Make notes on heart failure with new guidelines and harrison but content should be in chronological way ( definition , etiology, risk factor pathophysiology, investigation , treatment and prevention),add relevent images, types of heart failure, classification of heart failure ,
Reading File
Finding Sources
Searching PubMed
"heart failure" AND "guidelines"
Searching the Web
2024 2025 ACC AHA ESC heart failure guidelines summary treatment classification
Reading File
Finding Sources
Searching PubMed
"heart failure" AND "treatment" AND "SGLT2"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading Web Page
https://www.jacc.org/doi/10.1016/j.jacc.2023.12.024
Loading Image
Finding Sources
Here are comprehensive, chronologically organized notes on Heart Failure, drawing from Robbins & Cotran Pathologic Basis of Disease, Braunwald's Heart Disease, Goldman-Cecil Medicine, and the 2022 AHA/ACC/HFSA + 2024 ACC Expert Consensus guidelines.
🫀 HEART FAILURE - Comprehensive Notes
1. DEFINITION
Heart failure (HF) is a clinical syndrome in which the heart is unable to provide adequate cardiac output to meet the metabolic demands of the body, or does so only at the cost of elevated filling pressures. It is characterized by:
- Inadequate perfusion of peripheral tissues (forward failure), AND
- Increased congestion of the venous circulation (backward failure)
"Heart failure occurs when the heart is unable to provide adequate perfusion to meet the metabolic requirements of peripheral tissues; inadequate cardiac output is usually accompanied by increased congestion of the venous circulation." - Robbins & Cotran Pathologic Basis of Disease
2. ETIOLOGY
Common Causes
| Category | Specific Conditions |
|---|---|
| Ischemic Heart Disease (most common) | Coronary artery disease, MI (acute and old), ischemic cardiomyopathy |
