I have all the material I need for a comprehensive masterclass. Let me now compile this into a definitive, well-structured response.
🏥 Abdominal Wall & Ventral Hernia — Masterclass
Sources: Fischer's Mastery of Surgery (8th ed.), Sabiston Textbook of Surgery, Bailey & Love's Short Practice of Surgery (28th ed.), Current Surgical Therapy (14th ed.), Mulholland & Greenfield's Surgery (7th ed.)
1. ANATOMY OF THE ABDOMINAL WALL
Layers (Surface to Deep)
- Skin
- Subcutaneous tissue (Camper's & Scarpa's fascia)
- External oblique muscle/aponeurosis - fibers run inferomedially
- Internal oblique muscle - fibers run superomedially (perpendicular to external oblique)
- Transversus abdominis muscle (TA) - fibers run transversely
- Transversalis fascia
- Preperitoneal fat
- Peritoneum
Key Structures
| Structure | Description |
|---|
| Linea alba | Fibrous band from xiphoid to pubic symphysis, formed by aponeurotic fusion of all three flat muscles |
| Linea semilunaris | Lateral border of rectus abdominis; junction of oblique and TA aponeuroses |
| Rectus sheath | Above arcuate line: anterior = EO + anterior IO lamella; posterior = posterior IO lamella + TA. Below arcuate line: all aponeuroses pass anteriorly |
| Arcuate line (Douglas) | ~halfway between umbilicus and pubic symphysis; below this, posterior rectus sheath consists only of transversalis fascia |
| Deep inferior epigastric vessels | Enter the retrorectus space; mark the lateral extent of the retrorectus dissection |
| Space of Retzius | Preperitoneal space anterior to bladder; exploited in pelvic dissection for groin/suprapubic hernia repair |
Neurovascular Supply
- Segmental nerves T7-T12 and L1 (iliohypogastric, ilioinguinal) run between the internal oblique and TA in the neurovascular plane
- Large perforating neurovascular bundles at the linea semilunaris define the lateral boundary of safe retrorectus dissection
2. DEFINITION & EPIDEMIOLOGY
A ventral hernia is a protrusion of abdominal contents through a defect in the anterior abdominal wall fascia. The term encompasses:
- Primary hernias - occur at inherent anatomic weak points (umbilical, epigastric, Spigelian)
- Incisional hernias - result from failure of a prior surgical wound
- Traumatic hernias - rare, from blunt force
Epidemiology:
- ~350,000 ventral hernia repairs/year in the USA
- ~500,000 inguinal hernia repairs/year in the USA
- Incisional hernia occurs in 2-30% of laparotomies
- Total procedural costs exceed $3.2 billion/year in the USA - and that does not count complication management
(Fischer's Mastery of Surgery, 8th ed.)
