Explain acid base balance and disorders simple words
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have thorough content from multiple authoritative textbooks. Here is a clear, simple explanation of acid-base balance and its disorders.
Acid-Base Balance and Disorders - Explained Simply
What Is Acid-Base Balance?
Your blood must stay within a very narrow pH range of 7.35 - 7.45 (slightly alkaline). pH below this means the blood is too acidic; above this means too alkaline. This balance is critical because nearly every enzyme and chemical reaction in your body depends on it.
Think of it like a seesaw - the body is constantly adjusting to keep that seesaw level.
Key players in the balancing act:
- CO2 (carbon dioxide) - controlled by the lungs (breathing faster removes CO2; breathing slower retains it)
- HCO3- (bicarbonate) - controlled by the kidneys (they save or dump bicarbonate)
- The relationship between them is captured by the Henderson-Hasselbalch equation: pH depends on the ratio of HCO3- to CO2
"The pH of body fluids is maintained within a narrow range despite the normal large acid load produced as a by-product of metabolism. This acid load is efficiently neutralized by buffer systems and ultimately excreted by the lungs and kidneys." - Schwartz's Principles of Surgery
The Buffer System - The Body's First Line of Defense
Buffers are chemicals that absorb extra acid or base instantly to minimize pH changes. The main ones are:
- Bicarbonate-carbonic acid system (extracellular - most important)
- Intracellular proteins and phosphates (inside cells)
- Bone - acts as a long-term reservoir
The 4 Basic Acid-Base Disorders
There are 2 respiratory and 2 metabolic disorders:
| Disorder | pH | Primary Problem | CO2 (PCO2) | Bicarbonate (HCO3-) |
|---|---|---|---|---|
| Respiratory Acidosis | ↓ Low | Lungs can't remove CO2 | ↑↑ High | ↑ (compensatory) |
| Respiratory Alkalosis | ↑ High | Too much CO2 blown off | ↓↓ Low | ↓ (compensatory) |
| Metabolic Acidosis | ↓ Low | Too much acid / loss of bicarbonate | ↓ (compensatory) | ↓↓ Low |
| Metabolic Alkalosis | ↑ High | Loss of acid / gain of bicarbonate | ↑ (compensatory) | ↑↑ High |
(Double arrows = primary cause; single arrows = the body's compensatory response)
1. Respiratory Acidosis
The lungs are not removing enough CO2.
- CO2 + H2O → H2CO3 → H+ + HCO3-
- More CO2 means more H+ ions, which drops the pH = acidic blood
Common causes:
- Severe lung disease (COPD, pneumonia, pulmonary edema)
- Chest wall disease or weak breathing muscles
- Decreased brain drive to breathe (drug overdose, sedation)
Body's compensation: The kidneys slowly save more HCO3- to buffer the extra acid (takes 3-5 days - "chronic" compensation)
Signs: Confusion, headache, drowsiness, CO2 narcosis in severe cases
2. Respiratory Alkalosis
The lungs are blowing off too much CO2 (hyperventilation).
- Less CO2 = fewer H+ ions = pH rises = alkaline blood
Common causes:
- Anxiety or panic attacks
- High altitude (hypoxia drives faster breathing)
- Sepsis (fever drives ventilation)
- Mechanical ventilation set too fast
Body's compensation: Kidneys dump more HCO3- to bring pH back down
3. Metabolic Acidosis
Too much acid in the blood or too much bicarbonate lost - NOT a breathing problem.
Common causes:
- Diarrhea (lose HCO3- in stool)
- Diabetic ketoacidosis (DKA) - ketone acids pile up
- Lactic acidosis - shock or poor tissue perfusion
- Renal failure - kidneys can't excrete acid
- Toxic ingestions - aspirin, methanol, ethylene glycol
Body's compensation: You breathe faster and deeper (Kussmaul respirations) to blow off CO2, which raises pH back up. This is a fast response (minutes to hours).
Anion Gap - a key diagnostic tool:
AG = Na+ - (Cl- + HCO3-) | Normal < 12 mmol/L
- High anion gap (>12) = extra unmeasured acids present (ketones, lactate, toxins) - think MUDPILES: Methanol, Uremia, DKA, Propylene glycol, Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates
- Normal anion gap = loss of bicarbonate (diarrhea, renal tubular acidosis, extra chloride)
4. Metabolic Alkalosis
Too much bicarbonate in the blood or too much acid lost - again, not a breathing problem.
Common causes:
- Vomiting (lose hydrochloric acid from stomach)
- Diuretics (lose H+ and Cl-)
- Excessive antacid use
- Hypokalemia (low potassium drives H+ into cells)
Body's compensation: Breathing slows down to retain CO2 (raise H+), which lowers pH back toward normal. But this compensation is limited - the body won't let oxygen levels drop too far just to fix pH.
How the Body Compensates - Summary
| Primary Disorder | Compensation | Speed |
|---|---|---|
| Metabolic acidosis | Lungs breathe faster (↓ CO2) | Minutes - hours |
| Metabolic alkalosis | Lungs breathe slower (↑ CO2) | Hours |
| Respiratory acidosis | Kidneys retain HCO3- | 3-5 days |
| Respiratory alkalosis | Kidneys excrete HCO3- | 3-5 days |
"Respiratory compensation for metabolic disorders is more rapid and occurs through a change in the respiratory rate. Metabolic compensation for a respiratory disturbance requires renal adjustment and can take 3 to 5 days." - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Important rule: Compensation never fully normalizes the pH - it just moves it back toward 7.4. If it fully corrects, suspect a second separate disorder.
