Make a note of tonometry from basic to advanced level, what happens, how does it happen, principle, how it works, recent advances, everything
Reading File
Finding Sources
Finding Sources
Searching PubMed
tonometry intraocular pressure measurement
Searching the Web
tonometry types principles recent advances 2024 2025 intraocular pressure measurement
Reading File
Reading File
Reading File
Searching PubMed
"intraocular pressure" AND "tonometry" AND "glaucoma"
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"tonometry" AND "rebound" OR "non-contact tonometry" AND "wearable" AND "intraocular pressure"
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
"continuous intraocular pressure" OR "wearable tonometer" OR "smart contact lens" IOP monitoring
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
tonometry recent advances 2024 2025 AI continuous monitoring smart contact lens ORA ocular response analyzer
I now have extensive material from multiple authoritative sources. Let me compile the comprehensive notes.
Tonometry - Complete Notes (Basic to Advanced)
1. What is Tonometry?
Tonometry is the clinical measurement of intraocular pressure (IOP) - the pressure within the eyeball. Because directly inserting a needle into a patient's eye is impractical, tonometers measure IOP indirectly by applying force to the cornea and measuring the eye's mechanical response to that force.
IOP is generated by the balance between aqueous humor production (by the ciliary body, ~2.5 µL/min) and its outflow through the trabecular meshwork into the Canal of Schlemm. The normal IOP is approximately 10-21 mmHg (average ~15 mmHg), maintained within ±2 mmHg in a healthy eye.
Source: Guyton and Hall Textbook of Medical Physiology
2. Why Measure IOP? - Clinical Significance
- Glaucoma screening and management - elevated IOP is the primary modifiable risk factor for glaucomatous optic neuropathy. Over 2 million people in the US have some degree of blindness from glaucoma, yet fewer than half are diagnosed. IOP > 25-30 mmHg can cause optic nerve damage; acute rises to 60-70 mmHg cause rapid blindness.
- Acute angle-closure glaucoma - a medical emergency; patients present with headache, nausea, vomiting, and may have surprisingly mild ocular pain. IOP measurement confirms the diagnosis.
- Ocular trauma - to detect penetrating injury (IOP will be abnormally low); NOTE: tonometry is contraindicated if globe rupture is suspected.
- Monitoring glaucoma treatment response (medical, laser, surgical).
- Pre/post refractive surgery assessment (LASIK changes corneal biomechanics and affects readings).
- Diurnal variation tracking - IOP fluctuates throughout the day; peak is often early morning.
Sources: Pfenninger & Fowler's Procedures for Primary Care; Roberts & Hedges' Clinical Procedures in Emergency Medicine
3. Physiological Basis - How IOP is Generated
The aqueous humor is produced by the ciliary body and circulates through the posterior chamber → pupil → anterior chamber → trabecular meshwork → Canal of Schlemm → episcleral veins.
The trabecular spaces have openings of only 2-3 micrometers, providing resistance to outflow. At 15 mmHg, inflow equals outflow at 2.5 µL/min. When outflow resistance increases (as in glaucoma), pressure builds up.
Factors that raise IOP:
- Increased aqueous production
- Decreased trabecular outflow (most common in glaucoma)
- Tight collar or breath-holding (obstructs venous return)
- Eyelid squeezing / blepharospasm
- Restricted extraocular muscles (e.g., thyroid myopathy)
- Systemic antihypertensives can modestly lower IOP
Source: Guyton & Hall; Kanski's Clinical Ophthalmology 10th ed.