3. CLASSIFICATION
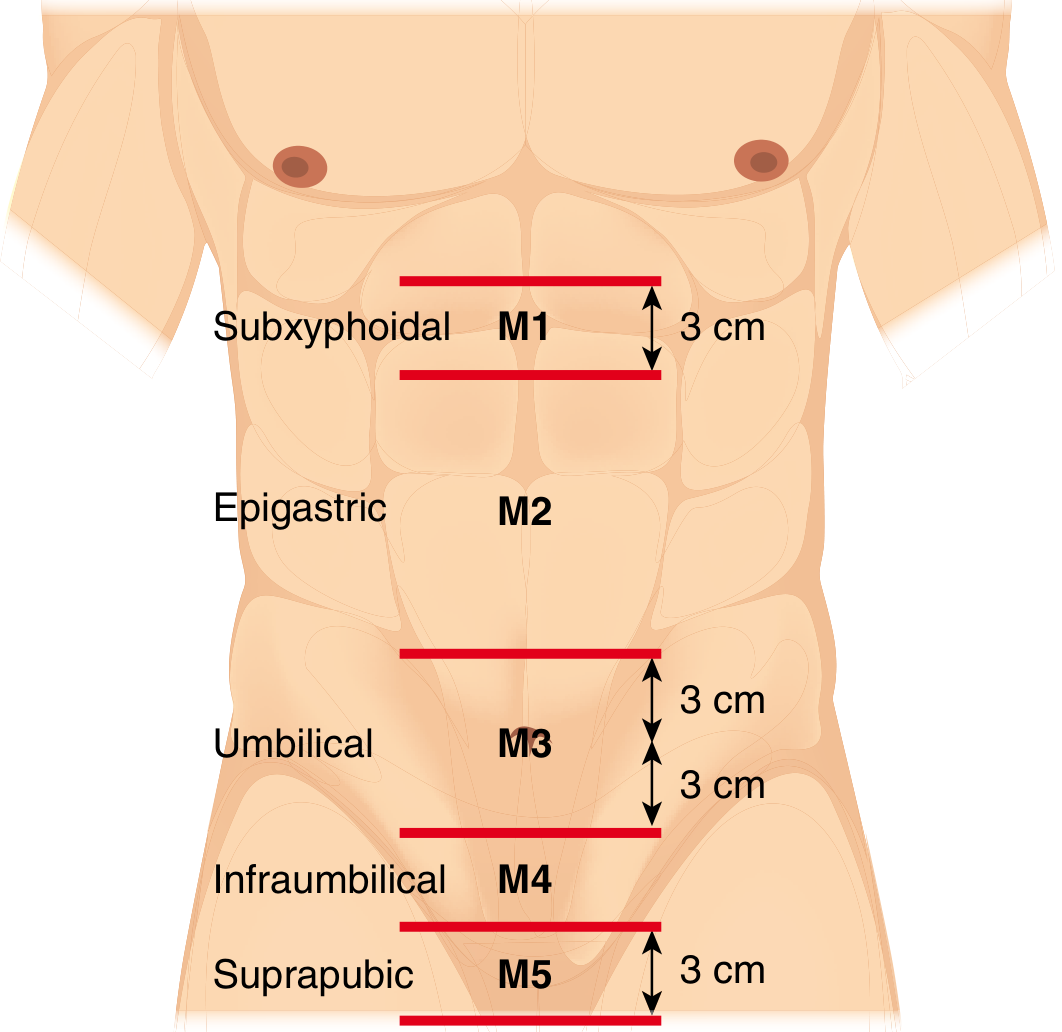
EHS (European Hernia Society) Midline Classification (Muysoms et al., Hernia 2009)
| Zone | Location | Landmark |
|---|
| M1 | Subxyphoidal | Upper boundary to 3 cm below xiphoid |
| M2 | Epigastric | >3 cm below xiphoid to 3 cm above umbilicus |
| M3 | Umbilical | 3 cm above to 3 cm below umbilicus |
| M4 | Infraumbilical | >3 cm below umbilicus to 3 cm above pubis |
| M5 | Suprapubic | ≤3 cm above pubis |
EHS Lateral classification: L1 (subcostal), L2 (flank), L3 (iliac), L4 (lumbar)
Size classification (EHS): Small (<4 cm), Medium (4-10 cm), Large (>10 cm)
Ventral Hernia Working Group (VHWG) Grade - for mesh selection
| Grade | Description |
|---|
| 1 | Low risk, no comorbidities |
| 2 | Smoking, obesity, DM, COPD, or immunosuppression |
| 3 | Potentially contaminated field (prior wound infection, enterotomy, colonized mesh) |
| 4 | Infected field / septic dehiscence / infected mesh |
(Current Surgical Therapy, 14th ed.)
