Malaria give me laq formate microbiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough LAQ-format answer. Let me compile it:
MALARIA - Long Answer Question (LAQ) Format
Microbiology
1. DEFINITION
Malaria is an acute infectious disease caused by obligate intracellular protozoan parasites of the genus Plasmodium, transmitted to humans through the bite of an infected female Anopheles mosquito. It accounts for ~216 million episodes with approximately 500,000 deaths annually, 90% occurring in Africa.
2. CAUSATIVE ORGANISM / CLASSIFICATION
| Parasite | Type of Malaria | Fever Cycle |
|---|---|---|
| P. vivax | Benign tertian malaria | 48 hrs |
| P. ovale | Benign tertian (ovale malaria) | 48 hrs |
| P. malariae | Quartan malaria | 72 hrs |
| P. falciparum | Malignant tertian malaria | 36-48 hrs (irregular) |
| P. knowlesi | Simian / Quotidian malaria | 24 hrs |
Classification: Kingdom Protista → Phylum Apicomplexa (Sporozoa) → Order Eucoccidiida → Genus Plasmodium
3. LIFE CYCLE
The life cycle involves two hosts: the female Anopheles mosquito (definitive host - sexual cycle) and humans (intermediate host - asexual cycle).
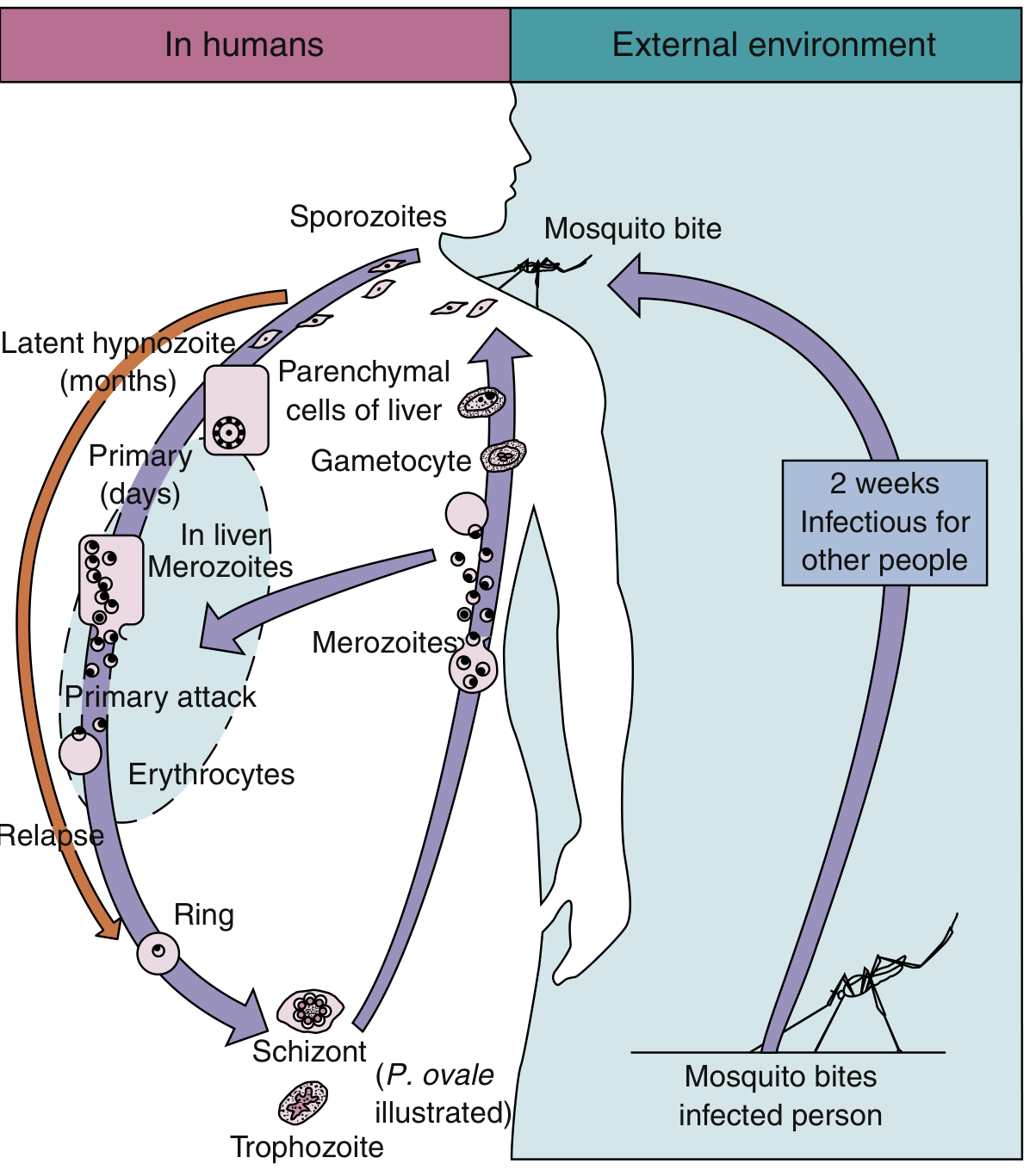
A. In the Mosquito (Sexual Phase - Sporogony)
- Mosquito ingests male and female gametocytes from infected human blood
- Fertilization occurs in the mosquito midgut → ookinete (motile zygote)
- Ookinete penetrates gut wall → oocyst
- Sporogony occurs within oocyst → sporozoites released
- Sporozoites migrate to salivary glands; mosquito becomes infective in ~2 weeks
B. In the Human (Asexual Phase)
