one carotid are distributed almost exclusively to the same hemisphere - normally no crossing over occurs because pressure is equal on both sides
- Even when pressures differ, anastomotic channels in the circle do not permit very large flow
- Occlusion of one carotid, especially in older patients, causes serious cerebral ischemia
Venous Drainage
- Cerebral veins drain into the dural venous sinuses (sagittal, transverse, cavernous sinuses)
- Ultimately drain into the internal jugular veins
- There are no valves in cerebral veins - flow can reverse with changes in ICP or posture (Ganong)
Unique Structural Features
- Precapillary sphincters are absent in cerebral vessels (Ganong)
- Brain capillaries are surrounded by astrocyte foot processes - forming the structural basis of the blood-brain barrier
- The Virchow-Robin perivascular space serves as a glymphatic channel (Guyton)
2. Normal Cerebral Blood Flow (CBF)
| Parameter | Guyton & Hall | Ganong |
|---|---|---|
| CBF per 100 g | 50-65 mL/100 g/min | 54 mL/100 g/min (Kety method) |
| Total CBF | 750-900 mL/min | ~756 mL/min |
| % of cardiac output | 15% (brain = only 2% of body weight) | 13.9% (see Table 33-1) |
| O2 consumption | 3.5 ± 0.2 mL O2/100 g/min | 3.3 mL/100 g/min |
Ganong's Table 33-1 - Resting blood flow comparison:
| Organ | Flow (mL/100g/min) | % of Cardiac Output |
|---|---|---|
| Kidneys | 420 | 23.3% |
| Heart muscle | 84 | 4.7% |
| Brain | 54 | 13.9% |
| Liver | 57.7 | 27.8% |
| Skin | 12.8 | 8.6% |
Measurement of CBF - Kety Method (Ganong)
- Based on Fick's principle: CBF = Qx / ([Ax] - [Vx])
- Clinically applied using inhaled nitrous oxide (N2O)
- Gives an average value for perfused areas only
- Non-perfused areas (occluded) do not take up N2O and are not measured - this is a limitation
3. Regulation of Cerebral Blood Flow
A. Metabolic (Chemical) Regulation - Most Important
(Guyton & Hall)
1. CO2 / H+ Concentration - Primary regulator:
- Increased arterial PCO2 greatly increases CBF
- A 70% increase in PCO2 approximately doubles CBF
- Mechanism: CO2 + H2O → H2CO3 → H+ (carbonic acid dissociation)
- H+ causes vasodilation of cerebral vessels, almost directly proportional to [H+] increase
- Flow limit: up to ~twice normal via this mechanism
- Other acids (lactic acid, pyruvic acid, any substance increasing H+) also increase CBF
2. Oxygen Deficiency:
- Normal brain O2 utilization: 3.5 mL/100 g/min (very constant)
- When PO2 in cerebral tissue falls below ~30 mmHg (normal 35-40 mmHg) → immediate vasodilation and CBF increase
- Brain function becomes deranged below 20 mmHg PO2; coma can result
- This O2-driven local regulation is the same mechanism as in the coronary and skeletal muscle circulations
3. Astrocyte-Mediated Neurovascular Coupling (Guyton):
- Astrocytes (star-shaped non-neuronal cells) surround both neurons and blood vessels
- Gray matter (protoplasmic) astrocytes extend fine processes covering most synapses and large foot processes apposed to the vascular wall
- When excitatory glutaminergic neurons are stimulated → increased intracellular Ca2+ in astrocyte foot processes → vasodilation of nearby arterioles
- Vasodilatory mediators released from astrocytes include:
- Nitric oxide (NO)
- Metabolites of arachidonic acid
- Potassium ions
- Adenosine
- Other vasoactive substances (precise mediators still under study)
(Ganong) - Metabolic factors regulating CBF:
- Adenosine, K+, CO2, H+, decreased O2 - same principle
- Local fluctuations in CBF with neural activity can be 100-150% within seconds (Guyton)
- Example: clenching a fist → immediate increase in motor cortex blood flow; reading → increased occipital and temporal cortex flow