4. TYPES OF PRIMARY VENTRAL HERNIAS
Umbilical Hernia
- Defect within 3 cm superior or inferior to the umbilicus (EHS definition)
- Adults: acquired, due to gradual weakening of the linea alba around the umbilical ring
- Risk factors: obesity, multiple pregnancies, cirrhosis (ascites), COPD, connective tissue disorders
- In infants: usually close spontaneously by age 2-3; repair if persists beyond age 4-5
Epigastric Hernia
- Located >3 cm below xiphoid and >3 cm above umbilicus
- May be multiple and lateral to midline
- Often contain preperitoneal fat (falciform ligament) ± peritoneal sac
- Mechanism: weakness at vascular bundle penetration points through linea alba
Spigelian Hernia
- Incidence: 0.12-2.4% of all abdominal wall hernias
- At the lateral border of rectus muscle / medial edge of linea semilunaris
- Usually an intraparietal (interparietal) hernia - external oblique remains intact; hernia passes through TA and internal oblique only
- Most common below the arcuate line
- Often occult on examination; diagnosed by ultrasound or CT
- CT finding: hernia sac at lateral border of rectus in characteristic crescent sign
(Fischer's Mastery of Surgery, 8th ed.)
5. INCISIONAL HERNIA
Risk Factors
| Intrinsic | Extrinsic |
|---|
| Obesity (BMI >30) | Wound infection / SSI |
| DM | Emergency surgery |
| Malnutrition | Improper closure technique |
| Smoking | Use of rapidly absorbing suture |
| COPD | Suture:wound length ratio <4:1 |
| Collagen disorders | Reoperation through same incision |
| Older age | Steroids / immunosuppression |
Prevention
- The STITCH trial approach: small bites (0.5 cm × 0.5 cm) with a 4:1 suture-to-wound length ratio using slowly absorbable suture (PDS/Maxon) minimizes incisional hernia risk
- Prophylactic mesh placement at index laparotomy in high-risk patients is increasingly practiced
Pathophysiology of Recurrence
- Suture-only incisional hernia repair: 43% recurrence at 2 years, 63% at 10 years
- Mesh-based repair: 24% recurrence at 2 years, 32% at 10 years (Luijendijk et al.)
6. PREOPERATIVE WORKUP & OPTIMIZATION
Clinical Assessment
- History: onset, duration, change in size, reducibility, prior repairs, comorbidities
- Exam: size, reducibility, skin changes, overlying scarring, abdominal domain assessment
- Loss of domain (LOD): when hernia contents can no longer be safely reduced without respiratory compromise; identified by CT volumetry (hernia volume >20-25% of total abdominal volume)
Imaging
- CT with hernia protocol (supine ± Valsalva): standard for complex hernias
- Assess defect size and number
- Identify contents (bowel, omentum, solid organ)
- Evaluate loss of domain
- Detect incarceration/strangulation
- Ultrasound: for small, clinically ambiguous hernias (especially Spigelian)
Patient Optimization (mandatory before elective repair)
| Factor | Target |
|---|
| BMI | <40, ideally <35 |
| Smoking | Cessation ≥4-6 weeks preoperatively |
| HbA1c | <8% |
| Nutritional status | Albumin >3.0 g/dL |
| Respiratory function | Optimize COPD / asthma |
| Skin integrity | No active infection, healed wounds |
Progressive pneumoperitoneum (PP): Pre-operative insufflation of CO2 into the peritoneal cavity over several weeks to restore domain in massive LOD hernias. Helps condition the diaphragm and respiratory muscles.