4. Methods of Tonometry - Classification
There are four main measurement principles:
| Method | Principle | Example Device |
|---|---|---|
| Impression / Indentation | Measures depth of corneal deformation by a fixed-weight plunger | Schiotz tonometer |
| Applanation | Measures force needed to flatten a defined corneal area | Goldmann (gold standard), Perkins, Tono-Pen |
| Non-contact (Air-puff) | Air jet flattens cornea; time to flatten correlates with IOP | Pneumotonometer / NCT |
| Rebound | Magnetized probe bounced off cornea; deceleration correlates with IOP | iCare |
Plus:
- Tactile / Digital tonometry - crude, for gross estimation only
- Dynamic Contour Tonometry (DCT) - contour-matching sensor, cornea-independent
- Ocular Response Analyzer (ORA) - measures corneal hysteresis
5. The Schiotz Tonometer (Impression Tonometry)
Principle
A plunger of known weight (5.5 g standard; 7.5 g and 10 g weights available) is placed on the anesthetized cornea. The depth of indentation by the plunger is proportional to the resistance of the eye - i.e., how firm the eye is. The scale reading is then converted to mmHg using a Friedenwald conversion table.
The Schiotz actually measures total IOP (initial pressure + pressure added by the weight). Friedenwald introduced a "rigidity coefficient" to convert the scale reading to true IOP. Accuracy is most dependable with scale readings >5; if <5, the next heavier weight should be used.
Important caveat: If ocular rigidity is altered (e.g., after scleral buckle surgery, extreme myopia), the conversion tables are unreliable.
Technique
- Instill topical anesthetic drops (e.g., proxymetacaine 0.5%).
- Patient lies supine, looks straight up at a fixed target.
- Test the tonometer on a flat surface first - should read zero.
- Examiner separates the eyelids using bony orbital rims (no pressure on globe).
- Hold the tonometer vertically and lower it gently onto the corneal apex.
- Record the scale reading → look up IOP in the conversion table.
- Disinfect after use.
Errors
- Globe pressure from fingers or lid squeezing → falsely elevated reading
- Altered ocular rigidity → conversion table inaccuracy
- Poor calibration
Source: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Pfenninger & Fowler's
6. Goldmann Applanation Tonometry (GAT) - The Gold Standard
The Imbert-Fick Principle
Goldmann applanation tonometry is based on the Imbert-Fick principle:
For an ideal, dry, thin-walled sphere, the pressure inside (P) equals the force required to flatten its surface (F) divided by the area of flattening (A): P = F/A
In practice, the human cornea is NOT an ideal sphere - two confounding forces exist:
- Corneal rigidity - resists flattening (artificially lowers the measured force needed → IOP underestimated)
- Capillary attraction of the tear meniscus - pulls the tonometer toward the cornea (artificially raises the force needed → IOP overestimated)
Goldmann found these two forces cancel each other out exactly when the flattened area has a diameter of 3.06 mm. This is why Goldmann tonometry uses this specific diameter.
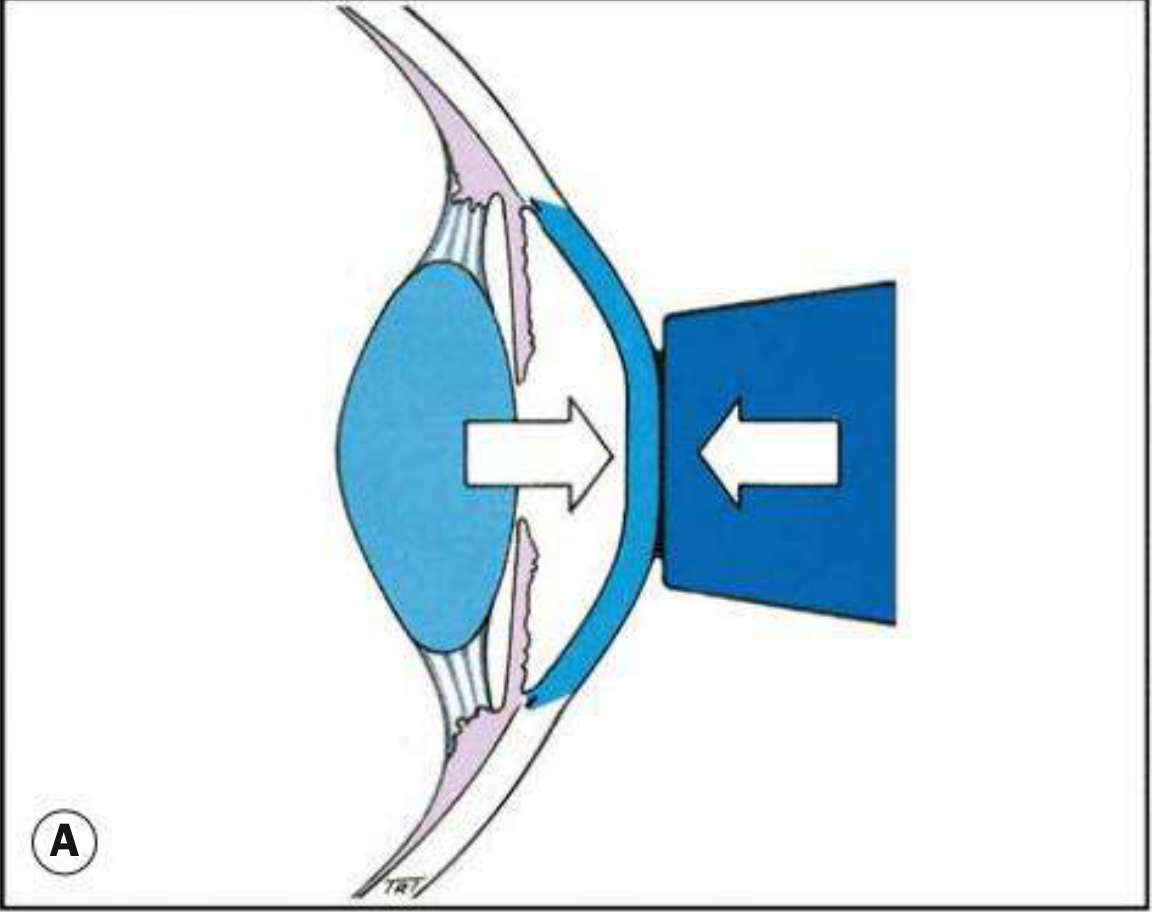
Fig. 1.43A - Physical principles of Goldmann tonometry. The prism is pressed against the cornea until a 3.06 mm diameter area is flattened. (Kanski's Clinical Ophthalmology 10th ed.)
The Double Prism and Mire Pattern
The Goldmann tonometer uses a biprism (double prism) mounted on a slit lamp. When the prism contacts the fluorescein-stained tear film under cobalt blue light, two green semi-circular mires appear - one above and one below the horizontal midline.
- The dial is turned to vary the applied force.
- When the inner margins of the two semi-circles just touch (align), the area of corneal contact is exactly 3.06 mm.
- Reading on the dial × 10 = IOP in mmHg.
Mire thickness should be ~10% of the arc diameter. Excessive fluorescein = mires too thick = overestimation. Insufficient fluorescein = mires too thin = underestimation.
Technique (Step by Step)
- Instill topical anesthetic (proxymetacaine 0.5%) and a small amount of fluorescein.
- Patient positioned at slit lamp with forehead against headrest, looking straight ahead (at examiner's opposite ear).
- Cobalt blue filter in place; illumination at maximum, directed obliquely (~60°).
- Dial preset at 1 (= 10 mmHg).
- Prism advanced until it just touches the corneal apex.
- View through the ocular - two green semi-circular mires visible.
- Rotate dial until inner margins align.
- Dial reading × 10 = IOP in mmHg.
Sources of Error in GAT
| Error | Effect on Reading |
|---|---|
| Excessive fluorescein | Overestimation |
| Insufficient fluorescein | Underestimation |
| Finger pressure on globe / lid squeezing | Falsely elevated |
| Thick cornea (CCT >520 µm) | Overestimation |
| Thin cornea (CCT <520 µm) (post-LASIK, NTG) | Underestimation |
| Corneal edema | Artificial lowering |
| Astigmatism >3 diopters | Distorted mires; error |
| Incorrect calibration | False readings |
CCT (Central Corneal Thickness) is a major confounder. GAT assumes CCT = 520 µm. Post-refractive surgery corneas are thinner AND biomechanically altered, causing significant underestimation. Calibration should be checked before each clinical session.
Source: Kanski's Clinical Ophthalmology 10th ed.
