Give answered for each objective
Reading File
Running Command
cd /home/daytona/workspace/attachments/94570764-59d6-48f9-b052-35b5ed3daace/ && python3 -c " import pdfplumber with pdfplumber.open('CH Tutorial - Epilepsy_685813b8-71b6-4023-8819-1f6fc480752a.pdf') as pdf: print(f'Total pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): text = page.extract_text() print(f'--- PAGE {i+1} ---') print(text) print() "
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
I now have sufficient information from the case and textbooks to answer all 6 learning objectives thoroughly. Let me compose the full detailed answers.
Answers to All Learning Objectives - Epilepsy Tutorial (Camille Mendoza, 7-year-old)
Objective 1 - Apply the ILAE Operational Definition of Epilepsy and the 2017 ILAE Seizure Classification
Does Camille meet the ILAE operational definition of epilepsy?
The ILAE 2017 operational definition requires at least two unprovoked seizures occurring more than 24 hours apart, OR one unprovoked seizure with a probability of further seizures ≥60%, OR diagnosis of an epilepsy syndrome.
Camille has had multiple unprovoked seizure-like episodes occurring many times a day for four months - far exceeding the minimum threshold of two unprovoked seizures. She therefore meets the operational definition of epilepsy.
Seizure type (2017 ILAE classification):
Using the 2017 ILAE framework, seizures are first classified by onset (focal, generalized, or unknown), then by awareness/motor features.
Camille's episodes are:
- Sudden onset and offset - no warning, resumes mid-sentence
- Bilateral from the start (no focal aura, no unilateral motor activity)
- Brief lapse of consciousness (behavior arrest) with bilateral automatisms (eyelid flutter, lip-smacking, picking)
- No postictal confusion
- EEG shows bilaterally synchronous, symmetric, generalized 3-Hz spike-and-wave discharges
Classification:
- Seizure type: Generalized onset, non-motor (absence) - typical absence seizures
- Epilepsy type: Generalized epilepsy
- Epilepsy syndrome: Childhood Absence Epilepsy (CAE)
CAE is defined by onset ages 4-10 years, frequent typical absence seizures, normal development, normal interictal EEG background, and characteristic 3-Hz generalized spike-and-wave on EEG, provoked by hyperventilation. Camille fulfills all these criteria.
(Harrison's Principles of Internal Medicine 22E, Generalized Onset Seizures)
Objective 2 - Differentiate Absence Seizures from Clinical Mimics
Mimics to consider for Camille:
| Feature | Absence Seizures (Camille) | ADHD / Daydreaming | Focal Impaired Awareness (complex partial) | Syncope |
|---|---|---|---|---|
| Duration | 5-10 seconds | Variable (minutes) | 30 sec - 3 min | Seconds (with prodrome) |
| Frequency | Many times/day | Continuous inattention | Usually <5/day | Occasional |
| Onset/offset | Abrupt, no warning | Gradual | May have aura | Pre-syncopal prodrome |
| Postictal state | None - resumes mid-sentence | N/A | Confusion, fatigue (minutes to hours) | Brief confusion, pallor |
| Automatisms | Present (subtle: eyelid flutter, lip-smack, picking) | Absent | Present but more prominent, purposeful | Absent |
| Hyperventilation provocation | YES - classic | No | No | May cause syncope |
| EEG | 3-Hz generalized spike-wave | Normal | Focal temporal discharge | Normal |
| Motor/fall | No fall, no jerking | N/A | May have dystonic posturing, head turning | Falls (flaccid) |
Key discriminating features in Camille:
-
Abrupt onset and offset with immediate resumption - she finishes the sentence she started. This is pathognomonic of absence. In ADHD or daydreaming, the child re-orients slowly and cannot immediately resume; in focal impaired awareness seizures, there is a postictal confusion phase of minutes.
-
Bedside hyperventilation provocation - 3 minutes of hyperventilation reproduced a typical episode (8-second stare, eyelid flutter, behavior arrest). This is a bedside test with ~80% sensitivity for CAE. ADHD, daydreaming, and focal seizures are not triggered by hyperventilation.
-
Frequency - many episodes per day is typical of CAE. Focal/temporal lobe seizures rarely exceed 3-5/day.
-
No postictal state - rules out focal impaired awareness seizures and tonic-clonic events.
