Epidemiology of acute kidney injury.
Reading File
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND epidemiology[MeSH Terms]
Finding Sources
Searching PubMed
"acute kidney injury" AND incidence AND epidemiology
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a comprehensive response. Here is the full synthesis:
Epidemiology of Acute Kidney Injury
1. Definitions and Diagnostic Challenges
AKI is defined by a rise in serum creatinine or a fall in urine output over hours to days. The KDIGO 2012 criteria (serum creatinine rise ≥0.3 mg/dL within 48 hours, or ≥1.5x baseline within 7 days, or urine output <0.5 mL/kg/h for ≥6 hours) are now standard. Because AKI is transient by definition - kidney disease lasting >3 months is CKD - it can only be described by incidence, not prevalence.
Epidemiologic estimates are complicated by several methodologic issues:
- Many studies use billing/diagnostic codes (e.g., ICD-9/ICD-10), which have poor sensitivity - one large VA study found only 49% of creatinine-confirmed AKI had an associated AKI billing code.
- Serum creatinine is only measured during health encounters, introducing ascertainment bias.
- The urine output criterion is relatively recent and inconsistently captured.
- There is no uniform definition for the cause of AKI in large databases.
(Brenner and Rector's The Kidney, p. 860)
2. Incidence
Community-Based Incidence
- Northern California: 522.4 cases/100,000 person-years (all AKI); 29.5 cases/100,000 person-years for dialysis-requiring AKI.
- Scotland: 214.7 cases/100,000 patient-years (all AKI); 18.3 cases/100,000 for dialysis-requiring AKI.
- Canadian cohorts: rates varied enormously - 100 to 11,700 cases/100,000 person-years depending on baseline GFR and proteinuria, demonstrating the huge impact of underlying CKD on susceptibility.
- Among Medicare beneficiaries >65 years: 4.0% had an AKI-coded hospitalization in 1 year.