7. Perkins Applanation Tonometer
Uses the same Goldmann double prism principle but is portable and hand-held with its own light source. Can be used in:
- Bed-bound patients
- Anaesthetized patients
- Children (under general anesthesia)
- Patients who cannot sit at a slit lamp
Same accuracy as GAT; reading technique and mire pattern are identical.
8. Non-Contact Tonometry (Air-Puff / Pneumotonometry)
Principle
A controlled jet of air is directed at the cornea. The time required to sufficiently flatten the cornea (to a pre-set area) is electronically measured and is directly proportional to IOP. The instrument detects the moment of applanation by monitoring the reflection of an infrared beam off the cornea.
Advantages
- No contact with the eye - no anesthesia required
- No risk of infection transmission
- Useful for community screening and for children (no fear of contact)
- Fast
Disadvantages
- The air jet can startle patients (blink reflex, eye movement)
- Slightly less accurate than GAT, especially at extremes of IOP
- Accuracy improves if at least 3 readings are averaged
Originally considered a screening-only tool, NCT accuracy is now comparable to applanation tonometry for routine clinical use.
Source: Kanski's Clinical Ophthalmology; Pfenninger & Fowler's
9. Tono-Pen (Electronic Applanation / MacKay-Marg Type)
The MacKay-Marg principle is a refined impression technique in which a much smaller area of cornea is indented. The Tono-Pen AVIA (Reichert) is the modern version.
How it works
- A small probe tip contains a strain-gauge transducer that measures the applied force.
