causes of rashes in the trunk and abdomen in 11 month old female baby
Reading File
Finding Sources
Finding Sources
Searching the Web
causes of trunk abdomen rash 11 month old infant differential diagnosis
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
I now have everything needed for a thorough, well-illustrated response. Here is the full answer:
Causes of Trunk/Abdomen Rash in an 11-Month-Old Female
At 11 months, an infant is in a high-risk window for several classic infectious exanthems, inflammatory conditions, and infestations. Below is a structured differential diagnosis organized by category.
1. Roseola Infantum (Exanthem Subitum / Sixth Disease) - Most likely at this age
The single most common cause of trunk-predominant rash at this exact age group (6 months to 3 years, 95% of cases).
Cause: Human Herpesvirus 6 (HHV-6), occasionally HHV-7. Spread by saliva.
Classic pattern:
- 3-4 days of HIGH fever (39-41°C), abrupt onset; infant appears surprisingly well despite the fever
- Fever breaks - rash appears (hallmark: rash after defervescence, not during fever)
- Discrete pink/rose-colored macules or maculopapules, 2-3 mm, blanch on pressure, rarely coalesce
- Starts on trunk, spreads to neck and extremities; face usually spared
- Rash lasts 3-5 days, then resolves spontaneously
- May have "Nagayama spots" (erythematous papules on soft palate) before rash
Complications: Febrile seizures (common); encephalitis (very rare). Prognosis is excellent; no treatment needed.
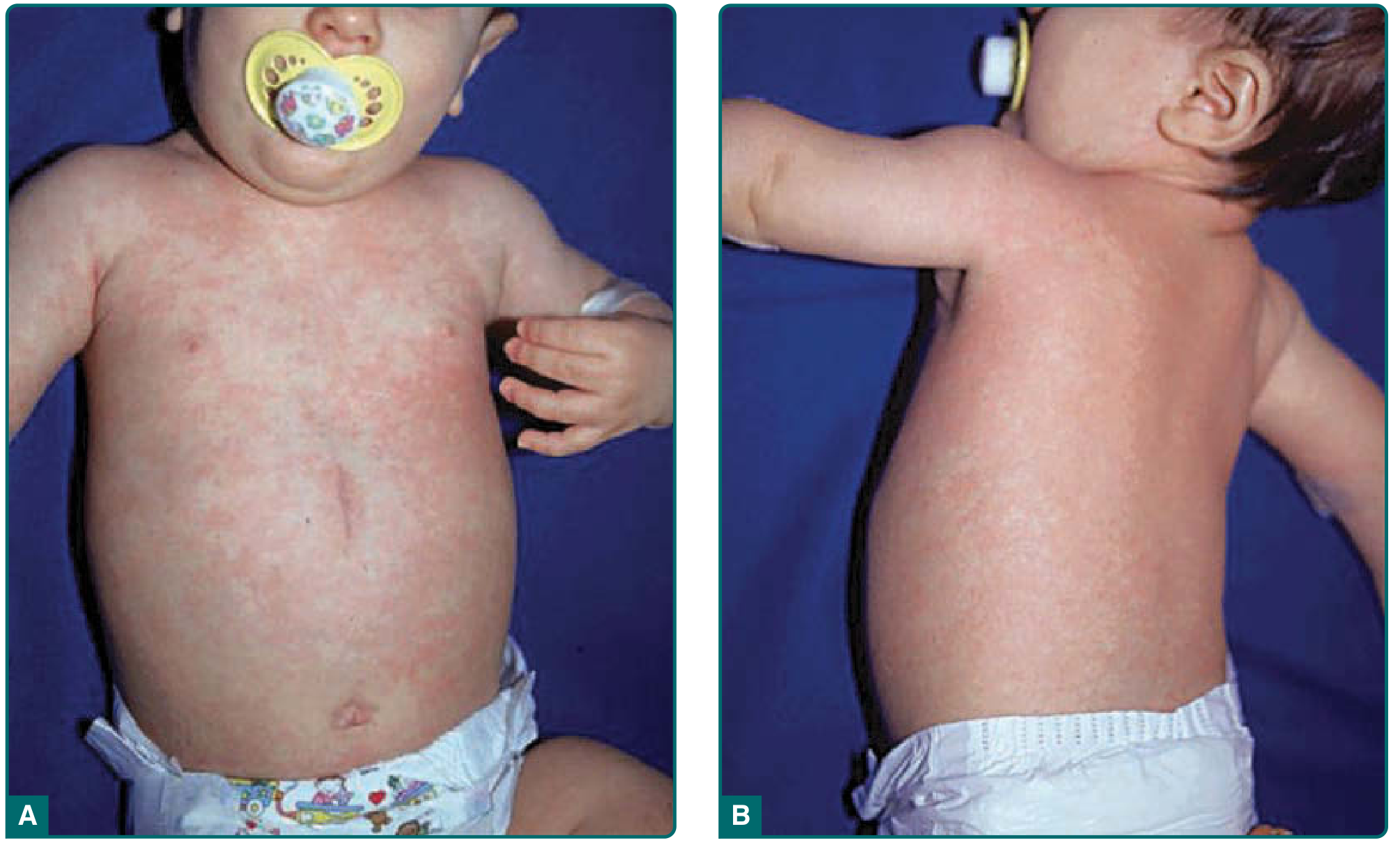
Roseola: truncal pink macules appearing 1 day after fever breaks. - Fitzpatrick's Dermatology

2. Viral Exanthems (Enteroviral / Echovirus / Coxsackievirus)
Cause: ~30 enteroviruses (coxsackievirus, echovirus) and adenoviruses account for ~72% of fever + rash in pediatric patients.
Features:
- Maculopapular rash, usually nonpruritic, does not desquamate
- Variable in extent; eruption typically starts on trunk
- May be accompanied by oropharyngeal lesions