| Hypertension | Chronic pressure overload leading to LV hypertrophy and eventual failure |
| Valvular Heart Disease | Aortic stenosis/regurgitation, mitral regurgitation/stenosis |
| Primary Myocardial Disease | Dilated cardiomyopathy (DCM), hypertrophic cardiomyopathy (HCM), restrictive cardiomyopathy |
| Arrhythmias | Persistent tachyarrhythmias (tachycardia-induced cardiomyopathy), AF |
| Infection/Inflammation | Myocarditis (viral - Coxsackie B, Chagas disease, HIV) |
| Toxins/Drugs | Alcohol, anthracyclines (doxorubicin), trastuzumab, cocaine |
| Metabolic/Endocrine | Thyrotoxicosis, hypothyroidism, diabetes mellitus, acromegaly, Cushing's syndrome |
| Infiltrative disorders | Amyloidosis, sarcoidosis, hemochromatosis |
| Congenital | Congenital heart defects (late-onset) |
| High-output states | Anemia, AV fistula, beriberi (thiamine deficiency), Paget's disease |
| Familial | Familial dilated cardiomyopathy (genetic mutations in sarcomere/cytoskeletal proteins) |
3. RISK FACTORS
Non-modifiable
- Age (risk doubles each decade after 45)
- Male sex (earlier onset; women catch up post-menopause)
- Family history / genetic predisposition
Modifiable (Key targets for prevention)
- Hypertension - single largest risk factor; patients have 6-fold increased risk of HF
- Coronary artery disease / IHD
- Diabetes mellitus - independently increases HF risk
- Obesity (BMI >30) - associated with structural changes and HFpEF
- Smoking
- Physical inactivity / low cardiorespiratory fitness
- Dyslipidemia
- Sleep-disordered breathing (obstructive sleep apnea)
- Alcohol excess
- Prior chemotherapy / radiation exposure (cardiotoxicity)
- Atrial fibrillation - bidirectional relationship
4. PATHOPHYSIOLOGY
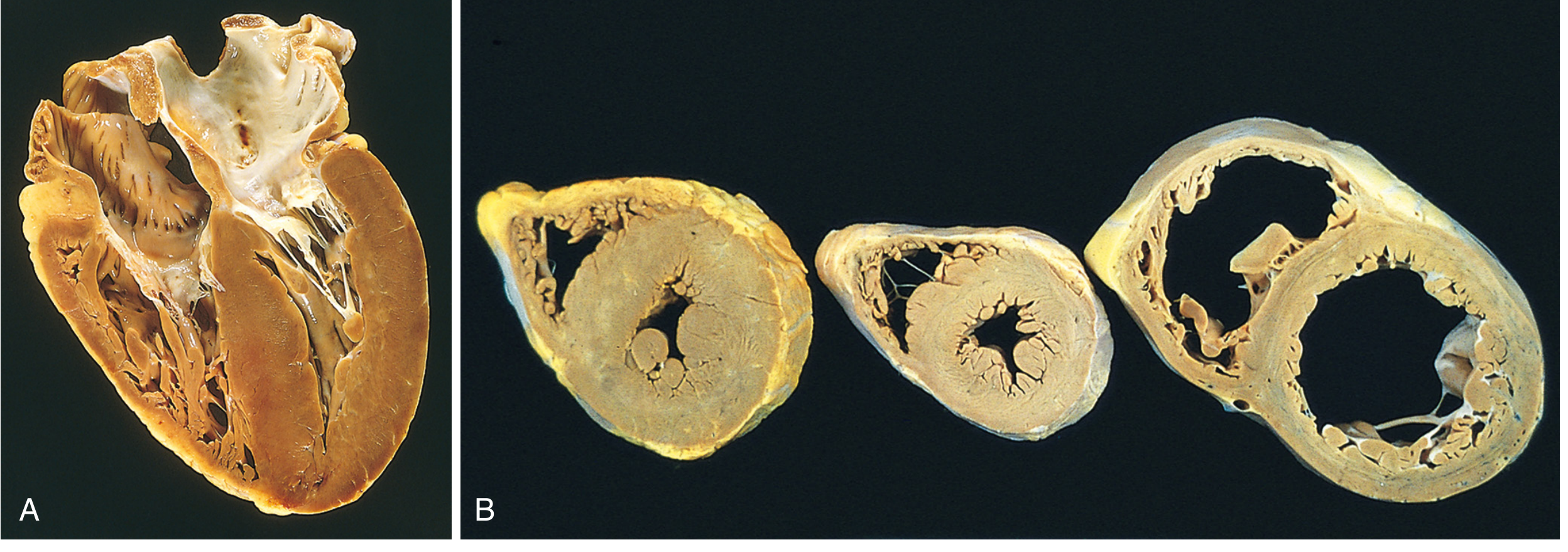
4a. Cardiac Hypertrophy - The Adaptive Response
A sustained increase in cardiac workload (pressure overload, volume overload, or neurohumoral signals) causes myocytes to hypertrophy:
Pressure overload (e.g., hypertension, aortic stenosis):
- New sarcomeres assembled in parallel to long axes
- Results in concentric hypertrophy - thickened wall, small cavity
Volume overload (e.g., valvular regurgitation):
- New sarcomeres assembled in series
- Results in eccentric hypertrophy - ventricular dilation
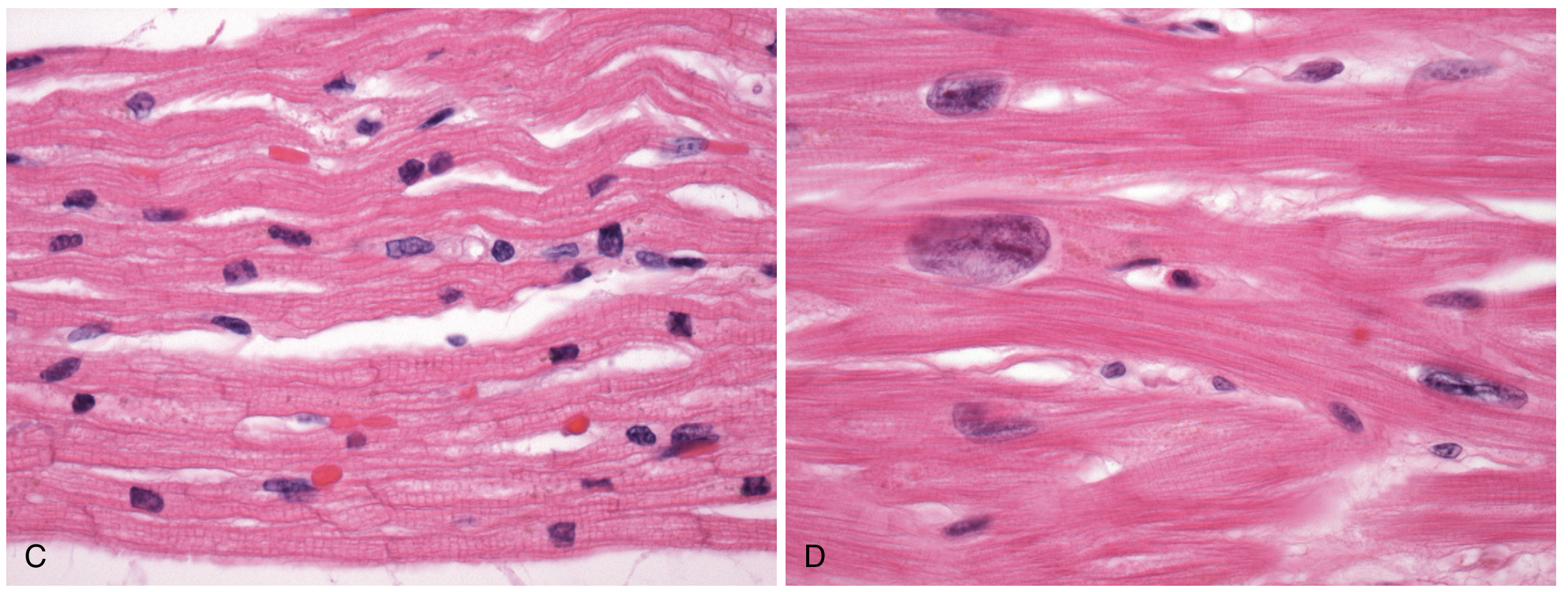
4b. Molecular/Cellular Changes with Hypertrophy
- Expression of immediate-early genes: FOS, JUN, MYC, EGR1 - stimulate cellular growth
- Re-expression of fetal gene program: fetal myosin isoforms, natriuretic peptides (ANP, BNP), collagen
- Interstitial fibrosis - myocardial fibroblasts increase ECM synthesis, increasing diastolic stiffness
- Inadequate capillary density - capillary proliferation does not keep pace with myocyte growth, creating relative ischemia
4c. Pathway to Failure
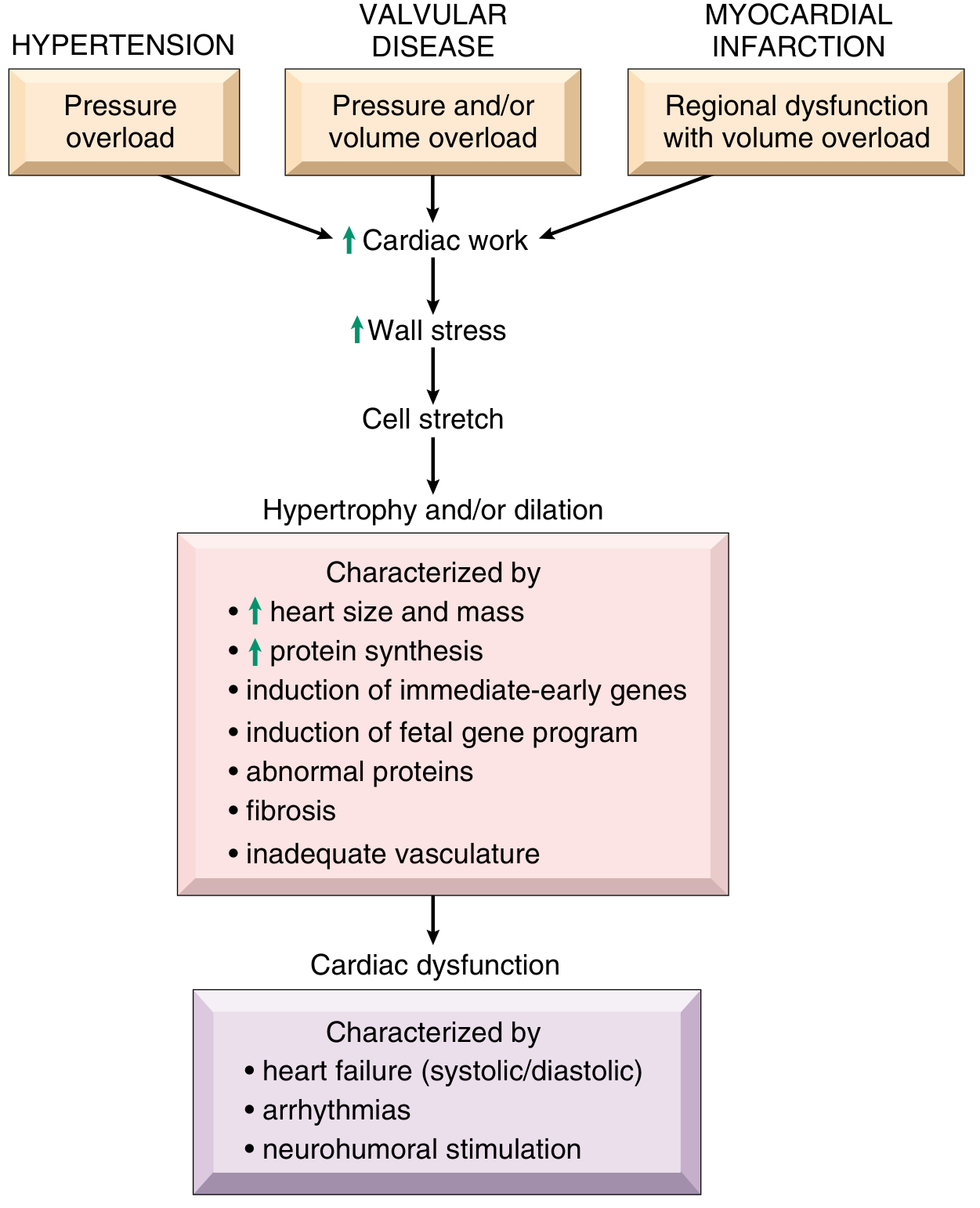
4d. Neurohumoral Activation
In moderate CHF, reduced EF → diminished renal perfusion → activation of RAAS (renin-angiotensin-aldosterone system):
- Salt and water retention
- Expansion of interstitial and intravascular fluid volumes
- Worsens pulmonary and peripheral edema
- Sympathetic nervous system activation: increases heart rate and contractility (short-term beneficial, long-term harmful - myocyte toxicity, remodeling)
If renal hypoperfusion is severe:
- Prerenal azotemia
- In far-advanced HF: hypoxic encephalopathy (irritability → stupor → coma)
4e. Left-Sided Heart Failure
Most commonly caused by: IHD, hypertension, aortic/mitral valve disease, primary myocardial disease
Morphology:
- LV usually hypertrophied and dilated
- LV dilation → papillary muscle displacement → functional mitral regurgitation
- LA dilation → risk of AF and left atrial thrombus