-
Automatisms are present but subtle - eyelid myoclonia (flutter) and oral automatisms (lip-smacking) are typical of absence. Prominent purposeful automatisms suggest focal temporal lobe origin.
(Harrison's 22E; Kaplan & Sadock's Comprehensive Textbook of Psychiatry, "Attention-Deficit Hyperactivity Disorder and Sorting Out Staring Spells")
Objective 3 - Evaluate Indications for, and Limits of, Investigations
EEG (Electroencephalography)
Indication: Required - EEG is the single most important investigation in suspected epilepsy. In Camille, the EEG with hyperventilation and photic stimulation:
- Confirmed generalized 3-Hz spike-and-wave discharges provoked by hyperventilation
- Normal interictal background (rules out encephalopathy)
- No focal slowing (rules out structural lesion)
- No photoparoxysmal response (rules out juvenile myoclonic epilepsy subtype)
Limits: A routine inter-ictal EEG can be normal in up to 50% of epilepsy cases overall (though much less so in CAE where hyperventilation nearly always provokes discharges). A negative EEG does not exclude epilepsy; conversely, epileptiform discharges can occur in non-epileptic individuals (~2% of healthy children).
Laboratory Studies
Indicated in Camille: Blood glucose at time of episode (92 mg/dL - normal, rules out hypoglycemia as cause), electrolytes (Na, K, Ca, Mg - all normal, rules out metabolic seizure triggers), CBC (normal), LFTs (baseline before starting valproate/ethosuximide, which can cause hepatotoxicity). ECG with QTc (baseline, especially important before some ASMs and rules out long QT as a cause of staring/syncope - QTc 410 ms, normal).
Limits: Routine metabolic work-up is low yield in an otherwise healthy child with a clinically and EEG-confirmed epilepsy syndrome (CAE). These tests are done to exclude metabolic mimics and establish a safe baseline for treatment, not to diagnose CAE.
Not required: Genetic testing is not routinely indicated for straightforward CAE, though CACNA1A, GABRG2, GABRA1 variants are known.
Neuroimaging (MRI Brain)
Not required in Camille - She has:
- Normal neurological exam
- Normal development
- EEG pattern consistent with a genetic/idiopathic generalized epilepsy (no focal slowing or asymmetry)
- Clinical picture that fits CAE exactly
MRI is indicated when there is: focal neurological signs, focal EEG abnormality, refractory epilepsy, age of onset <2 years, or regression in development. MRI is not needed for classic CAE with a typical EEG.
(Harrison's 22E; Adams and Victor's Principles of Neurology 12th Ed)
Objective 4 - Evidence-Based Antiseizure Medication (ASM) Plan for CAE + Why Sodium Channel Blockers Aggravate Generalized Seizures
First-line treatment for CAE:
The preferred first-line agents for CAE are:
-
Ethosuximide - drug of choice for pure absence (no generalized tonic-clonic seizures). The landmark CHILD study (2010, NEJM) showed ethosuximide achieved seizure freedom in ~53% of children and was superior to lamotrigine, with comparable efficacy to valproate but significantly fewer attentional side effects than valproate.
-
Sodium valproate (valproic acid) - effective for both absence and generalized tonic-clonic seizures. Preferred if GTC seizures co-exist. Requires LFT and CBC monitoring; teratogenic - not preferred in adolescent females without discussion. Camille's normal baseline LFTs support safe initiation if used.
-
Lamotrigine - second-line; effective but slower titration required. Less effective than ethosuximide for pure absence.
For Camille: Ethosuximide is the drug of choice. She has pure absence without GTC seizures, normal LFTs, and is a young girl (valproate teratogenicity concerns, though less pressing now). Ethosuximide works by blocking T-type calcium channels in thalamic neurons, interrupting the thalamocortical oscillations responsible for 3-Hz spike-wave discharges.
