Ovarian cyst
Reading File
Finding Sources
Searching PubMed
"ovarian cyst" management
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Ovarian Cyst
An ovarian cyst is a fluid-filled sac that develops on or within an ovary. They are extremely common, especially during the reproductive years, and most are benign and self-limiting.
Classification
1. Functional (Physiologic) Cysts
These arise from normal menstrual cycle activity and are the most common type. They are all benign and usually require no surgical treatment.
| Type | Mechanism | Features |
|---|---|---|
| Follicular cyst | Dominant follicle fails to rupture or involute; grows >3 cm | Most common functional cyst; rarely >8 cm; thin-walled, unilocular |
| Corpus luteum cyst | Post-ovulatory corpus luteum persists instead of involuting | Can hemorrhage; may mimic ectopic pregnancy; ruptures preferentially on right side, cycle days 20-26 |
| Theca lutein cyst | Excess beta-hCG stimulation or hypersensitivity | Usually bilateral; associated with hydatidiform mole, choriocarcinoma, clomiphene, multiple gestations, OHSS |
Cigarette and marijuana smoking increase risk of functional cysts. Oral contraceptive use (especially monophasic) reduces the risk by suppressing follicular development and ovulation, though they do NOT hasten resolution of existing cysts.
- Berek & Novak's Gynecology, p. 452
- Grainger & Allison's Diagnostic Radiology, p. 905
2. Non-functional Benign Cysts / Masses
- Endometrioma ("chocolate cyst"): Ectopic endometrial tissue within the ovary; typically 6-8 cm; contains thick brown fluid; associated with endometriosis, dysmenorrhea, dyspareunia
- Dermoid cyst (benign cystic teratoma): Germ cell neoplasm; contains fat, hair, skin, teeth; most common benign ovarian tumor in women <50 years; risk of torsion ~15%; bilateral in ~10% of cases; malignant transformation <2%
- Serous / mucinous cystadenoma: Epithelial tumors; serous cystadenomas are more common in older women; 5-10% of serous tumors have borderline malignant potential
3. Hemorrhagic Cyst
Occurs when a blood vessel in the cyst wall ruptures, filling the cyst with blood. Can develop from either follicular or corpus luteum cysts. On ultrasound, shows characteristic evolving appearances:
| Phase | US Appearance |
|---|---|
| Acute hemorrhage | Iso- to hyperechoic heterogeneous echoes; smooth wall |
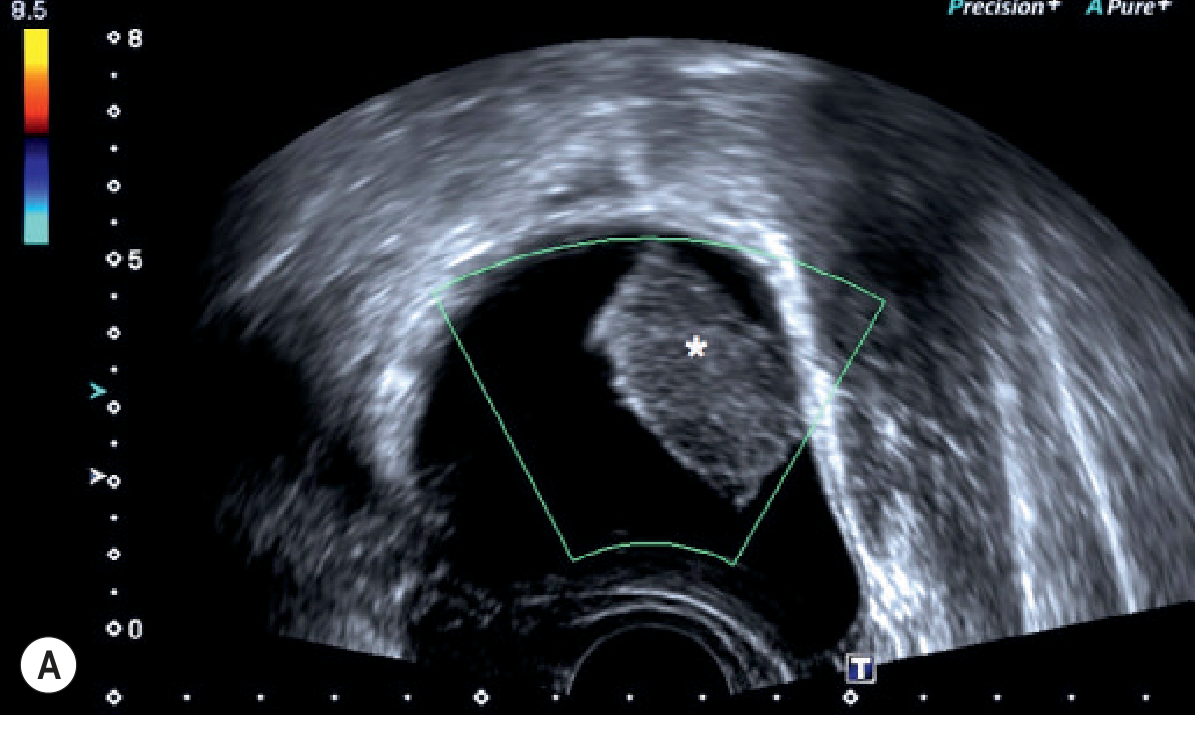
| Subacute (days-weeks) | Retracted avascular mural nodule ("retracted clot"); "jiggle" sign |
| Later (weeks) | Fibrin strands giving a "fish net" or "cobweb" appearance |
- Grainger & Allison's Diagnostic Radiology, p. 905
Hemorrhagic corpus luteal cyst on transvaginal ultrasound - note the retracted echogenic mural clot (asterisk):
Clinical Features
Presentation:
- Most are asymptomatic and discovered incidentally on imaging or pelvic exam
- When symptomatic: sudden-onset unilateral pelvic pain, more common on the right
- Pain often starts during physical activity or sexual intercourse
- Cervical motion tenderness and mild vaginal bleeding may be present
Complications:
-
Rupture: The corpus luteum cyst is the most common to rupture. Sudden onset severe pelvic pain, dizziness, syncope if significant hemoperitoneum develops. Ruptured corpus luteum cyst can closely mimic a ruptured ectopic pregnancy.