- Lungs: heavy and wet; hemosiderin-laden macrophages ("heart failure cells") in alveoli - pathognomonic of prior pulmonary edema episodes
- Pleural effusions (transudates)
Symptoms:
- Early: dyspnea on exertion, cough
- Progressive: orthopnea, paroxysmal nocturnal dyspnea (PND)
- Late: dyspnea at rest
Signs: Fine bibasal rales, S3 gallop (volume overload), S4 (increased stiffness), cardiomegaly, tachycardia
4f. Right-Sided Heart Failure
Most commonly caused by: Left-sided HF (most common), pulmonary HTN, cor pulmonale, RV MI, tricuspid/pulmonary valve disease
Morphology:
- RV hypertrophy and dilation
Clinical features:
- Peripheral edema (pedal, pretibial; sacral in bedridden)
- Hepatomegaly, hepatic congestion (cardiac cirrhosis if chronic)
- Ascites
- Elevated JVP
- Renal congestion (more pronounced azotemia than left HF)
5. TYPES OF HEART FAILURE
By Ejection Fraction (Primary Classification - 2022 AHA/ACC/HFSA)
| Type | LVEF | Key Feature |
|---|---|---|
| HFrEF - Heart Failure with Reduced EF | ≤40% | Systolic dysfunction; dilated LV; most evidence-based treatments available |
| HFmrEF - Heart Failure with Mildly Reduced EF | 41-49% | Intermediate phenotype; overlapping features; treatments extrapolated from HFrEF |
| HFpEF - Heart Failure with Preserved EF | ≥50% | Diastolic dysfunction; concentric LV; older, female, hypertensive, obese patients; 40-50% of all HF hospitalizations |
| HFimpEF - Heart Failure with Improved EF | Previously ≤40%, now improved >40% | EF has recovered (often after treating cause); ongoing monitoring required |
By Onset
| Type | Definition |
|---|---|
| Acute HF | New onset or rapid deterioration of signs/symptoms requiring urgent therapy |
| Chronic HF | Stable but persistent; may decompensate |
By Side of Heart
| Type | Key Features |
|---|---|
| Left-sided HF | Pulmonary congestion, dyspnea, orthopnea, PND |
