Congenital vertical talus 15 marks ms ortho
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive 15-mark MS Ortho answer. Here it is:
Congenital Vertical Talus (CVT) — 15 Marks (MS Ortho)
Definition
Congenital Vertical Talus (CVT), also called congenital convex pes valgus or rocker-bottom foot, is a rigid flatfoot deformity characterized by an irreducible dorsal dislocation of the navicular on the talus, with the talus pointing nearly vertical (almost parallel to the tibia). It must be distinguished from the flexible pes planus commonly seen in infants.
Incidence & Associations
- Rare deformity; may be unilateral or bilateral
- 50% are associated with neuromuscular/syndromic conditions:
- Myelomeningocele
- Arthrogryposis multiplex congenita
- Prune-belly syndrome
- Spinal muscular atrophy
- Neurofibromatosis
- Trisomies (13, 18)
- The remaining ~50% are idiopathic (isolated)
- A less severe form, oblique talus, exists - in this variant the navicular reduces with plantar flexion (treated conservatively)
Pathoanatomy
The deformity involves three key components:
| Component | Deformity |
|---|---|
| Hindfoot | Equinovalgus (talus nearly vertical, calcaneus in equinus) |
| Midfoot | Talonavicular dislocation - navicular displaced dorsally on talar head |
| Forefoot | Abducted and dorsiflexed at midtarsal joints |
Secondary adaptive changes (with weight-bearing):
- Talus becomes hourglass-shaped; its longitudinal axis approximates the tibial axis
- Only the posterior third of talar dome articulates with the tibia
- Calcaneus displaced posteriorly; rounded anterior plantar surface develops
- Callosities form under the anterior calcaneus and over the talar head medially
- Forefoot becomes severely abducted; heel does not touch ground
- Dorsal capsules, ligaments, and tendons become contracted
- Posterior tibial tendon and peroneal tendons may migrate anterior to the malleoli, acting as dorsiflexors rather than plantarflexors - this is a key secondary pathology
Clinical Features

Bilateral CVT in a 14-month-old child - note the classic rocker-bottom (convex sole), talar head prominence medially, and equinovalgus hindfoot. (Campbell's Operative Orthopaedics, 15th Ed)
- Rocker-bottom foot (Persian slipper/convex sole) - pathognomonic
- Prominent medial/plantar talar head - visible and palpable bulge
- Fixed equinovalgus hindfoot - cannot be corrected passively
- Abducted and dorsiflexed forefoot
- Deep dorsolateral skin creases anterior and inferior to the lateral malleolus
- Peg-leg gait - awkward gait with limited forefoot push-off (in ambulatory children)
- RIGIDITY - the deformity is non-reducible (distinguishes from flexible flatfoot)
Radiographic Findings
Lateral Radiograph (Weight-bearing + Forced Plantar-flexion views)
| Finding | Description |
|---|---|
| Talus | Nearly vertical - longitudinal axis almost parallel to tibia |
| Calcaneus | Equinus position |
| Navicular | Dorsally dislocated on talar head (not ossified in children <3 years) |
| Talocalcaneal angle | Increased (normal 20-40°) |
| Talo-first metatarsal angle | Reversed - talus points down while forefoot dorsiflexes |
Key diagnostic radiograph: Forced plantar-flexion lateral view
- In CVT: navicular does NOT reduce; the talus-first metatarsal alignment is NOT restored by plantarflexing the forefoot
- In flexible pes planus / calcaneovalgus foot: alignment IS restored on forced plantar-flexion
- In children <3 years, the navicular is unossified - its position is inferred from the medial cuneiform and first metatarsal alignment
AP Radiograph
- Increased talocalcaneal angle (>40°)
- Talonavicular divergence
Differential Diagnosis
| Condition | Key Distinction |
|---|---|
| Flexible pes planus | Reducible; plantar-flexion radiograph normalizes |
| Calcaneovalgus foot | Dorsiflexed hindfoot (calcaneus), not equinus |
| Oblique talus | Partial reducibility on plantar-flexion view |
| Tarsal coalition | Older age, peroneal spasm, X-ray/CT coalition |
Note: In calcaneovalgus foot, the hindfoot is in calcaneus (dorsiflexed); in CVT, hindfoot is in equinus (plantar-flexed) - an important distinction.