I. Exoerythrocytic (Pre-erythrocytic / Hepatic) Phase:
- Mosquito bite → sporozoites injected into bloodstream
- Sporozoites travel to liver → invade hepatic parenchymal cells
- Schizogony occurs → hepatic schizonts → rupture → release merozoites
- Duration: 8-25 days (species-dependent)
- P. vivax and P. ovale: some sporozoites become dormant hypnozoites (sleeping forms) in hepatocytes → responsible for RELAPSE months to years later
II. Erythrocytic Phase (responsible for symptoms):
- Merozoites attach to specific RBC surface receptors → invade erythrocytes
- Progression: Ring stage → Trophozoite → Schizont → Merozoites
- Mature schizont ruptures RBC → merozoites released → invade new RBCs
- This synchronous rupture causes the periodic fever spikes
- After several cycles, some merozoites → gametocytes (sexual forms)
Cycle durations:
- P. vivax / P. ovale: 48 hours (tertian - fever every 3rd day)
- P. malariae: 72 hours (quartan - fever every 4th day)
- P. falciparum: 48 hours but asynchronous (irregular fevers)
- P. knowlesi: 24 hours (quotidian - daily fever)
4. RBC INVASION - SPECIFICS
| Species | RBCs Invaded | Max Parasitemia | Receptor |
|---|---|---|---|
| P. vivax | Only reticulocytes (immature) | 1-2% | Duffy blood group antigen (Fya/Fyb) |
| P. ovale | Only reticulocytes | 1-2% | - |
| P. malariae | Only senescent (old) RBCs | 1-2% | - |
| P. falciparum | All RBCs regardless of age | Very high (>5%) | Glycophorin A (sialoglycoprotein) |
Key Point: Duffy-negative individuals (common in West African ancestry) are resistant to P. vivax malaria because the Duffy antigen serves as its receptor.