| Right-sided HF | Systemic venous congestion, edema, hepatomegaly, ascites |
| Biventricular (Congestive HF) | Combined features of both; most common presentation in chronic disease |
By Mechanism
| Type | Mechanism |
|---|---|
| Systolic HF | Impaired LV contraction (reduced EF) |
| Diastolic HF | Impaired LV relaxation/filling (preserved EF) |
By Output State
| Type | Examples |
|---|---|
| Low-output HF | IHD, cardiomyopathy, valvular disease (most HF) |
| High-output HF | Severe anemia, thyrotoxicosis, AV fistula, beriberi |
6. CLASSIFICATION OF HEART FAILURE
6a. NYHA Functional Classification (Symptom-based, dynamic)
| Class | Description |
|---|---|
| Class I | No limitation of physical activity. Ordinary activity does NOT cause symptoms |
| Class II | Slight limitation. Comfortable at rest; ordinary activity causes fatigue, dyspnea, palpitation |
| Class III | Marked limitation. Comfortable at rest; less than ordinary activity causes symptoms |
| Class IV | Unable to perform ANY activity without symptoms; symptoms at rest |
6b. ACC/AHA Staging System (Structural/progressive, cannot regress)
| Stage | Description | Examples |
|---|---|---|
| Stage A | At risk for HF; NO structural heart disease or symptoms | Hypertension, DM, obesity, CAD, cardiotoxins - no cardiac structural changes yet |
| Stage B | Structural heart disease; NO current or previous symptoms | Asymptomatic LV dysfunction, prior MI, reduced LVEF, LV hypertrophy |
| Stage C | Structural heart disease WITH current or previous symptoms | Symptomatic HF - dyspnea, fatigue, edema |
| Stage D | Refractory/advanced HF; marked symptoms interfering with daily life; repeated hospitalizations despite optimal GDMT | Requires advanced therapies: LVAD, transplant, or palliative care |
Key distinction: NYHA class is reversible (patients can improve); AHA stages are permanent (cannot go backward from C to B).