Treatment
CVT is difficult to correct and tends to recur. Treatment is based on age and severity.
Conservative Phase (All Ages - Initial Treatment)
Serial Manipulation and Casting (Dobbs Technique / Reverse Ponseti)
- Serial outpatient casting with the forefoot progressively plantarflexed (opposite direction to Ponseti for clubfoot)
- Achieves relaxation of dorsolateral structures
- Achieves partial or complete reduction of the talonavicular joint
- Typically 4-6 casts over several weeks
Surgical Treatment (Definitive)
Once casting has been performed, limited percutaneous surgery is done:
Step 1: Percutaneous retrograde pinning of the talonavicular joint (K-wire)
Step 2: Percutaneous Achilles tenotomy to achieve ankle dorsiflexion and eliminate the equinus component
This minimally invasive approach (Dobbs method) has shown excellent results and has become the standard initial surgical option for most patients.
Age-Based Surgical Protocol (for persistent/recurrent deformity):
| Age | Recommended Surgery |
|---|---|
| 1-4 years | Open reduction and realignment of talonavicular + subtalar joints (Kumar-Cowell-Ramsey technique) |
| 3+ years, severe | Open reduction + navicular excision if needed |
| 4-8 years | Open reduction + soft-tissue procedures + extra-articular subtalar arthrodesis |
| >12 years | Triple arthrodesis (talocalcaneonavicular + calcaneocuboid) for permanent correction |
Open Reduction Technique (Kumar, Cowell & Ramsey)
Three-incision approach (or preferred Cincinnati/transverse circumferential approach):
- Lateral incision over sinus tarsi - release calcaneocuboid ligament; reflect extensor digitorum brevis
- Medial incision over talar head - expose head of talus and navicular
- Posterior incision medial to Achilles - Z-plasty lengthening of Achilles tendon; posterior capsulotomy if needed
Releases performed:
- Dorsal talonavicular ligament
- Plantar calcaneonavicular (spring) ligament
- Anterior superficial deltoid ligament
- Talocalcaneal interosseous ligament (partial)
- Z-plasty lengthening of contracted tendons: anterior tibialis, EHL, EDL, peroneals
Fixation:
- K-wire from navicular into talar neck (or posterior to anterior) to maintain talonavicular reduction
- Confirm reduction with intraoperative AP and lateral radiographs
Reconstruction:
- Repair talonavicular ligament
- Anterior tibialis tendon transfer to plantar aspect of talonavicular joint capsule (preferred by many - prevents recurrence)
- Cast immobilization post-operatively
Single-Stage K-Wire Joystick Technique (Dobbs)
- Threaded K-wire placed axially through the vertical talus from posterior acting as a "joystick"
- Talus manipulated into reduced position
- Wire advanced across talonavicular and subtalar joints to hold correction
- Percutaneous Achilles tenotomy completes the procedure
Complications
- Recurrence - most common complication; requires repeat casting or surgery
- Avascular necrosis of the talar head
- Wound breakdown (extensive soft tissue dissection)
- Stiffness / residual deformity
- Pin tract infection
Key Points for Exam (MS Ortho)
- CVT = irreducible dorsal dislocation of navicular on talus - this is the pathological definition
- Distinguishing test = forced plantar-flexion lateral radiograph - navicular does NOT reduce in CVT
- Talus is nearly vertical; calcaneus in equinus; forefoot dorsiflexed and abducted
- 50% associated with neuromuscular conditions (myelomeningocele, arthrogryposis most important)
- Treatment progression: Serial casting (Dobbs/reverse Ponseti) → Percutaneous K-wire + Achilles tenotomy → Age-based open surgery → Triple arthrodesis in adolescents
- Navicular is unossified until age 3 - use first metatarsal/medial cuneiform as surrogate on X-ray
- Distinguish from calcaneovalgus foot: CVT has equinus hindfoot; calcaneovalgus has calcaneus (dorsiflexed) hindfoot
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 1324-1325; Miller's Review of Orthopaedics 9th Ed, p. 284
Hallux valgus
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the material needed for a comprehensive MS Ortho answer on hallux valgus.