- The probe is touched to the anesthetized cornea multiple times (typically 10 measurements).
- The device automatically averages valid readings and displays IOP with a statistical confidence indicator (displayed as a percentage - lower % = more consistent readings = more reliable).
Advantages
- Portable and hand-held
- Works on distorted, edematous, or scarred corneas where GAT fails
- Can measure IOP through soft contact lenses
- Disposable covers (Ocu-Film) eliminate infection transmission risk
- Useful in the ED, ICU, and at the bedside
Technique
- Spray probe tip with compressed gas to clean.
- Apply a new Ocu-Film disposable cover.
- Calibrate the device (hold vertically then quickly flip upward).
- Instill topical anesthetic.
- Touch probe lightly and perpendicularly to the corneal apex 10 times.
- Device displays IOP once sufficient valid measurements are collected.
Source: Roberts & Hedges' Clinical Procedures in Emergency Medicine
10. Rebound Tonometry (iCare)
Principle
A lightweight magnetized metal probe (~1.8 mm plastic ball attached to a wire) is accelerated toward and bounced off the central cornea. The deceleration of the probe upon corneal contact is proportional to IOP - a stiffer, higher-pressure eye decelerates the probe faster.
The iCare device uses electromagnetic induction to:
- Accelerate the probe
- Detect its deceleration on corneal contact
- Calculate IOP from the deceleration curve
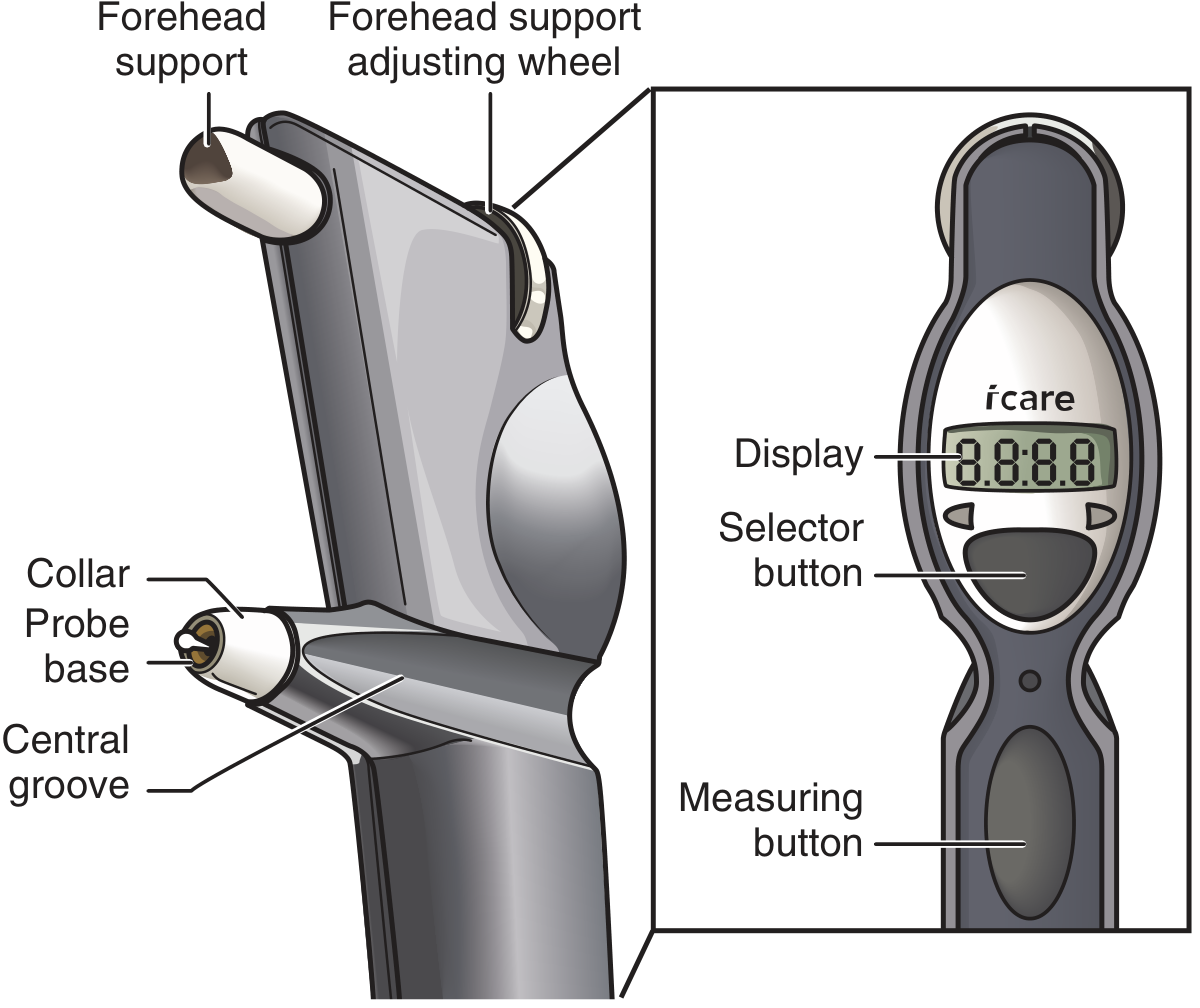
iCare tonometer components. (Roberts & Hedges)
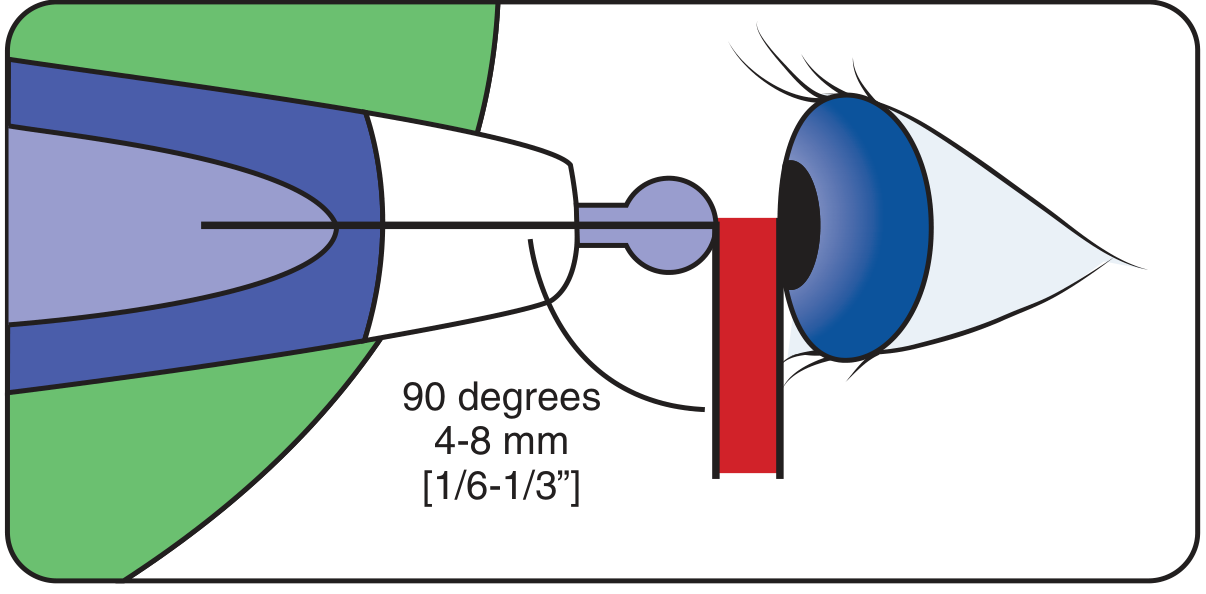
The probe must be held at 90° to the frontal plane, 4-8 mm from the cornea for a valid measurement.