Hospital-Based Incidence
- A worldwide meta-analysis estimated nearly 25% of hospitalized patients had AKI by the KDIGO definition, with approximately 10% requiring kidney replacement therapy (KRT).
- This estimate is echoed in the ISN global initiative, which cites the same ~25% figure as a call to action to eliminate preventable AKI deaths by 2025.
(Brenner and Rector's The Kidney, p. 860)
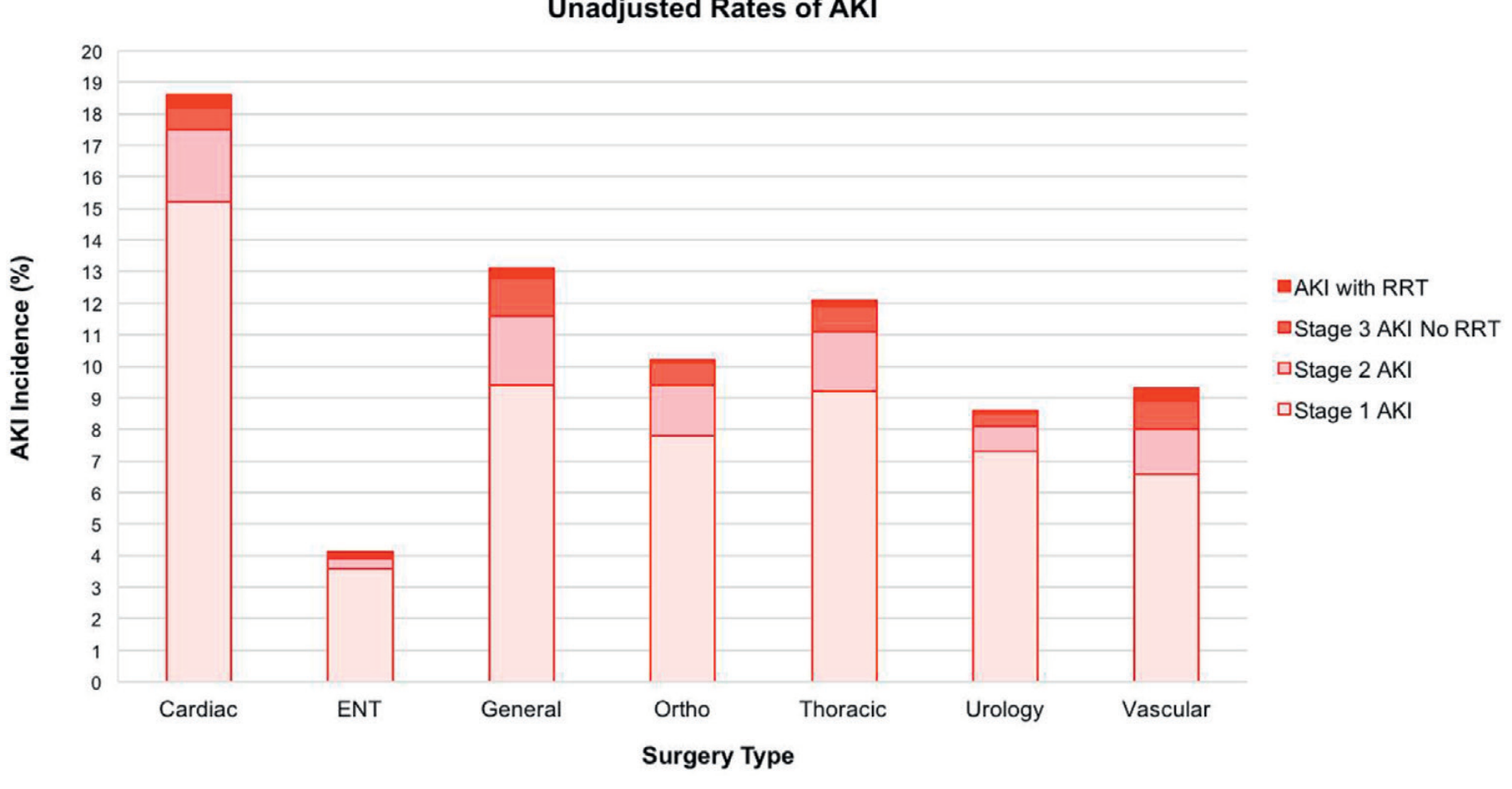
AKI After Major Surgery (7-day incidence)
| Surgery Type | AKI Incidence |
|---|---|
| Cardiac | ~18.7% |
| Thoracic | ~12% |
| General | ~13% |
| Orthopaedic | ~10% |
| Vascular | ~9% |
| Urology | ~8.5% |
| ENT | ~4.1% |
(Fig. 19.20, Brenner and Rector's; Grams et al., Am J Kidney Dis. 2016)
Community-Acquired vs. Hospital-Acquired AKI
Studies in hospitalized patients suggest approximately two-thirds of AKI is community-acquired and one-third is hospital-acquired.
3. Outcomes
AKI is not a self-contained event - it carries major downstream consequences:
- CKD development and progression: The incidence of CKD, eGFR decline, ESKD, and death are all higher after AKI, with risk graded by AKI stage.
- ESKD risk: In one U.S. study, surviving a dialysis-requiring AKI episode was associated with a 2.8x higher risk of progressing to stage G4/G5 CKD.
- Mortality: Even modest creatinine rises confer increased risk. Oliguria alone, even without a rise meeting AKI criteria, may confer higher risk.
- Economic burden: A 2005 study found a serum creatinine rise ≥0.5 mg/dL was associated with 3.5 extra hospital days and $7,500 in excess costs per patient.
- Non-recovery: Many patients with KRT-requiring AKI never recover full kidney function.
- Debate remains over whether adverse outcomes are caused by AKI or simply reflect shared risk factors - no interventional trial has definitively proven causation.