7. CLINICAL FEATURES (Investigations)
History (Symptoms)
Left HF symptoms:
- Dyspnea on exertion (earliest)
- Orthopnea (requires ≥2 pillows to sleep)
- PND (awaking from sleep with breathlessness)
- Cough (often nocturnal, frothy sputum - pink if severe)
- Fatigue and weakness
Right HF symptoms:
- Ankle/leg swelling
- Abdominal bloating (ascites, hepatomegaly)
- Anorexia, nausea (hepatic/bowel congestion)
Both:
- Exercise intolerance, fatigue
- Weight gain (fluid retention)
Physical Examination Signs
| System | Finding |
|---|---|
| Vitals | Tachycardia, ± hypotension or elevated BP |
| JVP | Elevated (right HF), hepatojugular reflux |
| Chest | Bibasal fine inspiratory rales (crepitations), dullness at bases (pleural effusion) |
| Heart | Cardiomegaly, displaced apex, S3 gallop (volume overload), S4 (stiffness), murmurs |
| Abdomen | Hepatomegaly ± tenderness, ascites |
| Extremities | Pitting pedal/pretibial edema |
8. INVESTIGATIONS
8a. Biomarkers
B-type Natriuretic Peptide (BNP) / NT-proBNP - Class I Recommendation
Ventricular myocytes release BNP in response to increased wall stress/stretch. Used for:
- Diagnosis of acute dyspnea (HF vs non-cardiac cause)
- Assessing severity and prognosis
- Monitoring therapy response
| BNP Level | Interpretation |
|---|---|
| BNP <100 pg/mL or NT-proBNP <400 pg/mL | HF unlikely (high negative predictive value) |
| BNP 100-400 pg/mL or NT-proBNP 400-2000 pg/mL | Intermediate; specialist assessment within 6 weeks (NICE 2025) |
| BNP >400 pg/mL or NT-proBNP >2000 pg/mL | HF likely; urgent specialist assessment needed |
Note: BNP levels are reduced by obesity; elevated by advancing age, renal dysfunction, AF, PE, pulmonary HTN, and most HF therapies.
8b. ECG
- Identifies arrhythmia (AF, VT)
- Evidence of MI (Q waves), LVH, LBBB
- LBBB with QRS ≥150 ms: criteria for CRT consideration
8c. Chest X-Ray (CXR)
- Cardiomegaly (CTR >0.5)
- Pulmonary venous congestion (upper lobe diversion)
- Kerley B lines (interstitial edema)
- Bat-wing perihilar shadowing (alveolar edema)
- Pleural effusions
8d. Echocardiography (KEY INVESTIGATION - Class I)
The cornerstone investigation:
- LVEF - determines HFrEF vs HFpEF
- Wall motion abnormalities (IHD)
- Valvular function
- Diastolic parameters (E/A ratio, E/e' ratio)
- RV function, pulmonary artery pressure
- Pericardial effusion
- Mural thrombus detection
8e. Serum Laboratory Tests
- Full blood count (anemia)
- Renal function (eGFR, creatinine, electrolytes) - cardiorenal syndrome, drug monitoring
- LFTs (hepatic congestion)
- Thyroid function (thyrotoxicosis, hypothyroidism)
- Fasting glucose / HbA1c (DM comorbidity)
- Iron studies / ferritin - iron deficiency (affects ~50% of HFrEF patients)
- Lipid profile
8f. Advanced Investigations (Selected Patients)
| Test | Indication |
|---|---|
| Cardiac MRI | Myocarditis, amyloidosis, sarcoidosis, cardiomyopathy characterization |
| Coronary angiography / CT coronary | Rule out IHD as cause |
| Nuclear imaging (MUGA scan) | Accurate EF measurement; chemotherapy monitoring |
| Right heart catheterization | Pulmonary pressures, PCWP; advanced HF/transplant assessment |
| Endomyocardial biopsy | Suspected myocarditis, amyloidosis |
| Genetic testing | Familial cardiomyopathy |
| Sleep study | Suspected sleep apnea |
| 6-minute walk test / CPEX | Functional capacity, prognosis (VO2 max) |
9. TREATMENT
9a. General Principles
Treatment aims to:
- Relieve symptoms
- Reduce hospitalizations
- Reduce mortality
- Slow disease progression
Non-pharmacological measures:
- Salt restriction (<2-3 g/day sodium)
- Fluid restriction (1.5-2 L/day in severe HF)