Hallux Valgus — MS Ortho
Definition
Hallux valgus (HV) is a complex 3D deformity of the first ray characterised by:
- Lateral deviation of the great toe at the first metatarsophalangeal (MTP) joint
- Medial deviation (varus) of the first metatarsal (metatarsus primus varus)
- Pronation of the hallux on its longitudinal axis
- Medial prominence of the first metatarsal head (bunion - bone + bursa)
- Lateral subluxation of the sesamoid apparatus
It is the most common forefoot deformity and affects women far more than men. It is frequently bilateral.
Anatomy of the Deformity
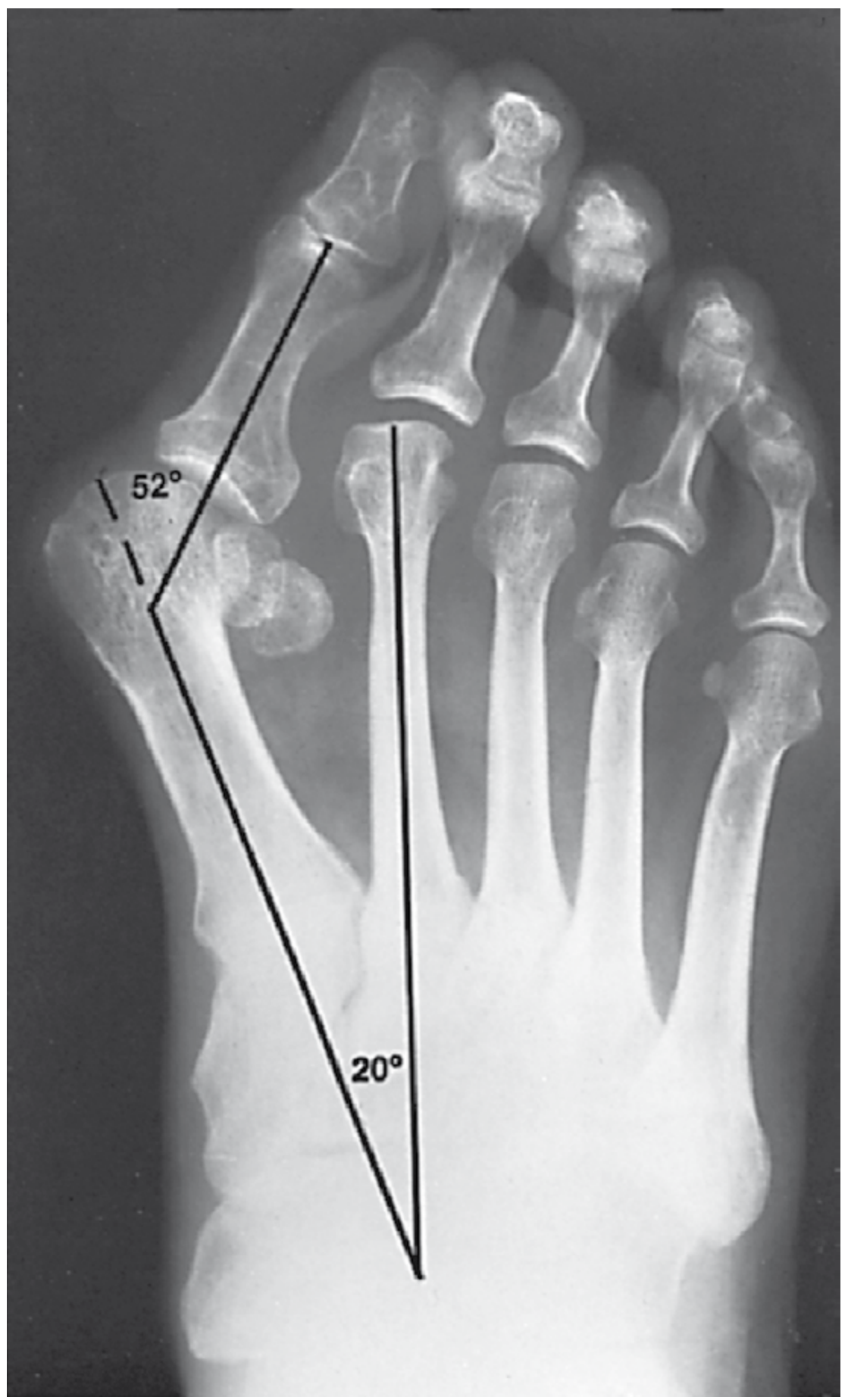
Severe hallux valgus: HVA = 52°, IMA = 20°, sesamoids laterally dislocated. (Campbell's Operative Orthopaedics, 15th Ed)
The key pathoanatomic associations are:
| Feature | Description |
|---|---|
| Metatarsus primus varus | Medial angulation of 1st metatarsal - widens IMA |
| Wide intermetatarsal angle | Between 1st and 2nd metatarsals |
| Sesamoid sling dislocation | Sesamoids shift laterally, become deforming force |
| Hallux pronation | As metatarsal head moves medially, toe pronates |
| Incongruent MTP joint | Subluxation of proximal phalanx laterally on metatarsal head |
| Increased DMAA | Distal metatarsal articular angle - articular surface tilts laterally |
| Bunion formation | Medial eminence hypertrophy + adventitial bursa |
The vicious cycle: With increasing deformity, the sesamoid sling (with all intrinsic muscles) rotates off the plantar surface of the metatarsal head. The sesamoids then act as a valgus deforming force, while the intrinsic-extrinsic muscle balance is lost, worsening the deformity progressively.
Etiology
The cause remains controversial. Contributing factors include:
- Genetic / familial - strongest association, especially in adolescents
- Tight/narrow footwear - accelerates development; highest HV rates in shoe-wearing populations
- Hypermobility of first ray - TMT1 joint laxity contributes (controversial)
- Pronated flatfeet - altered foot mechanics
- Abnormal insertion of posterior tibial tendon
- Increased obliquity of first metatarso-medial cuneiform joint - predisposes to metatarsus primus varus
- Rheumatoid arthritis - causes severe HV with MTP joint destruction
The strongest evidence supports lateral deviation of the great toe as the primary deformity in adults, with medial metatarsal angulation being secondary. In adolescents, metatarsus primus varus may be the principal driver.
