Diagnostic and therapeutic laparoscopy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, detailed response.
Diagnostic and Therapeutic Laparoscopy
1. Definition and Overview
Laparoscopy is a minimally invasive surgical technique that allows direct visual inspection of the abdominal and pelvic cavity using a laparoscope introduced through small abdominal incisions. It may serve three distinct roles:
-
Screening laparoscopy: rules out peritoneal penetration (e.g., in trauma)
-
Diagnostic laparoscopy: identifies injury or disease to viscera without therapeutic intent
-
Therapeutic (operative) laparoscopy: uses laparoscopic instruments to treat the identified condition
-
Bailey and Love's Short Practice of Surgery, 28th Ed.
2. Historical Background
Diagnostic laparoscopy is not a new innovation. Other specialists (particularly gynecologists) utilized this operative intervention for several decades before it was formally introduced as a procedure of choice for torso wounds. Ivatury et al. performed a critical evaluation of laparoscopy in penetrating abdominal trauma, and Fabian et al. reported on its efficacy in a prospective analysis. Its role has since expanded dramatically across general surgery, gynecology, urology, oncology, and gastroenterology.
- Maingot's Abdominal Operations
3. Physiology of Pneumoperitoneum
The unique feature of laparoscopic surgery is the need to lift the abdominal wall away from abdominal organs. Two methods exist: pneumoperitoneum (gas insufflation) and abdominal wall lift devices.
3.1 Choice of Insufflation Gas
| Gas | Advantages | Disadvantages |
|---|---|---|
| CO2 | Most widely used; rapidly absorbed | Respiratory acidosis, hypercarbia, cardiovascular effects |
| N2O | Physiologically inert, rapidly absorbed; better analgesia under local anesthesia; reduces intraoperative end-tidal CO2 | Unknown effect on tumor biology / port-site metastasis; safety in pregnancy not established |
| Inert gases (He, Ne, Ar) | No metabolic effects | Poorly soluble - prone to gas emboli |
| Air | Historical use | N2 poorly soluble, slowly absorbed; painful |
CO2 is the standard agent. Intraperitoneal pressure of 10-12 mmHg is considered optimal. In cardiopulmonary compromise, lower pressures should be used.
- Schwartz's Principles of Surgery, 11th Ed.; Maingot's Abdominal Operations
3.2 Local and Systemic Effects of CO2 Pneumoperitoneum
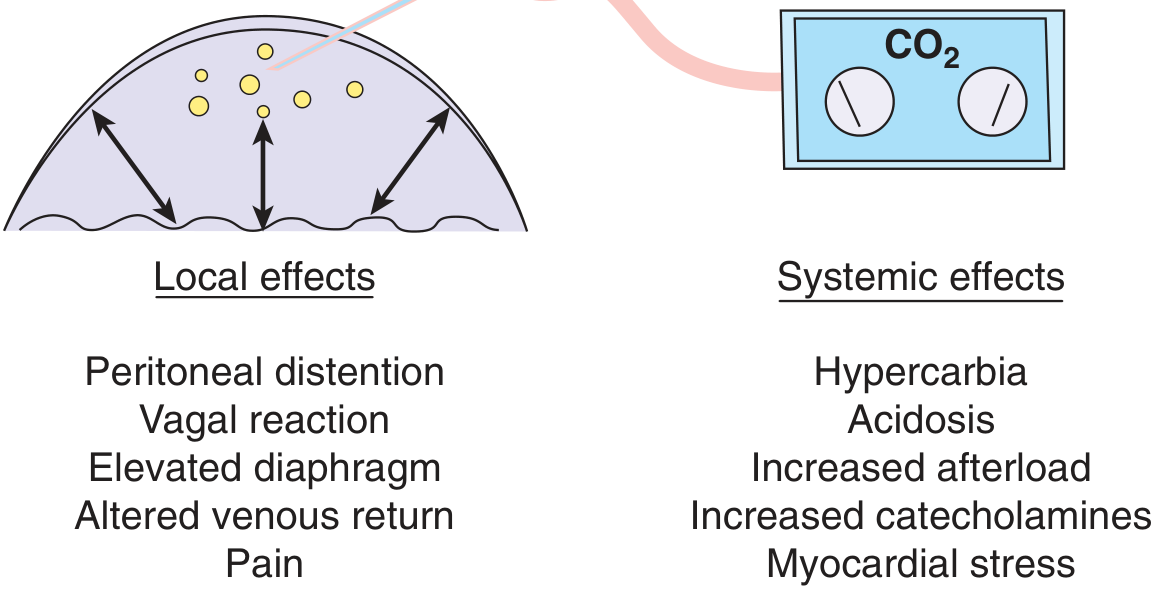
Figure: CO2 gas insufflated into the peritoneal cavity has both local and systemic effects that cause a complex set of hemodynamic and metabolic alterations (Schwartz's).