- Daily weight monitoring (alert if >2 kg in 2 days)
- Smoking cessation
- Alcohol restriction (avoid in alcohol-related cardiomyopathy)
- Supervised aerobic exercise (cardiac rehabilitation - improves NYHA class, QoL, reduces hospitalizations)
- Vaccination (influenza, pneumococcus, COVID-19)
- Dietary: low-salt, plant-forward diet
9b. Pharmacological Treatment of HFrEF (LVEF ≤40%)
The "4 Pillars" of HFrEF Treatment (2022 AHA/ACC/HFSA + 2024 ACC ECDP - Class I, Level A)
All 4 should be initiated and up-titrated simultaneously (or in rapid sequence):
| Pillar | Drug Class | Key Examples | Key Benefit |
|---|---|---|---|
| 1. RAAS blockade | ACEi/ARB or ARNI | Enalapril, ramipril, valsartan; Sacubitril/valsartan (Entresto) | Reduces mortality ~15-25%; preferred: ARNI over ACEi |
| 2. Beta-blocker | Beta-blockers (carvedilol-class) | Carvedilol, metoprolol succinate, bisoprolol | Reduces mortality ~34%; reduces sudden cardiac death |
| 3. MRA | Mineralocorticoid receptor antagonist | Spironolactone, eplerenone | Reduces mortality ~25-30%; anti-fibrotic, anti-aldosterone |
| 4. SGLT2 inhibitor | SGLT2 inhibitor | Dapagliflozin, empagliflozin | Reduces HF hospitalizations + CV mortality regardless of diabetes status |
ARNI (Sacubitril/valsartan) is the preferred RAAS agent over ACEi/ARB alone (PARADIGM-HF trial). Never combine ARNI with an ACEi (36-hour washout required).
SGLT2 inhibitors (dapagliflozin/empagliflozin): Class I recommendation for HFrEF with or without type 2 diabetes. Mechanism: osmotic diuresis, natriuresis, reduced arterial stiffness, ketone-based metabolism shift. A 2024 Lancet meta-analysis (PMID: 38768620) confirmed benefit across the cardiometabolic spectrum.
Additional Pharmacotherapy
| Drug | Indication | Notes |
|---|---|---|
| Loop diuretics (furosemide, bumetanide) | Symptomatic fluid overload (all NYHA classes with congestion) | Relieve symptoms; no mortality benefit; titrate to euvolemia |
| Ivabradine | LVEF ≤35%, sinus rhythm, HR ≥70 bpm, on max beta-blocker | Reduces HF hospitalizations (SHIFT trial) - Class IIa |
| Hydralazine + Isosorbide dinitrate | HFrEF in Black patients OR intolerant of ACEi/ARB/ARNI | A-HeFT trial; reduces mortality in self-identified Black patients |
| Digoxin | Symptomatic HFrEF in sinus rhythm (add-on); reduces hospitalization; rate control in AF | No mortality benefit; narrow therapeutic window |
| Vericiguat | Worsening HFrEF on max GDMT; LVEF <45% | Soluble guanylate cyclase stimulator; VICTORIA trial |
9c. Treatment of HFpEF (LVEF ≥50%)
- Fewer proven disease-modifying treatments than HFrEF
- SGLT2 inhibitors (empagliflozin, dapagliflozin): now recommended - reduce HF hospitalizations; Class IIa/IIb
- MRAs (spironolactone): modest benefit in TOPCAT trial (post-hoc benefit in Americas subgroup)
- Treat underlying causes: BP control (target <130/80), AF rate/rhythm control, coronary revascularization if ischemia
- Loop diuretics for symptom relief of congestion
- Manage comorbidities: obesity, diabetes, sleep apnea, AF, iron deficiency
9d. Device Therapy
| Device | Indication |
|---|---|
| ICD (Implantable Cardioverter Defibrillator) | LVEF ≤35% despite optimal GDMT for ≥3 months; NYHA II-III; expected survival >1 year - primary prevention of SCD |
| CRT (Cardiac Resynchronization Therapy) | LVEF ≤35%, LBBB with QRS ≥150 ms (strongest indication); NYHA II-IV; sinus rhythm |
| CRT-D | Combined ICD + CRT in eligible patients |
| LVAD (Left Ventricular Assist Device) | Stage D HF; bridge to transplant or destination therapy |
9e. Advanced Heart Failure (Stage D) Therapies