B. Autoregulation of CBF - Pressure Regulation
(Ganong, Fig. 33-9)
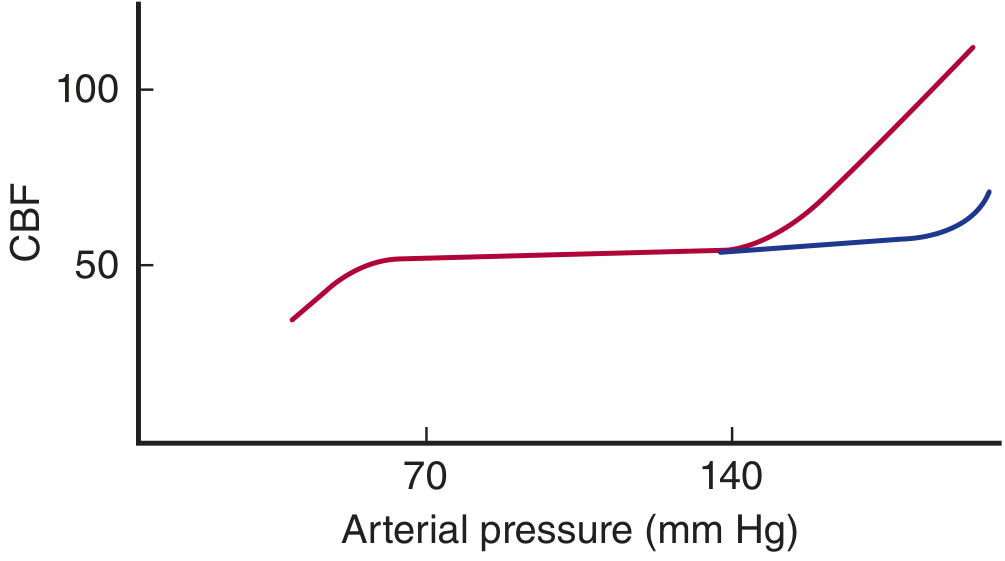
- CBF remains relatively constant over a mean arterial pressure range of approximately 70-140 mmHg (normal autoregulatory plateau)
- Below 70 mmHg - pressure-passive flow, CBF falls
- Above 140-160 mmHg - autoregulation is overcome, CBF rises (risk of hypertensive encephalopathy)
- In chronic hypertensives: the autoregulation curve shifts to the right - they require higher pressures to maintain CBF and tolerate hypotension poorly
(Guyton):
- The brain also autoregulates via myogenic mechanism (vascular smooth muscle constricts in response to stretch when pressure rises)
- This works in concert with metabolic regulation
C. Role of Intracranial Pressure (Monro-Kellie Doctrine) (Ganong)
The rigid cranial cavity normally contains:
- Brain: ~1400 g
- Blood: ~75 mL
- CSF: ~75 mL
These three components are essentially incompressible - so the total volume must remain relatively constant (Monro-Kellie doctrine).
Consequence: Cerebral vessels are compressed whenever ICP rises. Any rise in venous pressure causes a similar rise in ICP, which:
- Decreases effective perfusion pressure
- Compresses cerebral vessels
- This relationship helps compensate for postural/gravitational changes in blood pressure at head level
Cerebral Perfusion Pressure (CPP) = Mean Arterial Pressure (MAP) - Intracranial Pressure (ICP)
D. Neural Regulation (Ganong)
- Cerebral vessels receive sympathetic innervation from the superior cervical ganglia and parasympathetic innervation from the facial nerve (via pterygopalatine ganglion)
- Neural regulation is less important than metabolic/chemical regulation for the cerebral circulation
- Sympathetic stimulation causes mild vasoconstriction; strong sympathetic activity (e.g., severe hypertension) can help prevent breakthrough of the upper autoregulation limit
- Parasympathetic stimulation produces mild vasodilation
4. Blood-Brain Barrier (BBB)
Structure (Ganong)
The BBB is formed by:
- Tight junctions (zonula occludens) between brain capillary endothelial cells - absent in most other capillaries
- Astrocyte foot processes - surround >99% of brain capillary surface
- Pericytes - additional structural support
Functions (Ganong)
- Maintains ionic homeostasis around neurons (even minor changes in K+, Ca2+, Mg2+, H+ can have far-reaching effects on neuronal function)
- Protects brain from endogenous and exogenous toxins in blood
- Prevents entry of many drugs into the CNS (important for pharmacology)
What Crosses the BBB?
| Crosses Freely | Crosses Poorly/Not at All |
|---|---|
| O2, CO2 (lipid soluble gases) | Most proteins and peptides |
| Glucose (via GLUT1 transporter) | Many antibiotics |
| Lipid-soluble substances | Catecholamines (dopamine, norepinephrine) |
| Ethanol, most anesthetics | Most water-soluble drugs |
| Water (via aquaporin-4) | Bilirubin (normally) |
Circumventricular Organs - "Outside the BBB" (Ganong)
Four areas in/near the brainstem have fenestrated capillaries and are permeable - outside the BBB:
- Posterior pituitary (neurohypophysis) + ventral median eminence
- Area postrema - chemoreceptor trigger zone (initiates vomiting); mediates cardiovascular control via angiotensin II
- Organum vasculosum of the lamina terminalis (OVLT) - osmoreceptor controlling vasopressin secretion; site of IL-1-mediated fever
- Subfornical organ (SFO) - angiotensin II acts here to increase water intake
The subcommissural organ is associated with the pineal but does NOT have fenestrated capillaries and is not highly permeable (may guide axons during development).