- Concurrent fever; infant may be irritable
3. Measles (Rubeola)
Cause: Measles virus; highly contagious; risk in unvaccinated infants.
Features:
- Prodrome: fever + "3 C's" - cough, coryza, conjunctivitis
- Koplik spots (bluish-white spots on buccal mucosa) - pathognomonic, appear day 2
- Rash starts on forehead/upper neck, spreads to face, trunk, arms, legs (head-to-toe pattern)
- Maculopapular, erythematous; fades in same order it appeared
- More severe in malnourished or immunocompromised infants
4. Rubella (German Measles)
Cause: Rubella virus; spread by droplets.
Features:
- Pink to red maculopapules begin on face, spread rapidly to neck, trunk, and extremities
- Trunk lesions may coalesce; extremity lesions typically don't
- Generalized lymphadenopathy (especially suboccipital, postauricular)
- Rash lasts 1-5 days
- Rare in vaccinated populations
5. Erythema Infectiosum (Fifth Disease / Parvovirus B19)
Features:
- Classic "slapped cheek" appearance on face
- Lacy, reticular rash spreads to trunk and proximal extremities
- Can wax and wane with temperature changes, exercise, or sun exposure
- Usually benign; mild or absent systemic symptoms in this age group
6. Atopic Dermatitis (Infantile Eczema)
Features:
- In infants under 2 years: intensely itchy papules and vesicles with serous exudate/crusts
- Poorly defined erythema; involves face, trunk, extensor limb surfaces, and sometimes the diaper area
- Dry skin, excoriation marks from scratching
- Family history of atopy (asthma, hay fever, eczema)
- Chronic/relapsing course
7. Seborrheic Dermatitis (Infantile)
Features:
- Greasy, yellowish, scaly patches
- Begins on scalp (cradle cap), may spread to face, neck, trunk, and flexural areas
- Usually non-itchy (distinguishes it from atopic dermatitis)
- Common in first few months of life but can persist to 12 months
- Self-limiting
8. Miliaria (Heat Rash / Prickly Heat)
Cause: Blocked eccrine sweat ducts; common in hot/humid environments or overdressing.