- Heart transplantation: gold standard for end-stage HF; improves survival to ~50% at 10 years
- LVAD as destination therapy: for transplant-ineligible patients; HeartMate 3 trial
- Intra-aortic balloon pump (IABP): temporary mechanical support in cardiogenic shock
- Palliative/supportive care: symptom management, hospice consideration
9f. Treatment of Acute Decompensated Heart Failure (ADHF)
LMNOP - a useful mnemonic for acute management:
- L - Lasix (furosemide IV diuresis - cornerstone of acute treatment)
- M - Morphine (if severe anxiety/dyspnea - use with caution)
- N - Nitrates (sublingual/IV nitroglycerin - afterload reduction, symptom relief)
- O - Oxygen (if SpO2 <94%; avoid in normoxic patients)
- P - Positioning (sit upright; legs dependent)
Additional:
- Monitor fluid balance closely
- Continue oral GDMT if tolerated; titrate cautiously
- Treat precipitants: arrhythmia, infection, medication non-compliance, ACS
- Consider IV inotropes (dobutamine, milrinone) in cardiogenic shock
- NIV (CPAP/BiPAP) for respiratory distress
10. PREVENTION
Primary Prevention (Stage A - At-Risk Patients)
- Control hypertension aggressively (target <130/80 mmHg) - most impactful single intervention
- Treat diabetes - SGLT2 inhibitors and GLP-1 agonists reduce HF risk in diabetics
- Statin therapy in high-CV risk patients - reduces atherosclerotic burden
- Smoking cessation
- Regular aerobic exercise - reduces HF incidence by improving CRF; aerobic hypertrophy is beneficial (increases capillary density unlike pathologic hypertrophy)
- Weight management (BMI <25)
- Limit alcohol (<14 units/week)
- Cardioprotective strategies in chemotherapy patients (baseline echo, early cardiology referral)
Secondary Prevention (Stage B - Asymptomatic LV Dysfunction)
- ACEi/ARB in asymptomatic LV dysfunction (EF ≤35%): SOLVD Prevention trial showed reduction in HF development
- Beta-blockers post-MI with reduced EF
- Statins post-MI
- ICD consideration if EF ≤35% and not responding to medical therapy
Tertiary Prevention (Stage C/D)
- Maximize GDMT adherence
- Multidisciplinary HF team approach
- Regular monitoring (echo, BNP, renal function)
- Patient education and self-monitoring
- Cardiac rehabilitation programs
11. PROGNOSIS
- 5-year mortality approximately 50% (similar to many cancers)
- Annual mortality in NYHA Class IV: ~50-75% without advanced therapies
- Major killers: sudden cardiac death (SCD) and progressive pump failure
- Improved prognosis with: full GDMT implementation, ICD/CRT, optimal comorbidity management
Quick Reference: Summary of Key Treatment Recommendations (2022 AHA/ACC/HFSA + 2024 ACC ECDP)
| Recommendation | Class | Level |
|---|---|---|
| 4 Pillars (ARNI + BB + MRA + SGLT2i) for HFrEF | I | A |
| BNP/NT-proBNP measurement for HF diagnosis | I | A |
| Echocardiography for all patients | I | C |
| ICD for LVEF ≤35%, NYHA II-III, on GDMT ≥3 months | I | A |
| CRT for LVEF ≤35%, LBBB, QRS ≥150 ms | I | A |
| SGLT2i for HFpEF (empagliflozin/dapagliflozin) | IIa/IIb | B |
| Ivabradine for HR ≥70, LVEF ≤35%, max beta-blocker | IIa | B |
| IV iron replacement in iron-deficient HFrEF | IIa | B |
Sources consulted:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (Chapter 12)
- Braunwald's Heart Disease - 2 Vol Set, 12th Edition
- Goldman-Cecil Medicine International Edition
- 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure
- 2024 ACC Expert Consensus Decision Pathway (J Am Coll Cardiol 2024)
- NICE 2025 HFrEF Guideline update
- SGLT2 inhibitor meta-analysis - Lancet 2024 (PMID: 38768620)
This is a shared conversation. Sign in to Orris to start your own chat.