(Brenner and Rector's The Kidney, p. 861)
4. Risk Factors
Patient-Level Risk Factors
- Older age - the single strongest demographic predictor
- Male sex
- Black race - though this may be confounded by socioeconomic disparities; not fully explained by APOL1 risk variants in limited studies
- Diabetes mellitus - 1.5- to 2.5-fold increased odds of AKI
- Pre-existing CKD (lower eGFR) - the strongest modifiable risk factor, in a graded dose-response relationship
- Proteinuria/albuminuria - also confers graded increased risk, independent of eGFR
- Hypertension
The graph below illustrates the strong, graded relationships between lower eGFR, higher albuminuria (ACR), and AKI risk - these associations exist regardless of diabetes status:
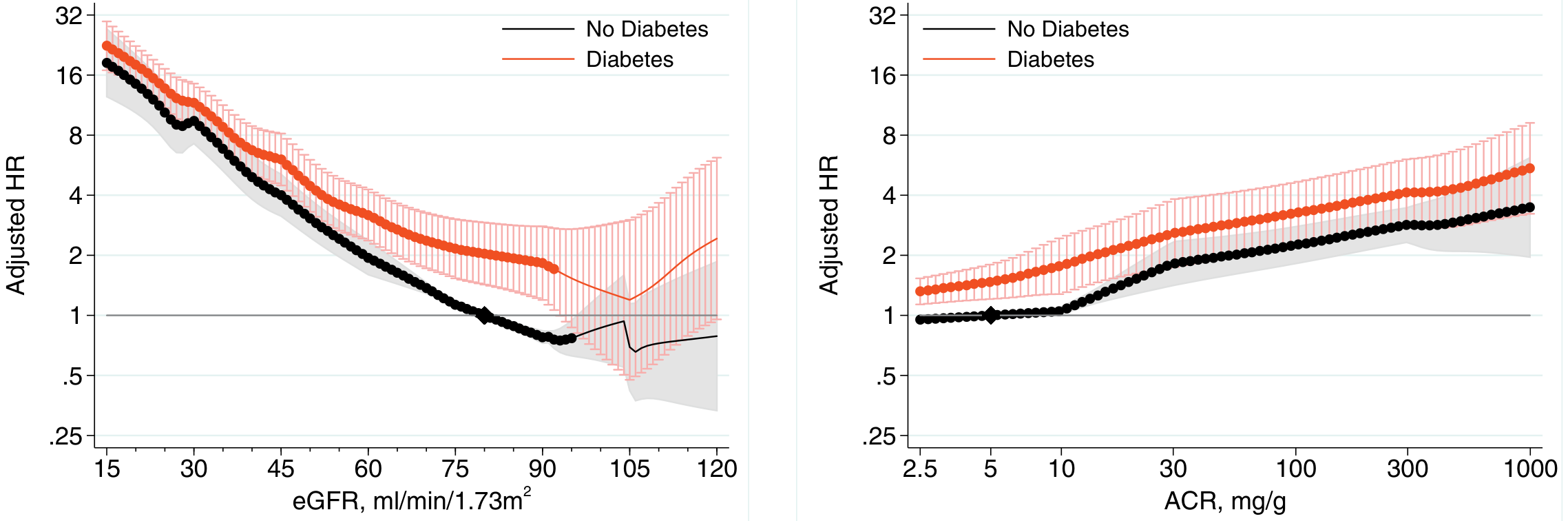
(Fig. 19.21, Brenner and Rector's; James et al., Am J Kidney Dis. 2015)
Setting-Specific and Exposure-Based Risk Factors
- Sepsis - the leading cause of AKI in the ICU; sepsis-associated AKI accounts for the majority of ICU AKI cases (multicenter AKI-EPI data)
- Cardiac surgery / cardiopulmonary bypass
- Major non-cardiac surgery
- Nephrotoxic drugs - aminoglycosides, NSAIDs, contrast media, cisplatin
- Volume depletion / haemorrhage
- Liver failure (hepatorenal syndrome)
- Immune checkpoint inhibitor therapy (emerging cause; ASCO/ASNO position statement 2025)
5. Special Populations
- Neonates: A 2024 meta-analysis in Pediatrics (PMID 38872621) found AKI is common in neonatal ICUs, especially in very preterm infants; incidence varies widely by definition used.
- ICU patients: A multinational ICU study (AKI-EPI) and Finnish FINNAKI study found AKI in 50-60% of ICU patients, with 90-day mortality exceeding 40% in severe stages.