Gas-specific (CO2) effects:
- Absorbed rapidly across the peritoneal membrane into the circulation
- Generates carbonic acid → respiratory acidosis
- Body buffers (largest reserve in bone) absorb up to 120 L CO2
- Once buffers saturate, respiratory system must compensate (increased ventilatory rate or tidal volume)
- Severe hypercarbia → cardiac arrhythmias
- Tachycardia, increased SVR, elevated blood pressure, increased myocardial O2 demand
Pressure-specific effects:
- Compression of the inferior vena cava → diminished venous return from lower extremities
- Venous engorgement → promotes DVT/PE risk (especially in prolonged operations)
- Increased intra-abdominal pressure transmitted through diaphragm → increased intrathoracic pressure, increased CVP, increased peak inspiratory pressure, risk of barotrauma
- Decreased renal blood flow, GFR, and urine output (mediated by direct pressure and activation of renin-angiotensin-ADH axis); oliguria can persist up to 1 hour post-procedure
- Intraoperative oliguria does NOT reflect intravascular volume status - IV fluids should not be guided by urine output during laparoscopy
Important: If intra-abdominal pressure is kept under 20 mmHg, cardiac output is usually well maintained.
Gas embolism:
- Rare but serious complication
- Suspect if hypotension develops during insufflation
- Diagnosis: characteristic "mill wheel" murmur on esophageal stethoscope
- Treatment: left lateral decubitus, head-down position (traps gas in apex of right ventricle) + central venous catheter aspiration
Endocrine/immune response:
-
Serum cortisol often higher after laparoscopic than open operations (intuitively unexpected)
-
However, stress-mediated hormone levels equilibrate more rapidly post-laparoscopy
-
Immune suppression is less after laparoscopy; faster normalization of cytokine levels
-
Schwartz's Principles of Surgery, 11th Ed.
4. Indications
4.1 Diagnostic Laparoscopy
| Clinical Setting | Role |
|---|---|
| Acute abdomen (appendicitis, acute pelvic pain) | Direct visualization of appendix and pelvic organs; identifies gynecologic causes of pain (48-73% of women with a normal appendix at laparoscopy have a gynecologic cause) |
| Equivocal imaging | CT/US inconclusive - laparoscopy as adjunct |
| Chronic pelvic pain / endometriosis | Gold standard for diagnosis; lesions should be excised for biopsy |
| Infertility evaluation | Assess fallopian tubes, ovaries, pelvic adhesions |
| Penetrating thoracoabdominal trauma (hemodynamically stable) | Diagnose diaphragmatic laceration (no other tool can exclude it), peritoneal penetration |
| Blunt abdominal trauma (hemodynamically stable) | Diagnose occult bowel, mesenteric, or diaphragmatic injuries missed by CT |
| Oncologic staging | Liver, peritoneal cavity, lymph node assessment; staging laparoscopy for gastric, pancreatic, hepatobiliary, colorectal cancers |
| Ascites / liver disease | Direct inspection + guided biopsy |
| Ectopic pregnancy | Accurate diagnosis and simultaneous treatment |
Note: Laparoscopy has no place in the hemodynamically unstable patient. Laparotomy remains standard for abdominal exploration in hemodynamic instability. - Bailey and Love's; Current Surgical Therapy 14e
Compared to CT:
-
Most studies of diagnostic laparoscopy are performed under general anesthesia, making it resource-intensive compared to imaging
-
Under local anesthesia, incomplete pelvic visualization occurs in up to 15% of cases
-
Currently, diagnostic laparoscopy should supplement, not replace, CT as first-line investigation
-
In trauma, diagnostic laparoscopy has been reported to reduce non-therapeutic laparotomy rates by up to 73% in select patients
-
Sleisenger and Fordtran's GI and Liver Disease; Current Surgical Therapy 14e; Maingot's Abdominal Operations
4.2 Therapeutic Laparoscopy
Common therapeutic laparoscopic procedures include:
General Surgery:
- Cholecystectomy (most common)
- Appendectomy
- Inguinal / incisional hernia repair
- Bowel resection (colectomy, Hartmann's, anterior resection)
- Nissen fundoplication / Heller myotomy
- Bariatric surgery (gastric bypass, sleeve gastrectomy)