Why sodium channel-blocking agents aggravate generalized seizures:
Drugs such as carbamazepine, oxcarbazepine, phenytoin, lamotrigine (to a lesser extent), and vigabatrin work primarily by blocking voltage-gated sodium channels. This mechanism:
- Reduces neuronal excitability by prolonging the inactivated state of Na+ channels (use-dependent block)
- Is effective against focal seizures and focal-to-bilateral tonic-clonic seizures
However, in idiopathic generalized epilepsies (like CAE), the ictal mechanism is a thalamocortical oscillation driven by T-type calcium channels and GABA-mediated inhibition, NOT by excessive Na+ channel activity. Sodium channel blockers may:
- Paradoxically increase absence seizure frequency - possibly by disrupting inhibitory interneuron function or facilitating the thalamic pacemaker rhythm
- Carbamazepine is well-documented to precipitate or worsen absence, myoclonic, and atonic seizures in genetic generalized epilepsies
- Vigabatrin (GABA-T inhibitor) can also worsen absence
This is why choosing ASMs in epilepsy requires knowing the seizure type and epilepsy syndrome first - the wrong drug can cause harm.
(Adams & Victor's Principles of Neurology 12th Ed; Neuroanatomy through Clinical Cases 3rd Ed; Harrison's 22E)
Objective 5 - Time-Based Algorithm for Acute Management of Prolonged Convulsive Seizure and Convulsive Status Epilepticus (CSE) in a Child
While Camille's current episodes are brief and self-terminating absence seizures (no acute management needed), this objective asks about the general management of CSE. If she were to develop a prolonged convulsive seizure:
Definition: Convulsive status epilepticus (CSE) = continuous convulsive seizure lasting ≥5 minutes, OR two or more seizures without recovery of consciousness between them.
Time-based algorithm:
| Time | Action |
|---|---|
| 0-5 min (Pre-hospital / early) | Position child safely (lateral recovery position), protect airway, do not restrain or put anything in mouth, time the seizure, call for help. If rectal diazepam / intranasal/buccal midazolam available (prescribed rescue medication), administer now. |
| 5-10 min (Emergency - IV/IO access) | Secure IV or intraosseous access. Check blood glucose (treat hypoglycemia if present with dextrose). First-line benzodiazepine: Lorazepam 0.1 mg/kg IV (max 4 mg), OR Diazepam 0.2 mg/kg IV (max 10 mg), OR Midazolam 0.2 mg/kg IM/intranasal (max 10 mg). Monitor: pulse oximetry, BP, ECG. |
| 10-20 min (If still seizing after 1st benzodiazepine) | Repeat benzodiazepine once (same dose). Continue monitoring. Consider cause: meningitis, metabolic, trauma, drug toxicity. |
| 20-40 min (Established CSE - 2nd line) | Add a non-benzodiazepine ASM: Levetiracetam 60 mg/kg IV (max 4.5 g) over 15 min, OR Fosphenytoin 20 mg PE/kg IV over 15 min (with cardiac monitoring), OR Valproate 40 mg/kg IV over 15 min. |
| 40-60 min (Refractory CSE) | Intubation and general anesthesia with: Midazolam infusion, Propofol infusion (avoid in young children), or Thiopental/Phenobarbital infusion. ICU admission. Continuous EEG monitoring. |
Key points:
- The single most important intervention is giving the first benzodiazepine early - delays worsen outcome exponentially
- IV lorazepam is preferred if access available; IM or intranasal midazolam is equivalent and faster when IV access is delayed (especially in out-of-hospital setting)
- Avoid phenytoin as first-line in known idiopathic generalized epilepsy (sodium channel blocker - see Objective 4)
- Treat the underlying cause (hypoglycemia, electrolyte abnormality, infection)
(ROSEN's Emergency Medicine; Harrison's 22E; The Harriet Lane Handbook 23rd Ed)
Objective 6 - Long-Term Care of a Child with Epilepsy
Adherence:
- Explain to Camille's mother the importance of daily medication without missing doses - breakthrough seizures from non-adherence are the leading preventable cause of morbidity
- Use a pill organizer or alarm; link dosing to a daily routine (breakfast/dinner)
- Address financial concerns directly: ethosuximide is inexpensive and available as generic; social work referral for medication subsidy programs
Safety and Lifestyle Counseling:
- Bathing: Supervision while bathing; prefer showers over baths. No unsupervised swimming
- Heights: Supervision near stairs, elevated play structures
- Cycling: Should wear helmet; can cycle once seizure-free for a defined period
- Sleep: Adequate sleep is essential - sleep deprivation lowers seizure threshold in many epilepsy syndromes (less of a trigger in CAE specifically, but boredom/fatigue were noted triggers in Camille)