Clinical Features
Symptoms:
- Pain over the medial eminence (bunion pain) - most common complaint
- Difficulty fitting shoes (narrow toe box)
- Second toe deformity/pain - often the primary complaint in advanced cases
- Metatarsalgia - pain under 2nd metatarsal head (first ray defunctioned)
- Plantar callosity beneath 2nd MTP joint
- Corn on medial aspect of 1st MTP or dorsum of 2nd toe
Signs:
- Lateral deviation of hallux, medial prominence at 1st MTP
- Bunion - swelling (bone + bursa) over medial eminence
- Pronation of hallux (nail facing medially)
- Hammer/claw deformity of 2nd toe
- Reduced/painful range of motion at 1st MTP (if OA has developed)
- Palpable sesamoids in lateral position (normally plantar)
- Assess: arch height, lesser toes, plantar callosities, gastrocnemius contracture, TMT1 hypermobility
Radiographic Evaluation
Standard: Weight-bearing AP and lateral radiographs of the foot
Key Angles
| Measurement | Normal | Hallux Valgus |
|---|---|---|
| Hallux Valgus Angle (HVA) | < 15° | > 15° |
| Intermetatarsal Angle (IMA) | < 9° | > 9° |
| Distal Metatarsal Articular Angle (DMAA) | < 10° | Often elevated |
| Proximal Phalangeal Articular Angle (PAA) | < 7-10° | May be elevated |
| Sesamoid position | Graded 1-7 (tibial sesamoid to lateral) | Grade 5-7 = fully dislocated |
Severity Classification (by HVA + IMA):
| Severity | HVA | IMA |
|---|---|---|
| Mild | 15-20° | 9-11° |
| Moderate | 20-40° | 11-18° |
| Severe | > 40° | > 18° |
MTP Joint Congruency (critical for planning):
- Congruent joint - articular surfaces parallel; deformity is within the joint surfaces (DMAA elevated); correcting by moving the metatarsal head only would leave an incongruent joint - requires correction at the articular level
- Incongruent joint - subluxated; metatarsal head can be realigned with soft-tissue + osteotomy
Treatment
Non-operative (First line)
- Wide toe box shoes
- Bunion pads / toe spacers
- Night splints (do NOT correct deformity permanently)
- Activity modification
- Treat pain but cannot correct the structural deformity
- Operative correction for cosmetic reasons alone is NOT indicated (except in progressive adolescent deformity)
Surgical Treatment
Indications:
- Persistent pain despite adequate non-operative management
- Progressive deformity
- Significant functional limitation
- NOT cosmesis alone (10% dissatisfaction rate with surgery)
Surgery is guided by:
- Severity of deformity (HVA, IMA, DMAA)
- MTP joint congruency