- Splenectomy / adrenalectomy / nephrectomy
- Peritoneal washings and adhesiolysis
Trauma:
- Repair of diaphragmatic lacerations
- Control of solid organ / mesenteric hemorrhage (selected stable patients)
- ICG fluorescence to assess bowel perfusion following mesenteric lacerations
Gynecology:
- Tubal sterilization (bipolar coagulation, Falope ring, Hulka clip, Filshie clip)
- Salpingectomy / salpingo-oophorectomy for ectopic pregnancy or ovarian pathology
- Ovarian cystectomy; management of ovarian torsion (detorsion ± cystectomy)
- Treatment of endometriosis (excision or electrocoagulation of implants)
- Lysis of pelvic adhesions
- Laparoscopic hysterectomy (total laparoscopic or laparoscopically assisted vaginal)
- LUNA (laparoscopic uterosacral nerve ablation) - though evidence does not support it over laparoscopy alone for CPP
Oncology:
-
Staging laparoscopy (gastric, pancreatic, hepatobiliary, colorectal cancers)
-
Laparoscopic lymph node dissection
-
Excision/biopsy of peritoneal/hepatic lesions
-
Berek & Novak's Gynecology; Bailey & Love's; Schwartz's
5. Contraindications
Absolute Contraindications
- Hemodynamic instability
- Uncorrectable coagulopathy
- Known or suspected abdominal aortic aneurysm (relative)
- Intestinal obstruction with massive distension (relative)
Relative Contraindications
-
Prior multiple abdominal surgeries (extensive adhesions)
-
Obesity (technically challenging; increased pneumoperitoneum effects)
-
Advanced cardiopulmonary compromise (pressure-specific effects poorly tolerated)
-
Pregnancy (first and third trimester - relative; second trimester generally preferred)
-
Suspected malignancy where laparoscopic extraction risks spillage
-
Schwartz's Principles of Surgery; Berek & Novak's Gynecology
6. Equipment
Standard equipment for laparoscopy:
-
Laparoscope: 5 or 10 mm, typically 30° angled telescope (provides better visualization than 0°)
-
Trocars/ports: 5 mm, 10-12 mm sizes depending on procedure
-
Insufflator: delivers CO2 to maintain pneumoperitoneum
-
Camera system: HD or 4K video with monitor
-
Light source: high-intensity xenon or LED
-
Working instruments: Maryland dissector, blunt-tip forceps, cup/biopsy forceps, atraumatic graspers, liver retractors, scissors, suction/irrigation device
-
Electrosurgical unit: monopolar and bipolar electrocautery, harmonic scalpel
-
Laparoscopic ultrasound (LUS) probe: optional, for hepatic/oncologic assessment
-
ICG fluorescence system: for perfusion assessment
-
Maingot's Abdominal Operations; Berek & Novak's Gynecology
7. Technique
7.1 Patient Preparation
- General anesthesia is standard; local anesthesia with conscious sedation possible for select procedures
- Trendelenburg position for pelvic procedures; reverse Trendelenburg for upper abdominal operations
- DVT prophylaxis: sequential compression stockings, subcutaneous or LMWH heparin (especially for prolonged procedures)
- Bowel/bladder decompression (Foley catheter, NGT as needed)
7.2 Peritoneal Access / Port Entry
Two fundamental entry strategies:
1. Closed Entry (Veress Needle technique):
- A spring-loaded Veress needle is inserted (typically at the infraumbilical crease, or Palmer's point - LUQ in cases of previous midline surgery)
- Insufflation begins at low flow rate until peritoneal entry is confirmed
- After establishing pneumoperitoneum (~12 mmHg), trocars are inserted
- Risk: visceral or vascular injury if placement is extraperitoneal or directly into vessel
2. Open Entry (Hasson technique):
- Direct cutdown through skin and fascia (minilaparotomy at umbilicus)
- Blunt trocar placed under direct vision
- Safer in patients with previous abdominal surgery, obesity, or when anatomical landmarks are distorted
- Preferred for patients with prior midline incisions
3. Optical/Visual Trocar Entry:
- Combines advantages of both techniques
- Trocar with transparent tip inserted under laparoscopic visualization
- Increasingly accepted as a safe primary insertion method
Port placement is guided by the planned procedure and findings on initial inspection. Ports are generally placed along the planned open incision line.