Features:
- Groups of erythematous papules and pustules over the face, upper trunk, and skin folds
- Miliaria rubra ("prickly heat") - red, prickly-feeling bumps
- Resolves quickly when infant is cooled and overdressing corrected
Textbook of Family Medicine 9e
9. Scabies
Cause: Sarcoptes scabiei mite infestation.
Features:
- Intensely pruritic (worse at night)
- In infants: involves the trunk, abdomen, palms, soles, and face (distribution differs from adults)
- Burrows, papules, vesicles, and secondary excoriation/impetiginization
- Often affects multiple household members
10. Urticaria (Hives)
Cause: Allergic reaction (food, medications, infection, insect bite).
Features:
- Raised, itchy, pale/red wheals that come and go
- Commonly on chest, abdomen, back, throat, and limbs
- Each lesion resolves within 24 hours but new ones appear
- If accompanied by lip/tongue swelling, vomiting, or breathing difficulty - anaphylaxis emergency
11. Tinea Corporis (Ringworm)
Features:
- Sharply marginated, annular lesion with raised edges and central clearing
- Can appear on the trunk or abdomen
- Slightly scaly border
- Diagnosis confirmed by KOH preparation showing branching hyphae
12. Impetigo
Cause: Staphylococcus aureus or Group A Streptococcus.
Features:
- Honey-colored crusted lesions or fluid-filled blisters (bullous impetigo)
- Can occur on trunk; spreads easily with contact
- Contagious; requires antibiotic treatment
- Note: NHS guidance recommends GP assessment for impetigo in infants aged 11 months or younger
13. Neonatal/Infantile Lupus (Neonatal Lupus Erythematosus)
Features:
- Caused by transplacental transfer of maternal anti-Ro/SSA antibodies
- Nonscarring, large, circular macules over face, trunk, and extremities
- Rash is photosensitive; typically resolves by 6-12 months as maternal antibodies clear
- May be associated with congenital heart block (rare but serious)
Rheumatology 2-Volume Set (Elsevier, 2022)
Red Flag Signs Requiring Urgent Evaluation
| Sign | Concern |
|---|---|
| Non-blanching petechiae/purpura | Meningococcemia, ITP, vasculitis |
| High fever + toxic-appearing infant | Sepsis, meningococcemia |
| Rash + difficulty breathing/wheezing | Anaphylaxis |
| Rash + stiff neck, photophobia | Meningitis |
| Blistering/peeling skin | Staphylococcal scalded skin syndrome |
| Rash + joint swelling | Septic arthritis, reactive arthritis |
Quick Summary Table
| Condition | Fever | Rash Type | Trunk Pattern | Key Clue |
|---|---|---|---|---|
| Roseola | High, then resolves | Pink macules/papules | Starts trunk, spreads out | Rash AFTER fever breaks |
| Measles | High | Maculopapular | Head-to-toe spread | Koplik spots, 3 C's |
| Rubella | Low-grade | Pink maculopapules | Face → trunk → limbs | Lymphadenopathy |
| Fifth disease | Absent/mild | Lacy reticular | Trunk + limbs | "Slapped cheek" face |
| Enterovirus | Variable | Maculopapular | Trunk-predominant | Oral ulcers possible |
| Atopic eczema | No | Itchy papules/vesicles | Face + trunk + extensors | Dry skin, family atopy |
| Seborrheic derm. | No | Greasy yellow scales | Trunk + scalp | Cradle cap, non-itchy |
| Miliaria | May be present | Red papules/pustules | Upper trunk, folds | Heat exposure |
| Scabies | No | Itchy papules/burrows | Trunk + palms/soles | Night itch, family members |
| Urticaria | Variable | Wheals | Chest/abdomen/back | Comes and goes |
| Impetigo | Possible | Honey crust/blisters | Any area | Contagious, spreads |
At 11 months, Roseola Infantum is by far the most probable diagnosis if the rash follows a febrile episode, is trunk-predominant, blanching, and the infant appears otherwise well. Always assess vaccination history, fever pattern, associated symptoms (cough, coryza, Koplik spots), and family/contact history to narrow the differential further. Non-blanching rashes require same-day urgent evaluation.
vitamin a administration causes rashes in abdomen
Reading File
Finding Sources
Finding Sources
Searching the Web
vitamin A toxicity hypervitaminosis A skin rash abdomen infant symptoms
Reading File
Reading File
I have solid textbook and web evidence. Here is the complete answer:
Vitamin A Toxicity and Skin Rash
Yes - Vitamin A toxicity (hypervitaminosis A) does cause skin rashes, and abdominal pain is also a recognized feature. However, the rash from Vitamin A excess is not specifically localized to the abdomen - it is typically generalized. This is an important distinction.