Advantages
- No anesthesia required (most comfortable method)
- Portable
- Disposable plastic-tipped probes (no infection risk)
- Can be used for self-monitoring at home (iCare HOME2)
- Positioning system and magnet in applicator assist correct alignment
- Correlates closely with GAT and Tono-Pen XL
iCare HOME2
Designed for patients needing diurnal IOP monitoring (IOP fluctuates significantly throughout the day). Patients can self-administer at home at different times, capturing data that a single clinic visit would miss.
Source: Kanski's Clinical Ophthalmology 10th ed.; Roberts & Hedges'
11. Dynamic Contour Tonometry (DCT) - PASCAL
Principle
Uses a solid-state pressure sensor embedded in a concave tip that matches the corneal contour. Rather than flattening the cornea (applanation), DCT measures IOP while maintaining the cornea in its natural curved shape. This approach aims to measure IOP independently of corneal mechanical properties (thickness, rigidity, biomechanics).
Key advantage
Studies comparing DCT and GAT against direct manometric intracameral IOP show DCT provides a more physiological measurement, particularly in eyes where corneal biomechanics confound GAT (post-LASIK, keratoconus, ocular hypertension with thick corneas, normal-tension glaucoma with thin corneas).
DCT also produces a Pulsatility Index (PI) - the amplitude of the IOP pulse wave generated by each heartbeat, which reflects ocular blood flow.
12. Ocular Response Analyzer (ORA)
The ORA is an advanced non-contact device that fires a controlled air jet and uses an infrared detection system to measure the cornea's response during both inward (applanation) and outward (rebound) deformation.
Key parameters
- IOPg (Goldmann-correlated IOP) - comparable to GAT
- IOPcc (corneal-compensated IOP) - adjusted for corneal biomechanics
- Corneal Hysteresis (CH) - the difference between the inward and outward applanation pressures. Reflects the viscoelastic dampening capacity of the cornea. Low CH is associated with glaucoma progression and progressive optic nerve damage independent of IOP.
- Corneal Resistance Factor (CRF) - related to corneal elasticity
CH has emerged as a significant predictive biomarker for glaucoma susceptibility and progression, independent of CCT and IOP.
13. Tactile / Digital Tonometry
The simplest and crudest method. The examiner rests both hands on the patient's forehead and alternately applies gentle digital pressure to the globe through the upper eyelid with both index fingers - one finger indents while the other feels the compliance (fluctuation) of the globe.
A relatively unskilled examiner can detect the very high IOP of acute angle-closure glaucoma (>40-50 mmHg) - the eye feels stony hard compared to a normal eye. This method cannot accurately quantify IOP.
Source: Roberts & Hedges'
14. Contraindications
Tonometry is absolutely contraindicated with:
- Suspected penetrating or perforating ocular injury - pressure on the globe can extrude intraocular contents.