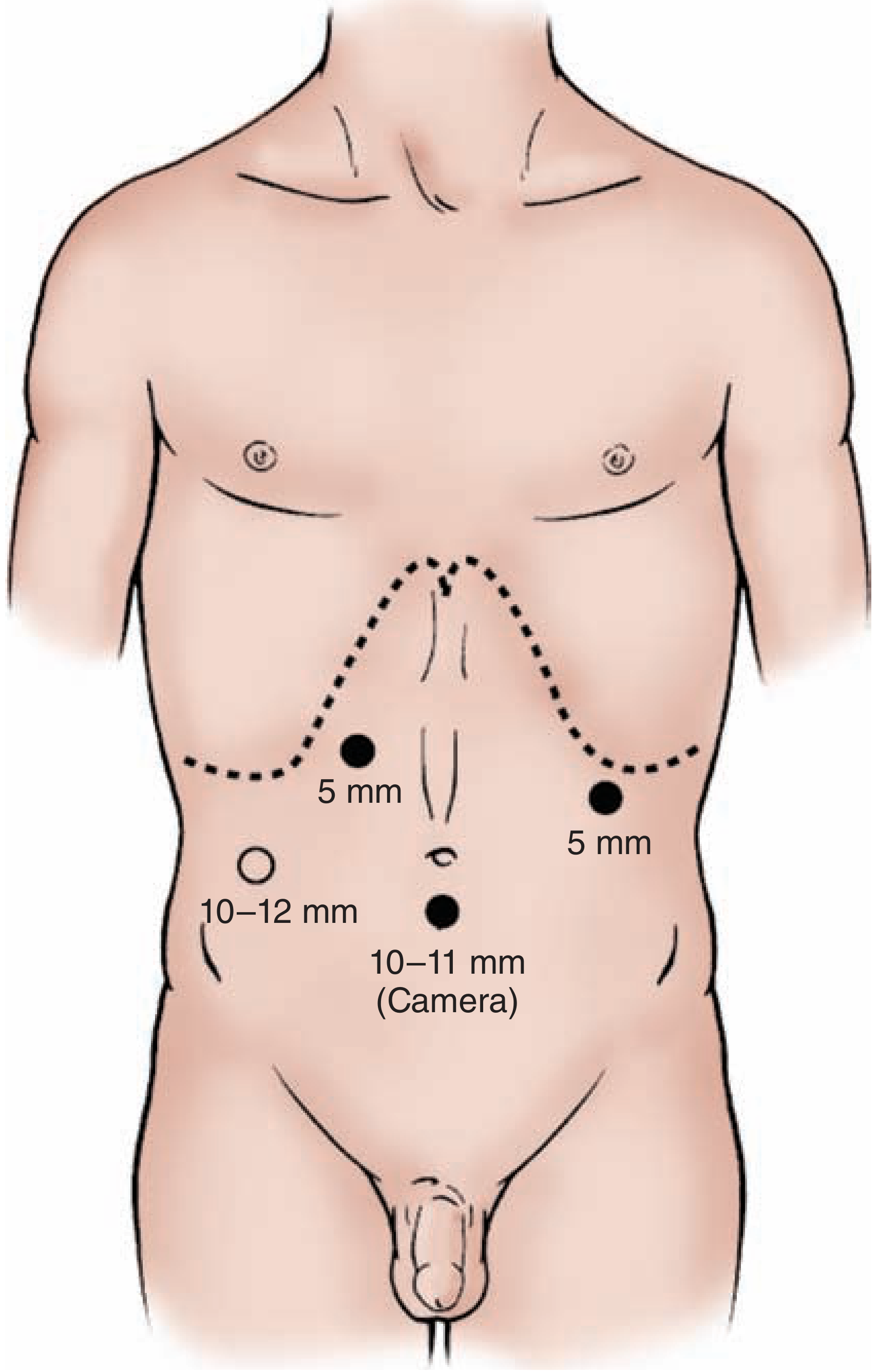
Figure: Typical port placement - 10-11 mm camera port infraumbilically, 5 mm working ports in epigastric and left flank positions, 10-12 mm working port in right iliac fossa (Maingot's Abdominal Operations).