- Screen time and photic stimulation: Camille's EEG showed no photoparoxysmal response, so photosensitivity is not a concern for her specifically
School and Psychosocial Impact:
- Camille's grades have dropped significantly - this is partly from seizure-related cognitive disruption (brief lapses many times/day prevent sustained learning), and partly from the known neurocognitive effects of CAE itself (attention problems)
- Write a school letter explaining absence epilepsy; teacher should know to not punish or single out episodes
- Neuropsychological assessment if learning difficulties persist after seizure control
- Address potential bullying or stigma
Comorbidities:
- CAE carries a 23% rate of psychiatric comorbidity (Kaplan & Sadock's Comprehensive Textbook)
- ADHD-like attention problems are common and may persist even after seizure control (especially with valproate - another reason to prefer ethosuximide in CAE)
- Screen regularly for anxiety and depression
- Monitor for juvenile absence epilepsy (JAE) or juvenile myoclonic epilepsy (JME) features as adolescence approaches
Medication Withdrawal:
- CAE has a favorable prognosis: ~70-80% of children with CAE achieve remission by mid-adolescence
- Consider ASM withdrawal after 2 years of seizure freedom, ideally before the child enters adolescence
- Requires a normal EEG before tapering; taper slowly over 3-6 months
- Family counsels about driving restrictions that apply during taper and after any breakthrough seizures
Prognosis:
- Camille's prognosis is good: she has classic CAE, normal development, normal MRI (not done but not expected to be abnormal), normal interictal EEG background, and response to hyperventilation provocation (a good prognostic sign)
- A maternal aunt with childhood seizures that resolved in her teens is consistent with an autosomal dominant/polygenic inheritance pattern common in genetic generalized epilepsies
- Approximately 70-80% remission rate before adulthood; roughly 10-15% develop JME or persistent absence (which requires lifelong treatment)
- Monitor closely around puberty for phenotype evolution
(Harrison's 22E; Kaplan & Sadock's Comprehensive Textbook; Adams & Victor's Principles of Neurology 12th Ed; The Harriet Lane Handbook 23rd Ed)
Summary for Camille:
Camille has Childhood Absence Epilepsy (CAE) - a genetic generalized epilepsy with typical absence seizures (generalized onset, non-motor/absence, per ILAE 2017 classification). Her EEG (generalized 3-Hz spike-wave provoked by hyperventilation) and clinical picture are diagnostic. She should be started on ethosuximide as first-line treatment. Sodium channel blockers (carbamazepine, phenytoin) are contraindicated in her. The family requires thorough counseling on adherence, school support, safety, and the favorable prognosis with high likelihood of remission by adolescence.
Explain first objective
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of Objective 1, built from the textbooks and applied directly to Camille's case.
Objective 1 - ILAE Operational Definition of Epilepsy & 2017 Seizure Classification Applied to Camille
This objective has three layers you need to work through:
- What is the ILAE operational definition of epilepsy?
- What is the 2017 ILAE seizure classification system?
- How do we apply both to Camille to arrive at a diagnosis?
Part A - The ILAE Operational Definition of Epilepsy
A seizure and epilepsy are not the same thing. Harrison's defines a seizure as:
"A transient occurrence of signs or symptoms due to abnormal excessive or synchronous neuronal activity in the brain."
A single seizure does not automatically mean epilepsy. Epilepsy describes a condition where a person has a sustained risk of recurrent seizures from a chronic underlying process.
The ILAE operational definition (Fisher et al., 2014) states epilepsy is diagnosed when any one of these three criteria is met:
| Criterion | What it means |
|---|---|
| 1. At least two unprovoked seizures occurring >24 hours apart | The classic definition - recurrence establishes chronicity |
| 2. One unprovoked seizure + ≥60% probability of further seizures over the next 10 years | e.g., one seizure after a stroke, or with epileptiform EEG - risk is high enough to call it epilepsy |
| 3. Diagnosis of an epilepsy syndrome | e.g., childhood absence epilepsy, West syndrome - where the syndrome itself carries a known recurrence risk |
The word "unprovoked" is key - it means the seizure has no immediate identifiable cause (no fever, no drug toxicity, no metabolic abnormality, no acute brain injury). A provoked seizure (e.g., hypoglycemia, meningitis) does not count toward this definition.