- Presence of arthritis
- Age and activity level
- First TMT joint hypermobility
- Adolescent vs adult
Surgical Options by Severity
A. Soft-tissue Procedures Alone
Modified McBride Procedure (Soft-tissue realignment)
- Indications: Mild-to-moderate HV with congruent joint; IMA < 13°; HVA < 25°; age > 55 years
- Components:
- Medial eminence resection
- Adductor hallucis tenotomy (from fibular sesamoid)
- Lateral capsulotomy of 1st MTP
- Fibular sesamoidectomy (McBride) OR lateral FHB release (modified - avoids hallux varus)
- Medial capsular imbrication (capsulorrhaphy)
- Note: Original McBride included fibular sesamoidectomy - now considered too aggressive due to hallux varus risk
B. Distal Metatarsal Osteotomies
Chevron Osteotomy (Austin Procedure)
- Indications: Mild-to-moderate HV; HVA < 35-40°; IMA < 15°; age < 50 years preferred
- Technique: V-shaped (60°) osteotomy through the metatarsal head - capital fragment displaced laterally 3-5 mm
- Combined with medial eminence resection and medial capsulorrhaphy
- Fixation: K-wire or cortical screw
- Results: 85-95% good results
- Advantages: Through cancellous bone (stable, good healing), minimal shortening, inherent stability
- Modified extracapsular chevron is the current workhorse for mild-moderate deformity
Akin Osteotomy (proximal phalanx)
- Medially-based closing wedge osteotomy at base of proximal phalanx
- Corrects hallux valgus interphalangeus (deformity distal to MTP joint)
- Corrects ~8° valgus per 2.5-3 mm of wedge removed
- Used as adjunct to other osteotomies; rarely indicated alone
C. Shaft Osteotomies
Scarf (Z) Osteotomy
- Indications: Mild-to-moderate HV; IMA 11-18°; HVA 20-40°
- Technique: Z-shaped osteotomy along the shaft of 1st metatarsal; capital fragment displaced laterally
- Can also correct DMAA, lengthen/shorten metatarsal, plantarflex capital fragment
- Fixation: 2 cortical screws
- Complication: "Troughing" (metatarsal collapse into plantar fragment - prevented by not shortening the short arms excessively)
Ludloff Osteotomy
- Oblique shaft osteotomy; used for moderate-severe deformity
D. Proximal/Basal Metatarsal Osteotomies
Used for severe HV with IMA > 15°:
| Osteotomy | Type |
|---|---|
| Proximal chevron | Medially-based closing wedge at base of 1st MT |
| Crescentic (Mann) | Rotational correction proximally |
| Opening wedge | Lateral-based opening wedge |
Combined distal soft-tissue + proximal osteotomy is the classic operation for moderate-severe HV.