7.3 Systematic Peritoneal Survey
Following port placement, a detailed systematic examination is performed:
- Initial survey of the entire peritoneal cavity
- Liver examination: patient placed in 20° reverse Trendelenburg with 10° left lateral tilt; examine left lateral segment (anterior and posterior), then right lobe (anterior and inferior surfaces)
- Indirect palpation of liver using two instruments (no tactile sensation available)
- Peritoneal surfaces, omentum, bowel, mesentery
- Primary pathology assessed
- Suspicious areas biopsied (cup biopsy forceps preferred; 5-mm biopsy forceps with 2-mm cup)
- Hemostasis with electrocautery or argon beam diathermy
For oncologic staging, assessment includes:
-
Liver surface and parenchyma (IOUS if available)
-
Peritoneal cavity for metastases/carcinomatosis
-
Regional lymph nodes
-
Primary tumor for extent and resectability
-
Peritoneal washings for cytology (particularly in gastric and colorectal cancer)
-
Maingot's Abdominal Operations; Schwartz's Principles of Surgery
8. Special Applications
8.1 Staging Laparoscopy in Cancer
Laparoscopic staging is useful for detecting metastatic disease not visible on CT/MRI, particularly:
- Gastroesophageal junction (GEJ) adenocarcinoma: staging laparoscopy recommended for T3/4 or N+ disease before resection or neoadjuvant therapy; accuracy >90% for identifying peritoneal metastases
- Gastric cancer: identifies peritoneal deposits and liver metastases
- Pancreatic cancer: identifies liver and peritoneal metastases before planned resection
- Hepatocellular carcinoma / biliary cancer (intrahepatic and gallbladder): strongly diagnostic
- Colorectal cancer with hepatic metastases: clinical scoring systems help predict yield
Laparoscopy should be reserved for patients in whom confirmation of metastatic disease that is not otherwise obtainable is essential in deciding on treatment.
- Sabiston Textbook of Surgery; Bailey and Love's; Mulholland and Greenfield's Surgery
8.2 Laparoscopy in Trauma
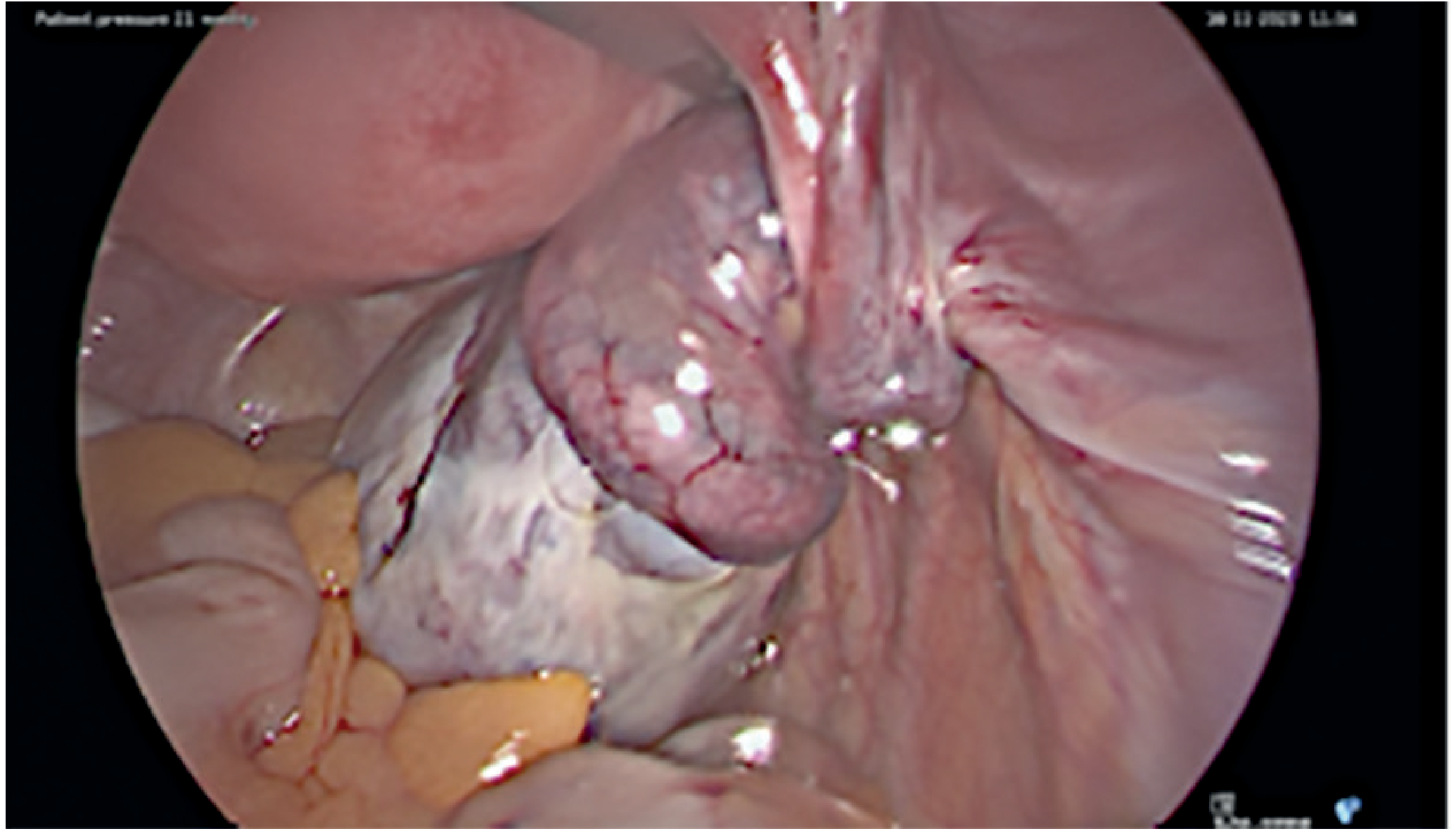
Figure: Laparoscopic image of ovarian torsion - typical appearance with ischemic adnexa (Bailey & Love's).
Indications in trauma (hemodynamically stable only):
- Concern for hollow viscus, mesenteric, or diaphragmatic injury not identified by imaging
- "Seat belt sign" with free fluid but no solid organ injury
- Suspected diaphragmatic laceration (laparoscopy is the study of choice for left thoracoabdominal penetrating wounds - no other modality can exclude diaphragmatic laceration)
- Discordant imaging and clinical findings ("unclear abdomen")
ICG fluorescence can be used intraoperatively to assess bowel perfusion following mesenteric lacerations - ICG is injected IV, binds plasma proteins, and fluoresces under near-infrared light for real-time perfusion imaging.