-
Torsion: More common with dermoid cysts due to high fat content (float freely). Risk ~15% for dermoids.
-
Hemorrhage: Patients on anticoagulants or with bleeding diatheses are at higher risk.
-
Rupture of endometrioma/dermoid: Causes chemical peritonitis; blood loss is typically minimal but pain is severe.
-
Berek & Novak's Gynecology, p. 560
-
Tintinalli's Emergency Medicine, p. 655
Diagnosis
Ultrasound (first-line):
- Transvaginal ultrasound (TVUS) is preferred - higher resolution
- Benign features: thin-walled, unilocular, no internal vascularity, no solid components
- Follicular cyst: thin-walled, hypoechoic, unilocular; low T1 / high T2 on MRI
- Worrying features: large (>8 cm), multiloculated, solid components, thick septations, internal flow on Doppler
Criteria for concern (possible neoplasm):
- Size >8 cm
- Solid or multiloculated morphology
- Postmenopausal patient - any ovarian mass should be considered malignant until proven otherwise
- Rapid growth
Lab tests:
- Beta-hCG to exclude ectopic pregnancy / gestational trophoblastic disease
- CA-125 (if malignancy suspected, especially postmenopausal)
- CBC if rupture/hemorrhage suspected
Management
Expectant (watchful waiting)
- Cysts <8 cm, unilocular, unilateral in a reproductive-age woman
- Functional cysts typically resolve in 4-8 weeks (follicular) or after 6-12 weeks follow-up US (corpus luteum)
- Uncomplicated ruptured cysts in hemodynamically stable patients can be managed conservatively with observation and repeat imaging
Medical
- Combined hormonal contraceptives: Recommended in women with recurrent functional ovarian cyst formation (suppresses ovulation). Do NOT accelerate resolution of existing cysts.
Surgical indications
- Hemodynamic instability from hemorrhage/hemoperitoneum
- Suspected torsion
- Chemical peritonitis (ruptured dermoid or endometrioma)
- Ruptured abscess (life-threatening)
- Cysts with suspicious features for malignancy
- Large (>8 cm), persistent, or symptomatic cysts not resolving with observation
Surgical approach:
-
Cystectomy (removing only the cyst, preserving the ovary) is preferred over oophorectomy in reproductive-age women to preserve fertility
-
Laparoscopic cystectomy is the minimally invasive approach of choice for benign masses
-
Even if very little ovarian tissue remains, preserving a small amount of cortex in a young patient is preferable to oophorectomy
-
Harrison's Principles of Internal Medicine 22E, p. 866
-
Berek & Novak's Gynecology, p. 453-454
Special Populations
| Population | Key Points |
|---|---|
| Pregnancy | New fluid levels or mixed echogenicity in a cyst may indicate torsion; fetal ovarian cysts also occur |
| Postmenopausal | Any ovarian mass is malignant until proven otherwise; refer to gynecology |
| Adolescents | Dermoid cysts most common; fertility-sparing surgery strongly preferred |
| On anticoagulants | High risk for corpus luteum cyst hemorrhage and hemoperitoneum |
Differential Diagnosis of Pelvic Mass / Ovarian Cyst
-
Ectopic pregnancy
-
Tubo-ovarian abscess / PID
-
Endometrioma
-
Ovarian torsion
-
Paraovarian/paratubal cyst
-
Hydrosalpinx
-
Uterine fibroid (subserosal)
-
Ovarian malignancy
-
Berek & Novak's Gynecology, p. 556
-
Tintinalli's Emergency Medicine, p. 655
This is a shared conversation. Sign in to Orris to start your own chat.