7. SURGICAL PRINCIPLES: MESH
Why Mesh? (Evidence)
- Umbilical hernias <4 cm: mesh reduces recurrence (4% vs. 12%, HR 0.31); effect is present even for 1-2 cm defects
- EHS/AHS guidelines: mesh for defects >1 cm (EHS) or >2 cm (many centers)
- Optimal patients for suture-only primary repair: defect <1 cm AND BMI <30
Mesh Categories
1. Synthetic mesh (permanent)
| Type | Key Property |
|---|
| Polypropylene (PP) | Inert, hydrophobic, monofilament; no immune response; resists bacterial ingrowth; promotes tissue ingrowth; workhorse mesh |
| Polyester (POL) | Hydrophilic; promotes microvascular ingrowth; multifilament; slightly more infection-prone |
| ePTFE | Flat sheet; macroporous ventral / microporous visceral; safe against bowel but prone to colonization; always needs strong non-absorbable fixation |
- Net meshes (PP, POL): allow tissue ingrowth between strands; become integrated into host within months
- Sheet meshes (ePTFE): do not allow tissue ingrowth; become encapsulated
- Inlay mesh (edge-to-edge) is NEVER acceptable - extremely high recurrence; condemned
2. Composite/Barrier-coated mesh
- Dual-sided: parietal (PP/POL) side promotes integration; visceral side has anti-adhesive barrier (absorbable coating, titanium, etc.)
- Required for intraperitoneal placement (IPOM) to prevent bowel adhesions, fistulae, erosion
3. Biosynthetic (degradable synthetic)
- Combines tensile strength of synthetic with improved biocompatibility
- Slow degradation profiles preferred (fast degradation → high recurrence)
- After resorption, associated tissues retain mechanical strength
- Used in contaminated fields (clean-contaminated, contaminated)
4. Biologic mesh
- Derived from human/bovine/porcine tissue; scaffold for tissue regeneration
- Designed for infected/contaminated fields (VHWG Grade 3-4)
- EXPENSIVE; recurrence ~30% at 2 years in contaminated fields
- Intense foreign-body reaction, poor tissue integration in contaminated environments
- No FDA clearance for contaminated wounds; biologic mesh has not outperformed synthetic in randomized trials
- Reserve for grossly contaminated fields or last resort
5. Mesh plug (avoid)
- Pushed into small defects; produces "meshoma" - fibrous mass causing chronic pain
- Complications: mesh migration, erosion into adjacent organs, fistula
- Largely abandoned
(Bailey & Love's, 28th ed.; Current Surgical Therapy, 14th ed.)
Mesh Position Options
| Position | Description | Pros | Cons |
|---|
| Onlay | On top of anterior fascia closure | Simple, no peritoneal entry needed | Large skin flaps → high SSO/SSI risk; seroma |
| Sublay (retrorectus) | Between posterior rectus sheath and rectus muscle | Excellent tissue coverage, protected by muscle, low SSO | Technical complexity |
| Preperitoneal | Between peritoneum and transversalis fascia | No bowel contact, good coverage | Technical difficulty in obese |
| Intraperitoneal (IPOM) | Inside peritoneal cavity | Simple laparoscopic access | Requires barrier-coated mesh; adhesion/fistula risk |
| Inlay | Edge-to-edge across defect | - | Condemned - extremely high recurrence |
Overlap requirements:
- Onlay and sublay: minimum 3-5 cm in all directions
- Open retrorectus/TAR: minimum 5 cm overlap with bare polypropylene
- Fixation-free repair is feasible with sufficient overlap in defects ≤15 cm (Etemad et al.)
8. OPERATIVE APPROACHES: OPEN
Open Primary Repair (suture-only)
- Figure-of-eight or interrupted transverse closure
- Slowly absorbable monofilament (PDS) or permanent suture
- Permanent suture risk: foreign body sensation, suture granulomas - some surgeons avoid it
- Key: fascial healing takes >1 year; suture must last through the proliferative phase
Open Onlay Mesh Repair
- Fascial closure first, then mesh on top of anterior fascia
- Large subcutaneous flaps increase SSO/SSI risk - major drawback
Open Preperitoneal Repair (Umbilical/Epigastric)
- Curvilinear incision; dissect down to hernia sac
- Preserve hernia sac to facilitate preperitoneal plane entry
- Dissect preperitoneal pocket circumferentially: overlap of 3-5 cm
- Close peritoneal holes with absorbable suture; lay flat sheet of PP or hernia patch
- Intra-abdominal pressure holds mesh - fixation sutures often not needed
- Then close fascia over mesh with permanent or slowly absorbable suture
Open Intraperitoneal Repair (Hernia Patch)
- For thin peritoneum where preperitoneal pocket creation is risky
- Hernia sac transected at fascial level; contents reduced
- Barrier-coated patch placed intraperitoneally, fixed with sutures ± positioning tails/memory rings
- Fascia closed over top
9. MYOFASCIAL RELEASE TECHNIQUES (Component Separation)
These techniques are essential for large defects to achieve tension-free fascial closure and allow adequate mesh overlap. Each step provides incremental medial advancement.