If injury is identified, the case may be converted to laparotomy, or depending on surgeon skill, repaired with minimally invasive techniques.
- Current Surgical Therapy 14e; Maingot's Abdominal Operations; Bailey and Love's
8.3 Gynecologic Applications
Diagnostic:
- Endometriosis: gold standard diagnosis requires laparoscopic visualization + histologic confirmation (positive histology confirms, but negative does not exclude the diagnosis)
- Chronic pelvic pain evaluation
- Infertility workup (tubal patency - chromopertubation, pelvic anatomy)
- Ectopic pregnancy: both diagnostic and therapeutic (most accurate tool for suspected ectopic)
- Acute pelvic pain / adnexal torsion
Therapeutic:
-
Tubal sterilization techniques:
- Bipolar coagulation: requires ≥25 W into 100-Ω resistance; 3 cm of tube coagulated
- Falope ring (Silastic band): loop of tube pulled into sleeve; ischemic necrosis
- Hulka clip: spring clip across midisthmus at right angles
- Filshie clip: titanium clip with silicone liner; lower pregnancy rate than Hulka clip; now most widely used in UK/Canada
-
Laparoscopic hysterectomy
-
Adhesiolysis (though efficacy for pain relief is uncertain; adhesion reformation is common)
-
LUNA: not more effective than laparoscopy alone for CPP
-
Berek & Novak's Gynecology
9. Advantages Over Open Surgery
| Parameter | Laparoscopy | Open Surgery |
|---|---|---|
| Incision/cosmesis | Small port sites | Large incision |
| Pain | Reduced | Greater |
| Hospital stay | Shorter | Longer |
| Recovery time | Faster | Slower |
| Wound infection | Lower rate | Higher rate |
| Blood loss | Generally less | More |
| Immune suppression | Less | More |
| Insensible losses | Minimal | Significant |
| DVT risk (prolonged) | Present (venous stasis) | Present |
| Tactile feedback | Absent | Present |
Robotic assistance has not been shown to have clinical, cost, or cosmetic advantages over conventional laparoscopic surgery. Available evidence shows increased cost and no better cosmetic results based on incision location and length. - Berek & Novak's Gynecology
10. Complications
Access-Related
| Complication | Comment |
|---|---|
| Vascular injury | Trocar/Veress needle injury to aorta, IVC, iliac vessels - most serious |
| Bowel injury | During trocar insertion or adhesiolysis |
| Bladder injury | Trocar, especially in previous pelvic surgery |
| Port-site hernia | Risk significantly increases when fascial incision >10 mm; requires fascial closure |
Pneumoperitoneum-Related
| Complication | Comment |
|---|---|
| Hypercarbia / respiratory acidosis | Most common; managed by increasing ventilation |
| CO2 pneumothorax | From diaphragmatic defect; enlarge hole to prevent tension pneumothorax; chest tube ± |
| Gas embolism | Rare; mill wheel murmur; left lateral decubitus + head down + aspiration |
| DVT / PE | Venous stasis from increased IAP; prevent with sequential compression devices + heparin |