The Skin Manifestations of Vitamin A Toxicity
Acute Toxicity (Subacute)
When a large dose of Vitamin A is ingested over a short period, the classic triad is:
- Red, peeling rash (desquamation/peeling)
- Headache
- Vomiting
The skin peels diffusely, not just on the abdomen.
Chronic Toxicity
From repeated excess dosing over time, skin changes include:
- Dry, rough skin (xerosis)
- Pruritus (itching)
- Scaly dermatitis (eczema-like scaling)
- Abnormal skin pigmentation
- Hair loss (alopecia), especially of the eyebrows
- Cracked lips and corners of the mouth
- Increased sensitivity to sunlight
- Jaundice (with hepatotoxicity)
Tintinalli's Emergency Medicine; Ganong's Review of Medical Physiology, 26th Ed.
Why the Abdomen May Seem Involved
Vitamin A toxicity does cause abdominal pain as a separate symptom from the rash. When a parent or caregiver notices a rash on the trunk/abdomen AND the infant has abdominal discomfort after Vitamin A supplementation, these are two different effects occurring together:
| Symptom | Cause |
|---|---|
| Abdominal pain | Direct GI irritation from excess retinol |
| Rash (peeling/scaling) | Systemic retinoid effect on epithelial cells |
| Headache / bulging fontanelle | Raised intracranial pressure |
| Vomiting | GI/CNS effects |
Specific Infant Vulnerability
Infants and children are far more sensitive to Vitamin A toxicity than adults:
- The toxic threshold for children is as low as 20,000 IU/day (vs. 100,000+ IU/day in adults)
- Swallowing even small amounts of retinol-containing skin cream can cause poisoning in infants
- Infant-specific signs include:
- Bulging anterior fontanelle (raised intracranial pressure - key sign in infants)
- Irritability and drowsiness
- Failure to gain weight
- Soft skull bone (craniotabes)
- Double vision or bulging eyeballs (with severe toxicity)
MedlinePlus / MSD Manual Professional Edition
Context: Vitamin A in Measles Treatment
In the previous question, Vitamin A was mentioned in the context of measles treatment. This is a WHO/AAP-recommended therapeutic use (not supplementation). When given at therapeutic doses for measles (100,000-200,000 IU as a one or two-dose regimen), side effects are uncommon. However, the peeling rash is occasionally seen as a transient effect even at these doses, especially if repeated.
Key Points
- Yes, Vitamin A toxicity causes skin rash - typically red, peeling, and generalized (not limited to the abdomen).
- Abdominal pain is a separate concurrent symptom of Vitamin A toxicity, not caused by the rash.
- In an 11-month-old, any excess Vitamin A is concerning - even modest overdosing causes toxicity faster than in adults.
- A bulging fontanelle after Vitamin A supplementation in an infant is a red flag and requires urgent evaluation.
- Treatment is simple: stop Vitamin A intake. Most symptoms resolve within 1-4 weeks of stopping.
Important: If an infant has received a Vitamin A supplement and develops a rash with vomiting, fontanelle bulging, or extreme irritability, this should be evaluated by a doctor promptly as it may indicate acute hypervitaminosis A.
vitamin A dosage in 9 month baby
Finding Sources
Finding Sources
Searching the Web
vitamin A recommended dosage 9 month old infant WHO guidelines supplementation
Finding Sources
Finding Sources
Reading File
Searching the Web
vitamin A dose 9 month old baby RDA upper limit IAP India measles supplementation
Excellent - comprehensive data from WHO, NIH, and clinical guidelines. Here is the full answer:
Vitamin A Dosage in a 9-Month-Old Baby
A 9-month-old infant falls in the 6-11 months age bracket. There are two distinct contexts for Vitamin A dosage: daily dietary requirements vs. therapeutic/preventive supplementation.