A. External Oblique Release (Anterior Component Separation, ACS)
First described by Ramirez, 1990.
Steps:
- Create skin and subcutaneous flaps over anterior rectus sheath, lateral to rectus muscle
- Incise posterior rectus sheath just lateral to linea alba; separate rectus from posterior sheath
- Incise external oblique aponeurosis just lateral to linea semilunaris, from costal margin to iliac crest
- Separate external oblique from anterior lamella of internal oblique
- Close midline fascia
Advancement achieved: ~5 cm per side in the mid-abdomen (bilateral = up to 10 cm total)
Drawback: Large skin flaps create significant SSO/SSI risk; devascularizes the lateral flaps; limits future surgical options
B. Retrorectus Repair (Rives-Stoppa)
- Posterior rectus sheath incised just lateral to linea alba (bilateral)
- Rectus muscle separated from posterior sheath (retrorectus space)
- Wide mesh placed in this space, well vascularized, protected from bowel
- Lateral extent: linea semilunaris (neurovascular perforators)
- Inferiorly: below arcuate line, connect both sides; can extend into Space of Retzius to Cooper's ligaments
- Posterior sheath closed over mesh with 2-0 resorbable suture; anterior fascia then closed
C. Transversus Abdominis Release (TAR) - Posterior Component Separation (PCS)
First described by Novitsky et al., 2012. An extension of the retrorectus repair.
Indication: When retrorectus dissection alone cannot achieve tension-free fascial closure OR additional mesh overlap is desired (large defects)
Steps (after completing retrorectus dissection):
- At the linea semilunaris, the medial leaf of the posterior TA fascia is incised
- This releases the TA muscle, expanding the preperitoneal plane laterally beyond the linea semilunaris
- The plane is extended between the TA muscle anteriorly and the preperitoneal fat/peritoneum posteriorly
- Bilateral TAR opens a vast retromuscular/preperitoneal space for very large mesh placement
Advantage over ACS (Majumder cadaveric studies):
- Posterior component separation (TAR) provides greater myofascial advancement than anterior (ACS), especially in the upper and mid abdomen
- No skin flaps required → dramatically lower SSO/SSI and skin necrosis rates
- Preferred for complex abdominal wall reconstruction with large defects
(Fischer's Mastery of Surgery, 8th ed.)
10. MINIMALLY INVASIVE APPROACHES
Laparoscopic Ventral Hernia Repair (LVHR)
Introduction: 1993 (LeBlanc & Booth)
Technique (IPOM):
- 3-5 ports lateral to the hernia
- Complete adhesiolysis
- Hernia contents reduced
- Barrier-coated mesh placed intraperitoneally with adequate overlap (≥5 cm)
- Mesh fixated: transfascial sutures at corners + tacks/staples circumferentially
Advantages: Less wound morbidity, shorter hospital stay, faster recovery
Disadvantages:
- Requires intraperitoneal (barrier-coated) mesh → long-term adhesion/fistula risk
- Difficulty closing fascial defect (bulge persists even with reduced hernia)
- Challenging in patients with prior adhesions, multiple hernias, loss of domain
IPOM-Plus: IPOM with intracorporeal fascial defect closure - reduces seroma, improves cosmesis, reduces risk of mesh bulge
Robotic Ventral Hernia Repair
Since 2012, robotic platforms have enabled extraperitoneal and retrorectus repairs that were previously only feasible open.