Relative contraindications:
- Active corneal infection or ulceration
- Recent corneal surgery
- Corneal abrasion (Tono-Pen may be attempted in some cases)
- Ocular surface disease or severe conjunctivitis
Source: Roberts & Hedges'; Pfenninger & Fowler's
15. Comparison Table of Tonometry Methods
| Method | Principle | Anesthesia | Portability | Accuracy | Best Use |
|---|---|---|---|---|---|
| Goldmann (GAT) | Applanation (Imbert-Fick) | Required | Slit lamp (fixed) | Gold standard | Ophthalmology clinic |
| Perkins | Applanation (Imbert-Fick) | Required | Hand-held | = GAT | Bedside, children under GA |
| Schiotz | Impression/indentation | Required | Portable | Good (affected by rigidity) | Primary care, ED |
| Tono-Pen | Electronic applanation | Required | Hand-held | Good | ED, ICU, distorted corneas |
| Air-puff / NCT | Non-contact applanation | NOT required | Desktop | Screening-level | Screening, community |
| iCare (rebound) | Electromagnetic rebound | NOT required | Hand-held | Good | Home, ED, children |
| DCT (PASCAL) | Contour-matching pressure | Required | Slit lamp | Cornea-independent | Post-LASIK, NTG |
| ORA | Bidirectional applanation | NOT required | Desktop | Biomechanics-aware | Glaucoma risk stratification |
16. Normal Values and Clinical Thresholds
| Parameter | Value |
|---|---|
| Normal IOP (average) | ~15 mmHg |
| Normal IOP range | 10-21 mmHg |
| Ocular hypertension threshold | > 21 mmHg |
| Glaucoma damage risk (elevated) | > 25-30 mmHg |
| Acute angle-closure glaucoma | Often 40-70 mmHg |
| Target IOP in treated glaucoma | Individualized; often < 15-18 mmHg |
| CCT (assumed by GAT) | 520 µm |
17. Factors Affecting IOP Readings
Patient factors
- Central Corneal Thickness (CCT) - most important confounder. Thin corneas → GAT underestimates. Thick corneas → GAT overestimates.
- Corneal edema - lowers reading artificially
- Post-refractive surgery (LASIK, PRK) - cornea is thinned AND biomechanically altered → significant IOP underestimation
- Astigmatism >3 diopters - distorted mires; rotate prism to minus axis to compensate
- Systemic antihypertensive medications - beta-blockers, calcium channel blockers, ACE inhibitors may modestly lower IOP (Leung et al., 2023)
- Exercise - aerobic exercise lowers IOP transiently (Gildea et al., 2024)
- Diurnal variation - IOP peaks in early morning; a single clinic reading misses peaks
- Valsalva / tight collar - raises IOP
- Body position - IOP is higher lying down than sitting upright
Measurement factors
- Fluorescein amount (too much or too little)
- Examiner applying pressure on globe
- Patient lid squeezing or blepharospasm
- Calibration error
18. Diurnal IOP Monitoring
IOP varies by as much as 6-10 mmHg during a 24-hour period. Peak is usually between 6-8 AM and trough in the late afternoon. In glaucoma patients, the diurnal range can be larger.
A single daytime office reading may miss dangerous nocturnal IOP spikes, which contribute to glaucoma progression even in patients whose daytime IOP appears controlled. This is the key rationale for:
- iCare HOME2 - self-monitoring at multiple time points
- 24-hour IOP monitoring protocols in research settings
- Continuous IOP sensors (see recent advances)
19. Recent Advances
A. Smart Contact Lens Sensors for Continuous IOP Monitoring
The most exciting frontier: embedding microsensors within a contact lens to allow real-time, continuous IOP monitoring without clinic visits.
Key developments:
- Hydrogel-based smart contact lenses with capacitive/resistive microsensors and wireless (NFC) data transmission (Zhu et al., 2022 - ACS Sensors, PMID 36260093)
- Contact lens sensor systems for continuous IOP monitoring validated in human eyes (Wei et al., 2025 - Ophthalmol Sci, PMID 40599256)
- All-polymer smart contact lens capable of real-time IOP monitoring AND responsive drug release in preclinical models - a single device that both monitors pressure and delivers glaucoma medication when IOP exceeds a threshold (Cai et al., 2026 - Science Translational Medicine, PMID 41950306)
This represents a shift from episodic clinic-based measurement to closed-loop theranostic systems.