5. PATHOGENESIS
Fever Mechanism
- Synchronous rupture of RBCs → release of merozoites + malarial pigment (hemozoin) + parasite toxins (GPI anchors) → stimulate macrophages → release of IL-1, TNF-α → fever, chills, rigors
Malarial Paroxysm (Classic Triad)
- Cold stage - shivering, rigors (15-60 min)
- Hot stage - high fever 40-41°C (2-6 hrs)
- Sweating stage - profuse sweating, temperature falls
Anemia Mechanisms
- Direct destruction of parasitized RBCs
- Immune-mediated hemolysis of non-parasitized RBCs
- Dyserythropoiesis (bone marrow suppression)
- Splenic sequestration
P. falciparum Specific Pathogenesis (Most Dangerous)
- Infects RBCs of all ages → high parasitemia
- Forms electron-dense knobs on RBC surface → produce PfEMP1 (Plasmodium falciparum erythrocyte membrane protein 1)
- PfEMP1 mediates cytoadherence - binding to endothelium of capillaries and postcapillary venules of brain, placenta, and visceral organs
- Results in microinfarcts → cerebral malaria, placental malaria
Genetic Protective Factors
| Condition | Protection Against | Mechanism |
|---|---|---|
| Sickle cell trait (HbAS) | P. falciparum | HbS polymerizes in low O2 → parasite "starves"; ↑ phagocytosis |
| G6PD deficiency | P. falciparum | Oxidant stress damages parasite |
| Thalassemia | P. falciparum | Fetal Hb retards maturation; enhanced antibody binding |
| HbC, HbD, HbE | P. falciparum | Similar oxidant mechanism |
| Duffy antigen negative | P. vivax | No receptor for invasion |
6. CLINICAL FEATURES
| Symptom | Description |
|---|---|
| Fever | Periodic; pattern depends on species |
| Chills/rigors | Classic paroxysm |
| Headache | Prominent |
| Myalgia/arthralgia | Common |
| Splenomegaly | Chronic infection |
| Anemia | Progressive |
| Jaundice | Hemolytic |
Complications of P. falciparum (Severe / Complicated Malaria)
- Cerebral malaria - altered consciousness, seizures, coma
- Blackwater fever - severe intravascular hemolysis → hemoglobinuria → black/dark urine
- Acute respiratory distress syndrome (ARDS)
- Acute kidney injury
- Hypoglycemia
- Thrombocytopenia
- Placental malaria → low birth weight, maternal anemia
Relapse vs Recrudescence
| Term | Cause | Species |
|---|---|---|
| Relapse | Hypnozoites reactivate from liver | P. vivax, P. ovale |
| Recrudescence | Persistent low-level parasitemia | P. malariae, P. falciparum |
7. MICROSCOPIC MORPHOLOGY (Blood Smear Features)
| Feature | P. vivax | P. falciparum | P. malariae | P. ovale |
|---|---|---|---|---|
| RBC size | Enlarged | Normal/small | Normal | Slightly enlarged, oval |
| Schüffner dots | Present (prominent) | Absent (Maurer clefts) | Absent | Present |
| Rings | Large, 1 chromatin dot | Multiple rings/RBC, accole (applique) forms | Thick, compact | Compact |
| Trophozoite | Amoeboid, irregular | Rarely seen in peripheral smear | Band form (pathognomonic) | Similar to vivax |
| Schizont | 12-24 merozoites (rosette) | 8-24 merozoites (rarely seen peripherally) | 8 merozoites - "rosette/daisy head" | 8 merozoites |
| Gametocyte | Round | Crescent/banana-shaped (pathognomonic) | Round | Round |
Mnemonic for gametocyte shape: Falciparum = Falcate (crescent-shaped)
8. LABORATORY DIAGNOSIS
Gold Standard: Peripheral Blood Smear
- Thick smear: Screening (detects low parasitemia) - stained with Giemsa/Leishman
- Thin smear: Species identification and morphology
- Repeat smears every 6-8 hours x 3 if initial negative
Other Methods
| Test | Principle | Comment |
|---|---|---|
| Rapid Diagnostic Tests (RDTs) | Detect parasite antigens (HRP-2 for P. falciparum; LDH for others) | Quick, no microscope needed; sensitivity: P. falciparum 94-100%, P. vivax 69-85% |
| QBC (Quantitative Buffy Coat) | Acridine orange fluorescent staining | Rapid, needs fluorescence microscope |
| PCR | Detects parasite DNA | Most sensitive/specific; gold standard for species ID; not routine |