Robotic Retrorectus (eTEP - extended totally extraperitoneal):
- Access retrorectus space via retroperitoneal ports
- Bilateral retrorectus dissection under robotic magnification
- Posterior sheath closed (barbed 2-0 slowly absorbable suture)
- Fascial defect closed with No.1 barbed suture (pulley technique at 10-12 mmHg)
- Bare polypropylene mesh placed in retrorectus pocket - no barrier needed
- Minimum 5 cm overlap in all directions
Key technical notes:
- If posterior sheath cannot close without undue tension → TAR must be considered
- Inability to close posterior sheath without tension → indication to convert to open
- Closing posterior sheath under tension → breakdown → intraparietal hernias
- Fixation: interrupted 3-0 absorbable suture or fibrin sealant; minimal fixation typically needed
Robotic TAR (rTAR):
- Extension of robotic retrorectus dissection
- Medial leaf of posterior TA fascia incised at linea semilunaris to expand preperitoneal plane laterally
- Enables repair of very large defects minimally invasively
Advantages of robotic over laparoscopic:
- Enhanced 3D visualization
- Articulating instruments - superior ergonomics
- Enables intracorporeal suturing (defect closure, posterior sheath closure)
- Facilitates extraperitoneal mesh placement (no barrier mesh needed)
(Fischer's Mastery of Surgery, 8th ed.)
11. SPECIAL HERNIAS
Parastomal Hernia
- Hernia adjacent to a stoma site (ileostomy or colostomy)
- Incidence: 24-86% of stoma patients at some point
- EHS Classification: Small (<5 cm) vs. Large (>5 cm) ± presence of stoma prolapse
- Management: conservative (hernia belt), stoma relocation, repair with mesh (Sugarbaker technique, keyhole technique, modified Sugarbaker)
Lumbar (Flank) Hernia
- Superior lumbar triangle (Grynfeltt): bounded by 12th rib, internal oblique, erector spinae - more common
- Inferior lumbar triangle (Petit): bounded by iliac crest, external oblique, latissimus dorsi
- Can be primary (acquired/congenital) or secondary (post-incisional)
- Often contain retroperitoneal fat; bowel herniation less common
Spigelian Hernia
- Location: lateral edge of rectus / medial edge of linea semilunaris, below arcuate line
- Intraparietal - external oblique intact; diagnosis missed on clinical exam
- CT or ultrasound required for diagnosis
- Repair: open or laparoscopic; mesh placement recommended
12. COMPLICATIONS OF HERNIA REPAIR