E. First TMT Joint Arthrodesis (Lapidus Procedure)
Modified Lapidus:
- Indications:
- Severe HV with IMA > 15°
- Hypermobile/unstable TMT1 joint
- Recurrent HV after previous osteotomy
- Adolescent HV with open physis (relative)
- Technique: Arthrodesis of 1st metatarso-medial cuneiform joint + adductor release + medial capsulorrhaphy
- Corrects the deformity at its root (metatarsus primus varus)
F. First MTP Joint Procedures
Keller Resection Arthroplasty
- Resection of proximal 1/3 of proximal phalanx
- Indications: Elderly, low-demand patients; HVA < 25°; age > 55 years; arthritis of 1st MTP
- Disadvantages: Weakness of push-off (cock-up hallux), transfer metatarsalgia, shortening; high recurrence without fusion
First MTP Joint Arthrodesis
- Gold standard for: Severe HV with MTP OA; rheumatoid HV; neuromuscular HV; recurrent/failed previous surgery; cerebral palsy HV
- Position: 10-15° valgus, 25-30° dorsiflexion (relative to floor)
- Best long-term outcomes and lowest recurrence rate
- Akin osteotomy may be added for hallux valgus interphalangeus
Age-Based Surgical Approach Summary
| Patient Profile | Preferred Surgery |
|---|---|
| Mild HV, congruent joint | Modified McBride (soft tissue) |
| Mild-moderate, IMA < 15° | Chevron ± Akin |
| Moderate, IMA 11-18° | Scarf osteotomy |
| Moderate-severe | Distal soft tissue + proximal osteotomy |
| Severe / TMT1 hypermobile | Lapidus arthrodesis |
| Elderly, arthritic | Keller or 1st MTP fusion |
| Rheumatoid / neuromuscular | 1st MTP fusion |
| Adolescent, progressive | Lapidus (if TMT1 open) or epiphysiodesis |
Complications
General:
- Recurrence (most common, esp. with inadequate IMA correction or ligamentous laxity)
- Transfer metatarsalgia (pain shifts to 2nd/3rd MTP)
- Infection, wound dehiscence
- Nerve injury: dorsomedial cutaneous nerve (terminal branch)
Procedure-specific:
- Hallux varus - overcorrection; due to overzealous lateral release or fibular sesamoidectomy
- Avascular necrosis of 1st metatarsal head (chevron/distal osteotomies - rare if periosteum respected)
- Dorsal malunion - first metatarsal elevated, causes transfer metatarsalgia
- Troughing (scarf osteotomy)
- Non-union (Lapidus - ~1%)
- Shortened first ray (Keller, metatarsal neck osteotomy)
- Cock-up hallux (Keller arthroplasty)
- Stiffness / reduced MTP range
Juvenile Hallux Valgus
- Family history very common
- IMA often the primary driver
- Surgical treatment more difficult and disappointing
- Open physis is a relative contraindication to osteotomy through the physis
- Lateral hemiepiphysiodesis (medial physis tethering) used for progressive deformity with adequate remaining growth
- Lapidus (if TMT1 hypermobile) preferred over proximal metatarsal osteotomy
- Recurrence rate is higher than in adults
Key Points for Exam
- Three components of HV: lateral hallux deviation + medial 1st MT angulation + hallux pronation
- HVA (normal < 15°) and IMA (normal < 9°) are the key angles on weight-bearing AP X-ray
- Congruent vs incongruent joint determines whether distal osteotomy alone can correct, or whether articular surface correction (DMAA correction or MTP fusion) is needed
- Chevron: mild-moderate, IMA < 15°, HVA < 40°, through cancellous bone, stable
- Lapidus: hypermobile TMT1 + severe HV - corrects at root cause
- MTP fusion: best for arthritic, rheumatoid, recurrent, neuromuscular HV - lowest recurrence
- Sesamoid realignment is essential - failure to reduce sesamoids = recurrence
- Hallux varus is the dreaded complication of overcorrection (especially with fibular sesamoidectomy)
- Operative correction for cosmesis alone is NOT indicated (10% dissatisfaction rate)
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 87; Bailey and Love's Short Practice of Surgery 28th Ed, Chapter 41; Miller's Review of Orthopaedics 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.