1. Daily Dietary Requirement (RDA / AI)
| Authority | Age | Dose |
|---|---|---|
| US Institute of Medicine (IOM) | 7-12 months | 500 mcg RAE/day (≈ 1,667 IU/day) |
| Tolerable Upper Intake Level (UL) | 7-12 months | 600 mcg RAE/day (≈ 2,000 IU/day) |
| Australia (NHMRC) | 7-12 months | 430 mcg retinol equivalents/day |
- RAE = Retinol Activity Equivalent
- This is the amount needed from breast milk, formula, and complementary foods combined
- Most healthy infants on breast milk or formula meet this requirement without supplements
2. WHO Preventive Supplementation (High-Dose, for Vitamin A Deficiency-Endemic Areas)
In countries where Vitamin A Deficiency (VAD) is a public health problem (common in South Asia, Sub-Saharan Africa), the WHO recommends:
| Age Group | Dose | Frequency |
|---|---|---|
| 6-11 months (includes 9 months) | 100,000 IU | Once (single dose) |
| 12-59 months | 200,000 IU | Every 4-6 months |
- Given as oral liquid (oil-based retinyl palmitate or retinyl acetate)
- Often co-administered with the measles vaccine at 9 months under the Expanded Programme on Immunization (EPI)
- This single 100,000 IU dose provides adequate liver stores for ~4-6 months
3. Therapeutic Dose - Measles Treatment (WHO / AAP)
If the 9-month-old has measles, Vitamin A is given therapeutically:
| Age | Dose | Duration |
|---|---|---|
| 6-11 months | 100,000 IU/day orally | 2 consecutive days |
| < 6 months | 50,000 IU/day | 2 days |
| ≥ 12 months | 200,000 IU/day | 2 days |
- An additional 3rd dose is given 2-4 weeks later if the child shows signs of Vitamin A deficiency (Bitot's spots, xerophthalmia) or eye complications.
- These high therapeutic doses have been shown to reduce measles mortality by up to 82% in children under 2 years and pneumonia-specific mortality by 67%.
WHO guidelines; NFID Call-to-Action 2023; Medscape Measles Treatment
4. Safety Margins - Why the Dose Seems High
The single 100,000 IU preventive dose and the 2-day 100,000 IU therapeutic dose are well-established and safe because:
- Vitamin A is stored in the liver and released slowly over months
- Side effects at these doses (headache, nausea, vomiting, diarrhea) are transient and mild, occurring in only 3-7% of children and resolving within 24 hours
- Studies have reported even 400,000 IU to be relatively safe as a single dose
- No deaths have been attributed solely to Vitamin A toxicity at WHO-recommended supplementation doses
However, repeated high doses over time accumulate and can cause toxicity (as discussed earlier - bulging fontanelle, peeling rash, liver damage).
Quick Reference Summary
| Purpose | Dose for 9-month-old | Notes |
|---|---|---|
| Daily dietary need | 500 mcg RAE (~1,667 IU)/day | From food/formula; rarely needs supplementation |
| Preventive supplementation (VAD-endemic) | 100,000 IU once | Co-administered with 9-month measles vaccine |
| Measles treatment | 100,000 IU/day × 2 days | Give even in non-deficient areas |
| Toxic threshold (chronic) | >20,000 IU/day continuously | Avoid exceeding; monitor for fontanelle bulging |
Clinical note: In India and most developing countries, the 100,000 IU single-dose Vitamin A is routinely given at 9 months alongside the measles vaccine as part of the National Immunization Schedule, and again at 16-18 months (200,000 IU). This is a safe, evidence-based public health intervention - not a cause for concern when given at the correct age-appropriate dose.
This is a shared conversation. Sign in to Orris to start your own chat.