The Acid-Base Map
This diagram from Roberts & Hedges shows where each disorder lands when you plot pH vs CO2:
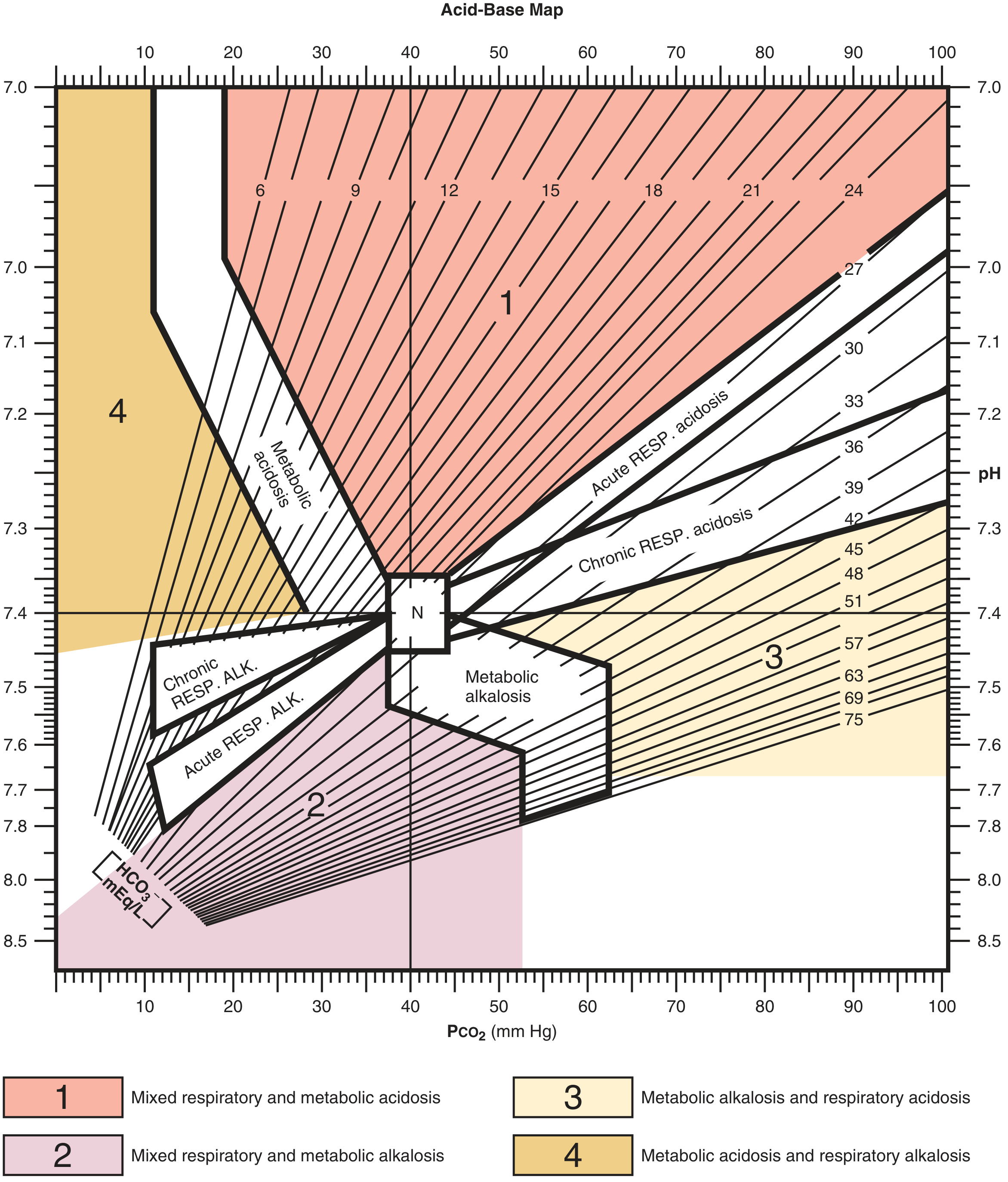
The "N" in the center is normal. Each colored zone is a distinct disorder. Values that fall between zones suggest a mixed disorder (e.g., simultaneous respiratory and metabolic acidosis).
Mixed Disorders
A patient can have two acid-base problems at the same time. For example:
- A patient with COPD (respiratory acidosis) who also develops severe diarrhea (metabolic acidosis) - blood is very acidic from two directions at once
- A septic patient (respiratory alkalosis from hyperventilation) who also develops lactic acidosis
To detect mixed disorders, you compare the predicted compensation formula against the actual measured value. If the actual doesn't match the predicted, a second disorder is hiding.
Quick Step-by-Step ABG Interpretation
- Check pH - is it acidic (<7.35) or alkaline (>7.45)?
- Check CO2 - if CO2 is the main culprit, it's respiratory
- Check HCO3- - if HCO3- is the main culprit, it's metabolic
- Check compensation - does the other value match the formula?
- Calculate anion gap if metabolic acidosis - to find the cause
Sources: Schwartz's Principles of Surgery 11th Ed.; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.