B. Wearable Glaucoma Diagnostics
Beyond contact lenses, wearable platforms (eyelid-mounted sensors, ocular inserts) are being studied for continuous IOP capture. A 2024 review in Bioengineering surveyed the range of approaches and identified remaining challenges including calibration drift, battery life, and biocompatibility (Shean et al., 2024 - PMID 38391624).
C. Corneal Biomechanics Beyond CCT
The recognition that Corneal Hysteresis (CH) - not just thickness - predicts glaucoma risk and progression has changed how tonometry results are interpreted. Low CH eyes need more aggressive IOP targets. ORA-derived CH is now incorporated into glaucoma risk models.
D. Home Tonometry (iCare HOME2)
Now commercially available and validated, home tonometry allows patients to self-measure at different times of day. It provides data on diurnal IOP fluctuation that was previously only obtainable by hospital-based phased tonometry.
E. AI-Assisted Tonometry and IOP-Disease Relationships
Emerging research is using machine learning to predict glaucoma risk and progression from IOP patterns, corneal biomechanics, and structural data combined. The evolving concept of the IOP-glaucoma relationship (Asrani et al., 2024) recognizes that IOP alone is insufficient - biomechanical susceptibility, cerebrospinal fluid pressure gradient, ocular perfusion pressure, and vascular factors all interact.
F. Displacement-Pressure Biparametric Sensors
Novel soft sensory systems measuring both displacement and pressure simultaneously improve IOP estimation accuracy, especially for eyes with unusual biomechanics (Cheng et al., 2024 - Natl Sci Rev, PMID 38707205).
20. Clinical Correlations
Glaucoma Screening Protocol
Tonometry alone is insufficient for glaucoma diagnosis. The complete screen includes:
- IOP by tonometry
- Optic disc examination (cup-to-disc ratio, RNFL)
- Visual field testing
All three are needed for sensitivity and specificity. Patients with high IOP but normal discs and fields = ocular hypertension (not glaucoma). Patients with glaucomatous discs but normal IOP = normal-tension glaucoma (require pressure-independent management).
Acute Angle-Closure Glaucoma in the ED
- IOP typically 40-70+ mmHg
- Systemic symptoms (nausea, vomiting, headache) can mask the ocular origin
- Tono-Pen or iCare are preferred in the ED setting
- Immediate treatment: IV acetazolamide, topical beta-blockers, pilocarpine, +/- laser iridotomy
Post-LASIK IOP
Always correct for corneal thinning. If CCT is not available, assume IOP is underestimated by approximately 1 mmHg per 10 µm of corneal thinning. DCT or ORA-derived IOPcc are more reliable in this population.
21. Quick Reference - How Each Tonometer Works (One Sentence Each)
- Schiotz: A known weight is placed on the cornea; how far it sinks in (scale reading) is converted to IOP.
- Goldmann: A variable force is applied to flatten exactly 3.06 mm of cornea; the force needed = IOP (Imbert-Fick).
- Perkins: Same as Goldmann but hand-held for portable use.
- Air-puff/NCT: A jet of air flattens the cornea; time to applanation ∝ IOP; no contact needed.
- Tono-Pen: A strain-gauge probe averages multiple light touch measurements on the cornea.
- iCare (rebound): A magnetized probe bounces off the cornea; faster deceleration = higher IOP.
- DCT (PASCAL): A contour-matching pressure sensor sits on the cornea without flattening it; reads IOP independently of corneal biomechanics.
- ORA: Air jet applied and released; measures IOP at both inward and outward applanation; the difference = corneal hysteresis.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed. | Guyton & Hall Textbook of Medical Physiology | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Pfenninger & Fowler's Procedures for Primary Care | PubMed: PMID 36966883, 38722193, 39303763, 38391624, 36260093, 40599256, 41950306, 38707205
This is a shared conversation. Sign in to Orris to start your own chat.