- Cirrhosis: AKI (including hepatorenal syndrome) is extremely common in hospitalised cirrhotic patients, with significantly worse outcomes than AKI in other settings (Patidar et al., J Hepatol 2023).
- Older adults (>65 years): Carry disproportionate burden; incidence of dialysis-requiring ESKD in this group increased from 1,203 to 1,556 cases/million between 1996 and 2014.
6. Global Burden and Disparities
- The ISN Global Snapshot and other global initiatives highlight enormous geographic disparities in AKI detection and treatment access.
- High-income countries have better surveillance and KRT access; many AKI deaths in low- and middle-income countries go unrecorded due to absence of creatinine testing or dialysis services.
- The ISN set a goal to eliminate preventable deaths from AKI by 2025 - largely unmet due to infrastructure gaps in the developing world.
(Brenner and Rector's The Kidney, p. 862)
Summary Table
| Parameter | Estimate |
|---|---|
| Community incidence (general population) | 215-522 cases/100,000 person-years |
| Dialysis-requiring AKI (community) | 18-30 cases/100,000 person-years |
| Hospitalised patients with AKI (global) | ~25% |
| Of those, requiring KRT | ~10% |
| Post-cardiac surgery AKI | ~18.7% |
| AKI in ICU (critically ill) | 40-60% |
| CKD risk after KRT-requiring AKI | 2.8x higher |
| Excess cost per AKI episode (≥0.5 mg/dL rise) | ~$7,500 + 3.5 days LOS |
Source: Brenner and Rector's The Kidney, 2-Volume Set (9780323532655), Chapter 19, pp. 860-862. Recent PubMed evidence (2023-2026) from meta-analyses on neonatal AKI, sepsis-associated AKI in the ICU, and post-cardiac surgery AKI corroborates these figures without contradicting the textbook data.
I want short very short
Epidemiology of AKI
Incidence
- Community: ~215–522 cases/100,000 person-years
- Hospitalized patients: ~25% develop AKI (KDIGO criteria)
- ICU: 40–60%
- ~10% of hospitalized AKI cases require dialysis
Risk Factors
- Older age, male sex, diabetes, pre-existing CKD, albuminuria, sepsis, major surgery, nephrotoxins
Outcomes
- Survivors have 2.8x higher risk of CKD progression
- Even a 0.5 mg/dL creatinine rise = 3.5 extra hospital days + $7,500 excess cost
- Many KRT-requiring AKI patients never fully recover kidney function
Global burden
- Massive treatment gap in low-income countries; ISN goal to eliminate preventable AKI deaths by 2025 largely unmet
What about in context of nepal
Searching PubMed
"acute kidney injury" AND Nepal
Searching the Web
acute kidney injury epidemiology Nepal incidence causes
Reading Article
Reading Web Page
AKI epidemiology Nepal incidence causes mortality
AKI Epidemiology in Nepal
Incidence
- Non-ICU hospital admissions: ~15%
- ICU patients: up to 60%
- No national surveillance data exists; true burden is likely underestimated
Key Feature: Community-Acquired AKI Dominates
Unlike high-income countries where hospital-acquired AKI prevails, most AKI in Nepal is community-acquired - affecting younger, previously healthy individuals who present late with already advanced complications.
Main Causes (distinct from HIC pattern)
- Infections and sepsis (including tropical - malaria, dengue, leptospirosis)
- Diarrheal illness and severe dehydration
- Snakebite envenomation - especially in the Terai/southern lowlands; major cause of severe AKI requiring dialysis
- Obstetric complications - eclampsia, septic abortion
- Nephrotoxic traditional/herbal medicines (Ayurvedic preparations, including aristolochic acid)
- Acute post-streptococcal glomerulonephritis (children and adults)
- Chemical poisoning
South Asia Meta-Analysis context (Naqvi & Huma, JPMA 2023): Complete recovery across South Asian AKI studies ranged 40-80%; mortality ranged 2.2-52% - far higher than high-income countries, reflecting late presentation and limited resources.