Surgical Site Events (SSE)
| Complication | Notes |
|---|
| Seroma | Most common; fluid collection in hernia sac or mesh space; most resolve spontaneously; aspiration if symptomatic |
| Hematoma | Drain if expanding; re-explore if unstable |
| SSI (skin/soft tissue) | Higher risk with onlay repair and large skin flaps |
| Surgical Site Occurrence (SSO) | Includes seroma, hematoma, SSI, wound dehiscence |
| Mesh infection | May require mesh explantation; biologic/biosynthetic preferred in contaminated fields |
Long-term Complications
| Complication | Notes |
|---|
| Recurrence | Main endpoint; 4-32% depending on technique and follow-up; mesh significantly reduces risk |
| Chronic pain | Nerve entrapment (especially with transfascial sutures); tack/staple neuropathy |
| Mesh migration | More common with sheet meshes, plug repairs, inadequate fixation |
| Bowel erosion/fistula | Intraperitoneal uncoated mesh; ePTFE colonization risk |
| Adhesions | Intraperitoneal mesh; barrier-coated meshes reduce but do not eliminate |
| Meshoma | Collagenous mass from mesh plug; chronic pain, may require excision |
Complications Specific to Minimally Invasive Repair
- Inability to tolerate pneumoperitoneum
- Trocar-site hernia
- Bowel injury during adhesiolysis (especially from thermal energy near hernia sac - electrosurgery must be used cautiously)
13. PERIOPERATIVE MANAGEMENT
Analgesia (Enhanced Recovery Protocol)
- Epidural analgesia for open hernia repair: large NSQIP/ACHQC database studies show increased LOS, increased complications (UTI, PE), and increased transfusion with no improvement in pain control - NOT recommended
- Preferred approach: TAP (transversus abdominis plane) blocks intraoperatively + preoperative "cocktail":
- Acetaminophen 1,000 mg
- Pregabalin 75 mg
- Celecoxib 400 mg
- This multimodal approach reduces LOS and opioid use
Abdominal Binder
- A 2024 systematic review/meta-analysis (PMID 39550494) found that abdominal binders after ventral hernia repair reduce seroma formation and improve patient comfort
Smoking
- A 2024 meta-analysis on smoking and hernia repair (PMID 39085514) confirmed smoking significantly increases complications and recurrence after both ventral and inguinal hernia repair - cessation is mandatory before elective repair
Local Anesthesia
- A 2025 systematic review (PMID 40420065) confirmed feasibility and safety of ventral hernia repairs under local anesthesia in selected patients