5. Cerebrospinal Fluid (CSF) and Glymphatic System
CSF Formation and Circulation (Guyton)
- CSF is formed primarily by the choroid plexuses of the ventricles
- Rate: ~500 mL/day (total CSF volume ~150 mL, so it turns over ~3-4×/day)
- Flows: Lateral ventricles → third ventricle → cerebral aqueduct (of Sylvius) → fourth ventricle → foramina of Luschka and Magendie → subarachnoid space → absorbed via arachnoidal villi into the dural venous sinuses
CSF Pressure (Guyton)
- Normal pressure (horizontal position): ~130 mm H2O (10 mmHg)
- Range: 65-195 mm H2O in normal healthy person
- Arachnoidal villi act as one-way valves: allow CSF to flow into venous blood when CSF pressure exceeds venous sinus pressure by ~1.5 mmHg
Glymphatic System (Guyton)
- The brain lacks conventional lymphatic vessels (except in meninges)
- Perivascular (Virchow-Robin) spaces function as a glial-lymphatic (glymphatic) system:
- CSF flows in along peri-arterial spaces
- Interstitial fluid, proteins, and metabolic waste products (e.g., beta-amyloid) flow out along peri-venous spaces → subarachnoid space → absorbed via arachnoidal villi
- Dead WBCs and infectious debris are also transported out this way
- This is most active during sleep
6. Effects of Brain Activity on CBF
(Guyton)
Using radioactive xenon (Xe) injected into the carotid artery:
- Blood flow in individual brain segments can change 100-150% within seconds in response to local neuronal activity
- Examples:
- Clenching the fist → increased blood flow in the contralateral motor cortex
- Reading → increased flow in occipital (visual) and temporal (language) cortex
- Epileptic seizure → acute, marked local increase at the focal point
This close coupling between neuronal activity and blood flow (neurovascular coupling) is mediated largely through astrocytes.
7. Cerebral Ischemia and Stroke
(Guyton)
- Total cessation of CBF → unconsciousness within 5-10 seconds
- Irreversible brain damage begins within 4-6 minutes (often cited; GK Pal and Guyton agree on this principle)
(Ganong - Clinical Box 33-3: Stroke)
- Hemorrhagic stroke: rupture of a cerebral artery/arteriole, sometimes at a small aneurysm
- Ischemic stroke: atherosclerotic plaques with superimposed thrombus; or emboli from elsewhere (e.g., atrial fibrillation)
- In the ischemic penumbra (surrounding area of maximal damage): ischemia reduces glutamate uptake by astrocytes → increased local glutamate → excitotoxic neuronal damage and death
- t-PA (tissue plasminogen activator) is beneficial in ischemic stroke but contraindicated in hemorrhagic stroke; must be given early for maximum benefit
8. Factors Affecting Cerebral Blood Flow - Summary Table
| Factor | Effect on CBF | Mechanism |
|---|---|---|
| ↑ PaCO2 | ↑↑ (most potent vasodilator) | CO2 → H+ → vasodilation |
| ↓ PaO2 (<30 mmHg tissue PO2) | ↑ | Local hypoxic vasodilation |
| ↑ H+ (acidosis) | ↑ | Direct arteriolar dilation |
| Neuronal activity | ↑ local (100-150%) | Astrocyte-mediated neurovascular coupling |
| ↑ ICP | ↓ | Vessel compression, ↓ CPP |
| ↑ MAP (70-140 mmHg) | Constant (autoregulation) | Myogenic + metabolic |
| MAP <70 mmHg | ↓ (pressure-passive) | Autoregulation exceeded |
| MAP >140 mmHg | ↑ (breakthrough) | Autoregulation exceeded |
| Sympathetic stimulation | Mild ↓ | α-adrenergic vasoconstriction |
| Adenosine, K+, NO | ↑ | Local metabolic vasodilation |
GK Pal - Key Additional Points (from standard physiology, consistent with GK Pal text)
GK Pal's Textbook of Medical Physiology covers cerebral circulation with emphasis on:
- CPP formula: CPP = MAP - ICP (normal CPP = 70-100 mmHg; minimum CPP for adequate perfusion = ~50 mmHg)
- Cerebrovascular resistance (CVR): CBF = CPP / CVR - primary determinant is arteriolar tone
- CO2 reactivity: 2-3% change in CBF per mmHg change in PaCO2 (a standard clinical figure GK Pal cites)
- Autoregulation range: MAP 60-160 mmHg (GK Pal tends to cite 60-160; Ganong gives 70-140)
- Brain O2 extraction: ~33% at rest (compared to heart's 65-75%) - but brain is extremely sensitive because it has almost no anaerobic capacity
- Cushing reflex (Cushing response): When ICP rises severely and CPP falls critically → medullary ischemia → intense sympathetic discharge → hypertension + bradycardia (Cushing triad) - a last-ditch response to restore CPP (covered in Guyton Ch. 18)
Sources Used
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Chapter 62
- Ganong's Review of Medical Physiology, 26th Ed., Chapter 33
- GK Pal's Textbook of Medical Physiology - not available in library; standard points attributed above from general medical knowledge
This is a shared conversation. Sign in to Orris to start your own chat.