Applied to Camille:
She has had multiple episodes per day for four months - this is far beyond the minimum of two unprovoked seizures. Her blood glucose at the time of an episode was normal (92 mg/dL), electrolytes were all normal, no fever, no infection, no head trauma. These seizures are unprovoked. She meets Criterion 1 conclusively, and also Criterion 3 (once we identify the syndrome).
Part B - The 2017 ILAE Seizure Classification
The previous system (1981) used the terms "simple partial" and "complex partial." The 2017 revision replaced this entirely. Here is the classification framework:
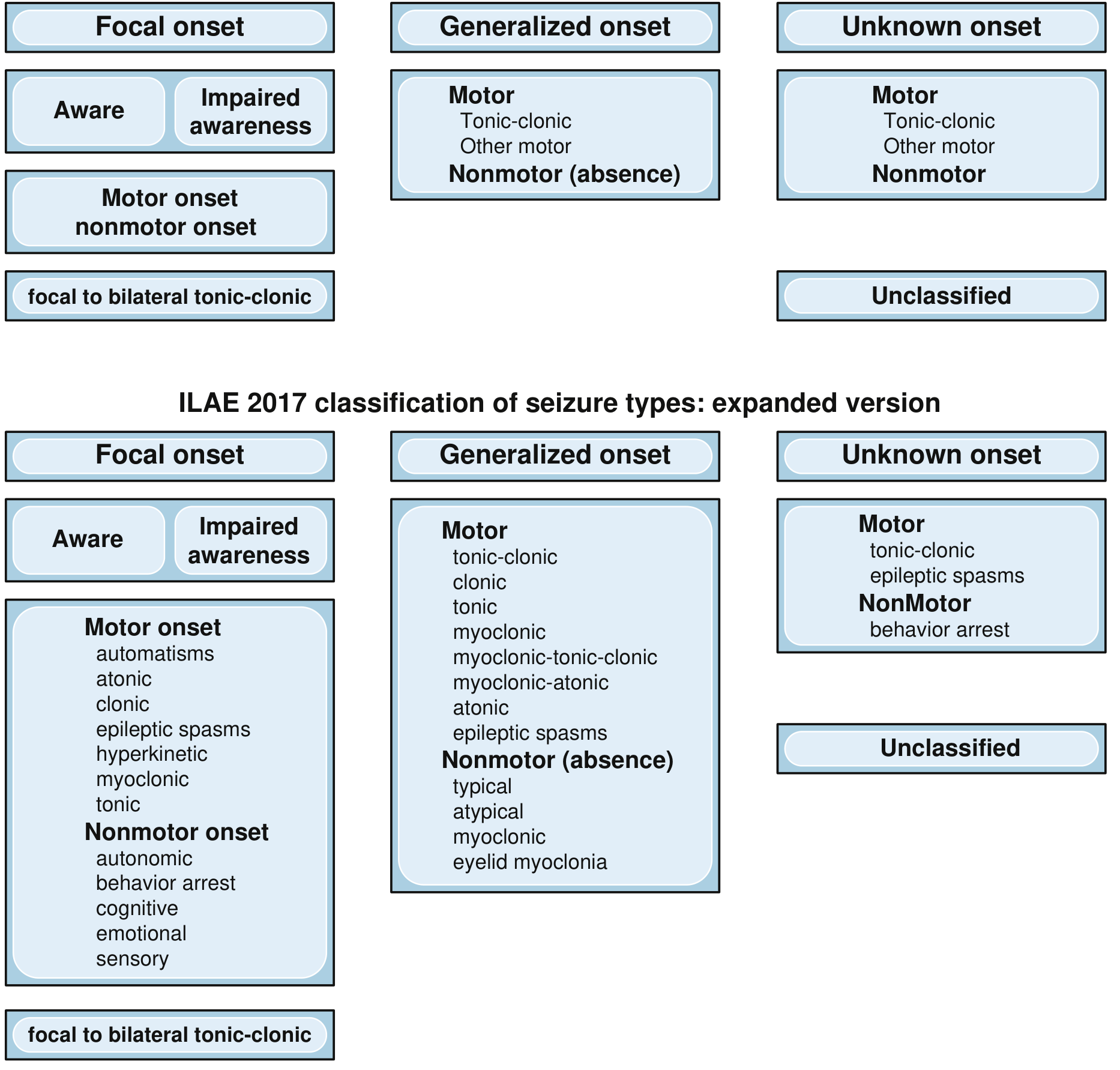
The classification works in a step-wise manner, asking three questions in order:
Step 1 - Where did the seizure start? (Onset)
- Focal onset - originates within networks limited to ONE hemisphere (was called "partial")
- Generalized onset - originates at some point but immediately and rapidly engages networks in BOTH hemispheres simultaneously
- Unknown onset - onset cannot be determined
Step 2 - For focal seizures: Is awareness intact or impaired?