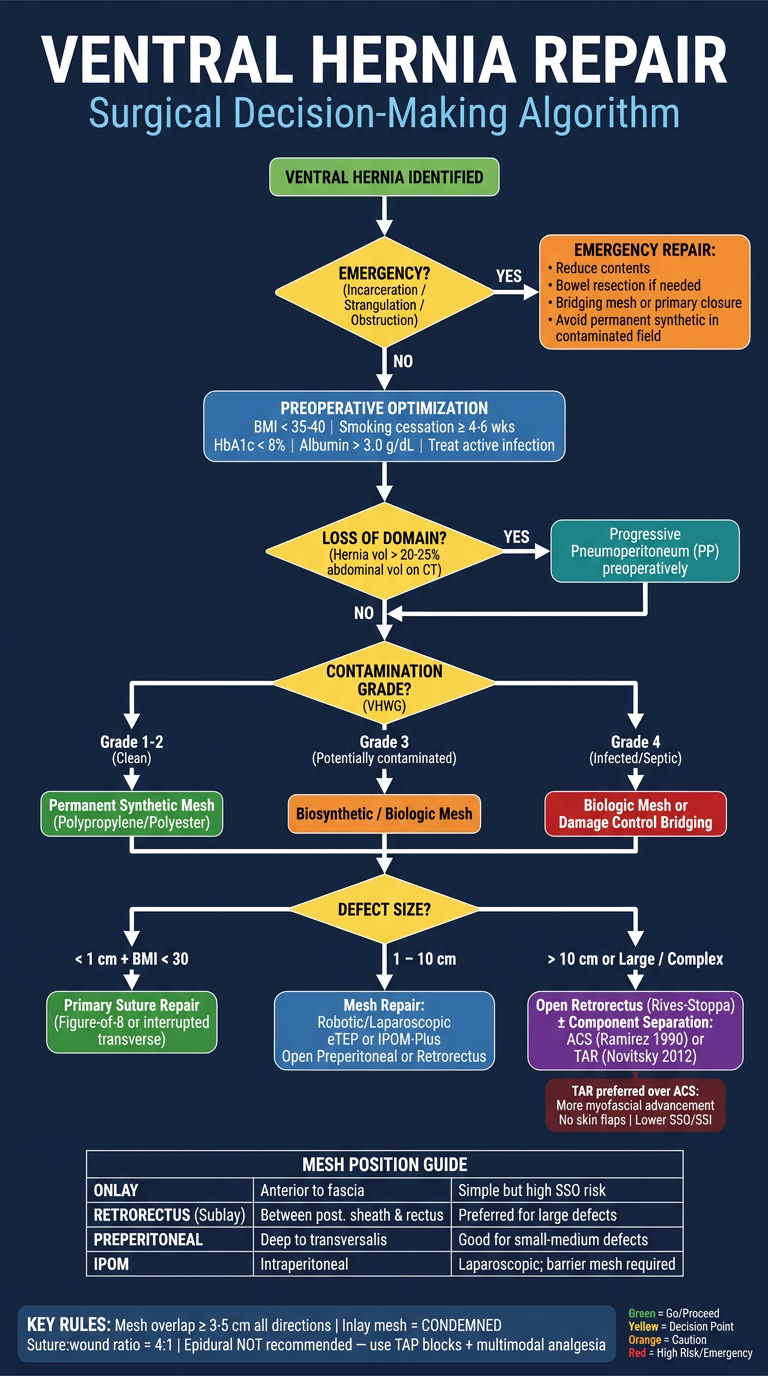
14. DECISION-MAKING FRAMEWORK
VENTRAL HERNIA IDENTIFIED
|
├── Asymptomatic, very small (<1 cm), low-risk patient
│ → Watch and wait (discuss risks/benefits with patient)
│
├── Symptomatic OR enlarging OR incarcerated/strangulated
│ → Surgical repair indicated
│
└── OPERATIVE PLANNING:
│
├── Optimize: BMI, smoking, DM, nutrition
│
├── Defect size?
│ ├── <1 cm + BMI<30 → Primary suture repair acceptable
│ ├── 1-4 cm → Mesh (preperitoneal or IPOM-Plus)
│ └── >4 cm → Mesh + consider component separation
│
├── Contamination grade? (VHWG)
│ ├── Grade 1-2: permanent synthetic mesh
│ ├── Grade 3: biosynthetic preferred; caution with synthetic
│ └── Grade 4: biologic (last resort) OR damage-control bridging
│
├── Loss of domain?
│ └── Yes → Progressive pneumoperitoneum preoperatively
│
└── Approach?
├── Small/medium, laparoscopic-suitable → Robotic/laparoscopic (eTEP or IPOM-Plus)
├── Large midline, complex → Open retrorectus ± TAR
└── Contaminated/emergency → Open ± bridging mesh
15. QUICK-REFERENCE HIGH-YIELD FACTS
| Fact | Value |
|---|
| Incisional hernia rate after laparotomy | 2-30% |
| Suture-only incisional hernia recurrence (10 yr) | 63% |
| Mesh-based incisional hernia recurrence (10 yr) | 32% |
| Umbilical hernia mesh vs suture (RCT) | 4% vs 12% recurrence |
| EHS: mesh recommended for defect | >1 cm |
| Mesh overlap required | ≥3-5 cm (onlay/preperitoneal); ≥5 cm (retrorectus) |
| Inlay mesh | Condemned - unacceptably high recurrence |
| TAR described by | Novitsky et al., 2012 |
| ACS (Ramirez technique) described by | Ramirez, 1990 |
| STITCH trial closure ratio | 4:1 suture:wound length |
| LVHR introduced | 1993 (LeBlanc & Booth) |
| Spigelian hernia incidence | 0.12-2.4% of all abdominal wall hernias |
| TAR advantage over ACS | More myofascial advancement, especially upper/mid abdomen; no skin flaps needed |
| Below arcuate line: posterior sheath | Transversalis fascia only |
| Epidural for hernia repair | NOT recommended (increased LOS, complications) |
Sources:
- Fischer's Mastery of Surgery, 8th ed., Chapters 216-217
- Sabiston Textbook of Surgery, Chapter 80
- Bailey and Love's Short Practice of Surgery, 28th ed., Chapter 64
- Current Surgical Therapy, 14th ed., Chapters 5, 10
- Mulholland & Greenfield's Surgery, 7th ed., Chapters 72-73