| Subcutaneous emphysema | Extraperitoneal gas tracking |
| Cardiac arrhythmias | Severe hypercarbia; vagal reaction during insufflation |
| Oliguria | Common intraoperatively; not a guide to fluid resuscitation |
Electrosurgery-Related
- Unintended injury from monopolar current spread (capacitive coupling, direct coupling)
- Thermal injuries to bowel, ureter, bile duct may present delayed (12-72 hours)
- Reduction strategies: bipolar or harmonic devices, remove instruments when not activated, understand electrosurgical principles
Port-Site Metastasis
-
Rare but recognized complication in cancer surgery
-
Mechanism not fully understood; CO2 pneumoperitoneum effects on tumor biology under investigation with alternative gases
-
Schwartz's Principles of Surgery; Berek & Novak's Gynecology; Maingot's Abdominal Operations
11. Conversion to Open Surgery
Patients should be counseled about the possibility of conversion to laparotomy. Indications for conversion include:
- Hemodynamic instability
- Uncontrollable hemorrhage
- Inadequate visualization
- Dense adhesions precluding safe dissection
- Injury requiring open repair
- Equipment failure
Conversion is not a complication but a sound surgical judgment decision.
12. Contraindications to Laparoscopy in Specific Scenarios
- Ovarian malignancy strongly suspected: laparotomy preferred to avoid spillage
- Laparoscopic cancer surgery: caution with N2O (unknown effect on tumor biology / port-site metastasis)
- Large uterine/fibroid size: may preclude laparoscopic hysterectomy
- Extensive adhesions from previous surgery: open approach may be safer
Summary
Laparoscopy is a fundamental tool in modern surgery spanning all surgical subspecialties. Its diagnostic role allows direct visualization and tissue biopsy with minimal morbidity; its therapeutic role replaces open surgery for most elective and many urgent/emergency abdominal operations. The physiology of CO2 pneumoperitoneum underlies its limitations in cardiopulmonary compromise, and complications - though less frequent than open surgery - require a thorough understanding to prevent and manage. Entry technique, systematic peritoneal survey, and appropriate patient selection determine the safety and success of the procedure.
Key references:
- Schwartz's Principles of Surgery, 11th Ed., Chapter 14 (Minimally Invasive Surgery)
- Maingot's Abdominal Operations, Chapter 5 (Staging Laparoscopy)
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapters 29 & 66
- Berek & Novak's Gynecology (Diagnostic and Operative Laparoscopy)
- Current Surgical Therapy 14e (Laparoscopy in Blunt Abdominal Trauma)
- Sleisenger and Fordtran's GI and Liver Disease (Diagnostic Laparoscopy in Appendicitis)
- Sabiston Textbook of Surgery (Role of Diagnostic/Staging Laparoscopy in Cancer)
This is a shared conversation. Sign in to Orris to start your own chat.