- Focal aware (was "simple partial") - patient remains fully conscious and responsive
- Focal impaired awareness (was "complex partial") - any alteration in awareness during any part of the seizure
Step 3 - What is the nature of the seizure? (Motor or Nonmotor)
For Generalized onset seizures, the main subtypes are:
- Motor: tonic-clonic, clonic, tonic, myoclonic, atonic, epileptic spasms
- Nonmotor (absence): typical, atypical, myoclonic absence, eyelid myoclonia
This 3-level structure then feeds into a higher classification of the epilepsy itself:
| Level | Camille's answer |
|---|---|
| Seizure type | Generalized onset, nonmotor (absence) - typical |
| Epilepsy type | Generalized epilepsy |
| Epilepsy syndrome | Childhood Absence Epilepsy (CAE) |
| Etiology | Genetic (idiopathic) |
(Harrison's 22E, Table 436-1; Bradley & Daroff's Neurology in Clinical Practice, Fig. 100.3)
Part C - Applying This to Camille Step by Step
Step 1 - Was the onset focal or generalized?
Look at Camille's episode features:
- No aura (no warning, no initial sensory/motor/emotional symptom confined to one body part)
- No head or eye deviation to one side
- No post-ictal confusion or focal weakness
- EEG shows bilaterally synchronous, symmetric, generalized discharges - meaning both hemispheres were engaged from the very beginning
This rules out focal onset. The onset is generalized.
Step 2 - What type of generalized seizure?
She has:
- Sudden lapse of consciousness (behavior arrest) - cannot respond when her name is called
- No tonic stiffening, no clonic jerking, no falling
- Brief duration (5-10 seconds)
- No postictal state - resumes mid-sentence immediately
- Subtle bilateral motor features: eyelid flutter (eyelid myoclonia) and oral automatisms (lip-smacking, chewing movements)
This is a generalized onset, nonmotor (absence) - TYPICAL absence seizure.
The "typical" qualifier is important:
- Typical absence: abrupt onset/offset, brief, generalized 3-Hz spike-wave, normal interictal EEG background, provoked by hyperventilation - this is Camille
- Atypical absence: slower onset/offset, more prolonged, <2.5 Hz spike-wave, usually associated with brain pathology (e.g., Lennox-Gastaut syndrome)
Step 3 - What is the epilepsy type and syndrome?
- Epilepsy type: Generalized epilepsy (both hemispheres involved from the start, consistent EEG pattern)
- Syndrome: Childhood Absence Epilepsy (CAE)
- Age 4-10 years at onset ✓ (Camille is 7)
- Multiple absence seizures per day ✓
- Normal development and neurological exam ✓
- Normal interictal EEG background ✓
- Generalized 3-Hz spike-wave on EEG provoked by hyperventilation ✓
- No other seizure types (no myoclonic, no tonic-clonic) ✓
- Family history of childhood seizures (maternal aunt) ✓ - consistent with genetic basis
- Etiology: Genetic/idiopathic - no structural brain lesion, no metabolic cause
Summary Diagram for Camille
Seizure onset → GENERALIZED (bilateral, symmetric, no aura)
↓
Motor or Nonmotor? → NONMOTOR (no tonic/clonic/myoclonic)
↓
Type? → TYPICAL ABSENCE
↓
Epilepsy type → GENERALIZED EPILEPSY
↓
Syndrome → CHILDHOOD ABSENCE EPILEPSY (CAE)
↓
Etiology → GENETIC
Why does this classification matter clinically? Because the seizure type and epilepsy syndrome directly determine treatment. CAE requires drugs that work on T-type calcium channels (ethosuximide, valproate) - NOT sodium channel blockers like carbamazepine, which would worsen her seizures. Getting the classification right is the foundation for everything that follows in her management.
This is a shared conversation. Sign in to Orris to start your own chat.