System Barriers
- Dialysis access mainly in urban Kathmandu; nearly absent in rural areas
- Workforce shortage; patients often travel far to reach tertiary care
- No pharmacovigilance for nephrotoxic herbal remedies
- High out-of-pocket costs limit private care access
Bottom line: Nepal carries a high, largely preventable AKI burden driven by infections, toxins, and obstetric causes - most of which are addressable with basic public health interventions, early recognition, and improved rural access to KRT.
Can u add nepal context in epidemiology
Epidemiology of AKI
Incidence
| Setting | Global | Nepal |
|---|---|---|
| Community | 215–522/100,000 person-years | No national data |
| Hospitalized (non-ICU) | ~25% | ~15% |
| ICU | 40–60% | Up to 60% |
| Requiring dialysis | ~10% of hospital AKI | Limited access; underreported |
Community-Acquired vs. Hospital-Acquired
- Globally: ~2/3 community-acquired, 1/3 hospital-acquired
- Nepal: community-acquired AKI predominates - affects younger, previously healthy individuals who present late with advanced disease
Causes
- Global: sepsis, major surgery, nephrotoxic drugs, contrast, cardiac surgery
- Nepal (distinct pattern): infections/sepsis (malaria, dengue, leptospirosis), severe diarrheal dehydration, snakebite (Terai region), obstetric complications (eclampsia, septic abortion), nephrotoxic herbal/Ayurvedic medicines (aristolochic acid), post-streptococcal GN
Risk Factors
- Global: older age, male sex, diabetes, pre-existing CKD, albuminuria, low eGFR
- Nepal adds: rural residence, delayed presentation, poverty, use of traditional medicine, lack of early diagnostics
Outcomes
| Global | Nepal/South Asia | |
|---|---|---|
| Mortality | Low in HIC; 20–30% in ICU | 2.2–52% (South Asia meta-analysis) |
| Full recovery | Common with early treatment | 40–80% complete recovery |
| CKD progression | 2.8x higher after KRT-AKI | Higher due to late diagnosis |
System-Level Gaps (Nepal-specific)
- No national AKI surveillance - true burden underestimated
- Dialysis facilities concentrated in Kathmandu; nearly absent rurally
- Workforce shortage; long travel to tertiary care
- No pharmacovigilance for nephrotoxic herbal remedies
- High out-of-pocket costs
Bottom line: Nepal's AKI burden is driven largely by preventable, infectious, and environmental causes - a very different profile from high-income countries - compounded by late presentation and limited KRT access.
I liked the short version but i want u to add nepal context too
Epidemiology of AKI
Incidence
- Community: ~215–522 cases/100,000 person-years (Nepal: no national data; true burden underestimated)
- Hospitalized: ~25% globally; ~15% non-ICU in Nepal
- ICU: 40–60% globally and in Nepal
- ~10% require dialysis globally (Nepal: severely limited dialysis access outside Kathmandu)
Risk Factors
- Older age, male sex, diabetes, pre-existing CKD, albuminuria, sepsis, major surgery, nephrotoxins
- Nepal adds: rural residence, delayed presentation, use of nephrotoxic herbal/Ayurvedic medicines, poverty
Causes
- Globally: sepsis, surgery, contrast, drugs
- Nepal: infections (malaria, dengue, leptospirosis), diarrheal dehydration, snakebite (Terai region), obstetric complications (eclampsia, septic abortion), aristolochic acid herbal remedies, post-streptococcal GN
- Most AKI in Nepal is community-acquired (unlike HIC where hospital-acquired dominates)
Outcomes
- Survivors have 2.8x higher CKD progression risk; even small creatinine rises = 3.5 extra days + $7,500 cost
- Nepal/South Asia: mortality ranges 2.2–52% (vs. much lower in HIC); complete recovery only 40–80% — reflecting late presentation and limited KRT access
Global burden
- Massive treatment gap in LMICs; ISN goal to eliminate preventable AKI deaths by 2025 largely unmet
- Nepal: no national surveillance, dialysis concentrated in Kathmandu, high out-of-pocket costs — most preventable cases go unrecognized
This is a shared conversation. Sign in to Orris to start your own chat.