| Serology (IFA, ELISA) | Antibody detection | Useful for epidemiology, not acute diagnosis |
| Malaria antigen test | Paracheck, OptiMAL | Point of care |
9. TREATMENT
Goals of Chemotherapy
- Suppressive/Prophylactic - prevent infection and symptoms
- Therapeutic (clinical cure) - eradicate erythrocytic cycle
- Radical cure - eradicate exoerythrocytic (liver) cycle (hypnozoites)
- Gametocidal - destroy gametocytes, prevent transmission
Drug Targets by Stage
| Drug | Mechanism | Stage Targeted |
|---|---|---|
| Chloroquine | Inhibits hemoglobin degradation; raises pH of food vacuole → impairs acid proteases | Erythrocytic (blood schizonticidal) |
| Primaquine | Oxidative damage | Hypnozoites (radical cure); gametocidal |
| Quinine/Quinidine | Similar to chloroquine | Blood schizonticidal |
| Artemisinins | Bind to multiple parasite proteins; prevent gametocyte development | Broad spectrum; reduce transmission |
| Mefloquine | Interferes with hemoglobin digestion | Blood schizonticidal |
| Pyrimethamine + Sulfadoxine (Fansidar) | Blocks folate synthesis (double block) | Blood schizonticidal |
| Doxycycline | Protein synthesis inhibition | Blood schizonticidal (combination) |
| Atovaquone + Proguanil (Malarone) | Electron transport disruption | Broad spectrum; prophylaxis |
Treatment Regimens (Summary)
| Species | First-line Treatment |
|---|---|
| P. vivax / P. ovale (chloroquine-sensitive) | Chloroquine + Primaquine (radical cure) |
| P. vivax (chloroquine-resistant) | Mefloquine ± artesunate + Primaquine |
| P. malariae | Chloroquine alone |
| P. falciparum (uncomplicated) | Artemisinin-based Combination Therapy (ACT) |
| P. falciparum (severe/complicated) | IV Artesunate (preferred) or IV Quinine |
| P. knowlesi | Chloroquine or ACT |
Note: Primaquine must not be given to G6PD-deficient patients (risk of severe hemolytic anemia). Always test G6PD before prescribing.
Drug Resistance
- Chloroquine resistance: widespread in P. falciparum (Africa, Southeast Asia); some P. vivax (Papua New Guinea, Sumatra, Indonesia, Brazil)
- Multi-drug resistance: P. falciparum now variably resistant to all drug groups including artemisinins (especially Southeast Asia)
- Management: Combination therapy (ACT) to slow resistance development
10. PREVENTION AND CONTROL
Personal Protection
- Insecticide-treated bed nets (ITNs) - most effective intervention
- Repellents (DEET)
- Protective clothing (long sleeves, trousers at dusk/dawn)
- Indoor residual spraying (IRS)
Chemoprophylaxis
| Drug | Indication |
|---|---|
| Chloroquine | Travelers to chloroquine-sensitive areas |
| Mefloquine | Chloroquine-resistant areas |
| Atovaquone-Proguanil (Malarone) | Most areas; well tolerated |
| Doxycycline | Alternative; SE Asia |
| Primaquine | P. vivax/P. ovale endemic areas (terminal prophylaxis) |
Vector Control
- Larval control (drainage of stagnant water, larvicides)
- Adult mosquito control (insecticides)
- Biological control
Vaccine
- RTS,S/AS01 (Mosquirix) - approved by WHO (2021) for children in sub-Saharan Africa; provides ~30-40% protection against severe malaria
11. KEY POINTS / MNEMONICS
- "VOMF" - Vivax, Ovale = relapse via hypnozoites; Malariae, Falciparum = recrudescence
- Falciparum = most dangerous: banana gametocytes, knobs, PfEMP1, no hypnozoites but multi-drug resistant
- Quartan malaria (P. malariae) = 72-hr cycle; "band form" trophozoites; associated with nephrotic syndrome in children
- Duffy-negative = naturally resistant to P. vivax
- Blackwater fever = P. falciparum + massive hemolysis + hemoglobinuria
- Thick smear for detection; Thin smear for identification
- Primaquine is the only drug for hypnozoites (radical cure)
Sources: Medical Microbiology 9e (Murray), Sherris & Ryan's Medical Microbiology 8th Edition
This is a shared conversation. Sign in to Orris to start your own chat.