notes on ophthalamic division of trigeminal nerve
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Excellent material gathered. Here are comprehensive notes on the ophthalmic division of the trigeminal nerve, compiled from Gray's Anatomy for Students, Scott-Brown's Otorhinolaryngology, Bradley and Daroff's Neurology, and Localization in Clinical Neurology.
Ophthalmic Division of the Trigeminal Nerve (V1)
Overview
The ophthalmic nerve (V1) is the smallest and most superior of the three divisions of the trigeminal nerve. It is a purely sensory nerve - it carries no motor fibers. It arises from the trigeminal (semilunar/Gasserian) ganglion.
Course
- From the trigeminal ganglion, V1 travels forward in the lateral wall of the cavernous sinus, positioned below the oculomotor (III) and trochlear (IV) nerves but above the maxillary nerve (V2).
- Just before entering the orbit, it divides into its three terminal branches.
- It enters the orbit through the superior orbital fissure:
- The frontal and lacrimal nerves pass outside the common tendinous ring.
- The nasociliary nerve passes within the common tendinous ring (between the superior and inferior branches of the oculomotor nerve).
Three Terminal Branches
1. Frontal Nerve (Largest branch)
- Runs between the levator palpebrae superioris and the periorbita on the roof of the orbit.
- Midway across the orbit, divides into two terminal branches:
- Supratrochlear nerve - passes medially above the trochlea; supplies the conjunctiva and skin of the upper eyelid, and the lower medial forehead.
- Supraorbital nerve - the larger terminal branch; exits through the supra-orbital notch; ascends across the forehead and scalp as far back as the middle of the scalp, supplying the upper eyelid, conjunctiva, forehead, and anterior scalp.
2. Lacrimal Nerve (Smallest branch)
- Runs along the upper border of the lateral rectus muscle.
- Receives a branch from the zygomaticotemporal nerve carrying parasympathetic and sympathetic postganglionic fibers for the lacrimal gland (secretomotor fibers).
- Supplies: lacrimal gland, conjunctiva, and the lateral part of the upper eyelid and brow.
3. Nasociliary Nerve (Intermediate in size; most important autonomically)
- Enters the orbit within the common tendinous ring; the first branch from V1.
- Crosses the optic nerve superiorly, passing medially below the superior rectus muscle.
- Gives off several branches:
- Communicating branch to the ciliary ganglion (sensory root of the ciliary ganglion) - sensory fibers pass through the ciliary ganglion without synapsing.
- Long ciliary nerves (2-3) - sensory to the cornea and eyeball; also carry sympathetic fibers for pupillary dilation.
- Posterior ethmoidal nerve - supplies posterior ethmoidal air cells and the sphenoidal sinus.
- Infratrochlear nerve - runs along the medial wall of the orbit; supplies skin of the upper medial eyelid, medial angle of the eye, lacrimal sac, and upper side of the nose.
- Anterior ethmoidal nerve - exits through the anterior ethmoidal foramen into the anterior cranial fossa, crosses the cribriform plate, and exits through a slit in the crista galli into the nasal cavity. Supplies: anterior nasal mucosa, then emerges at the lower nasal bone as the external nasal nerve supplying skin over the tip, alar, and vestibule of the nose.
Sensory Distribution (Summary)
V1 carries sensation from:
- Eyes, conjunctiva, cornea, and orbital contents (including the lacrimal gland)
- Upper eyelid
- Forehead and anterior scalp (to the vertex)
- Dorsum and tip of the nose
- Nasal cavity mucosa, frontal sinus, ethmoidal cells, sphenoidal sinus
- Falx cerebri and dura of the anterior cranial fossa and superior tentorium cerebelli
The Corneal Reflex
- Afferent limb: Nasociliary nerve (V1) - via the long ciliary nerves
- Efferent limb: Facial nerve (VII) - orbicularis oculi
- On testing, the corneal wisp is applied to the lower cornea with the patient looking upward; the ipsilateral eye closes and the opposite eye closes consensually.
- Absence of the corneal reflex is often the first clinical sign of V nerve damage and should be tested in any patient with vertigo, deafness, or facial pain.
- Corneal hypoesthesia occurs in ~45% of diabetic patients; bilateral corneal anesthesia can be the presenting feature of diabetic neuropathy.
Diagram
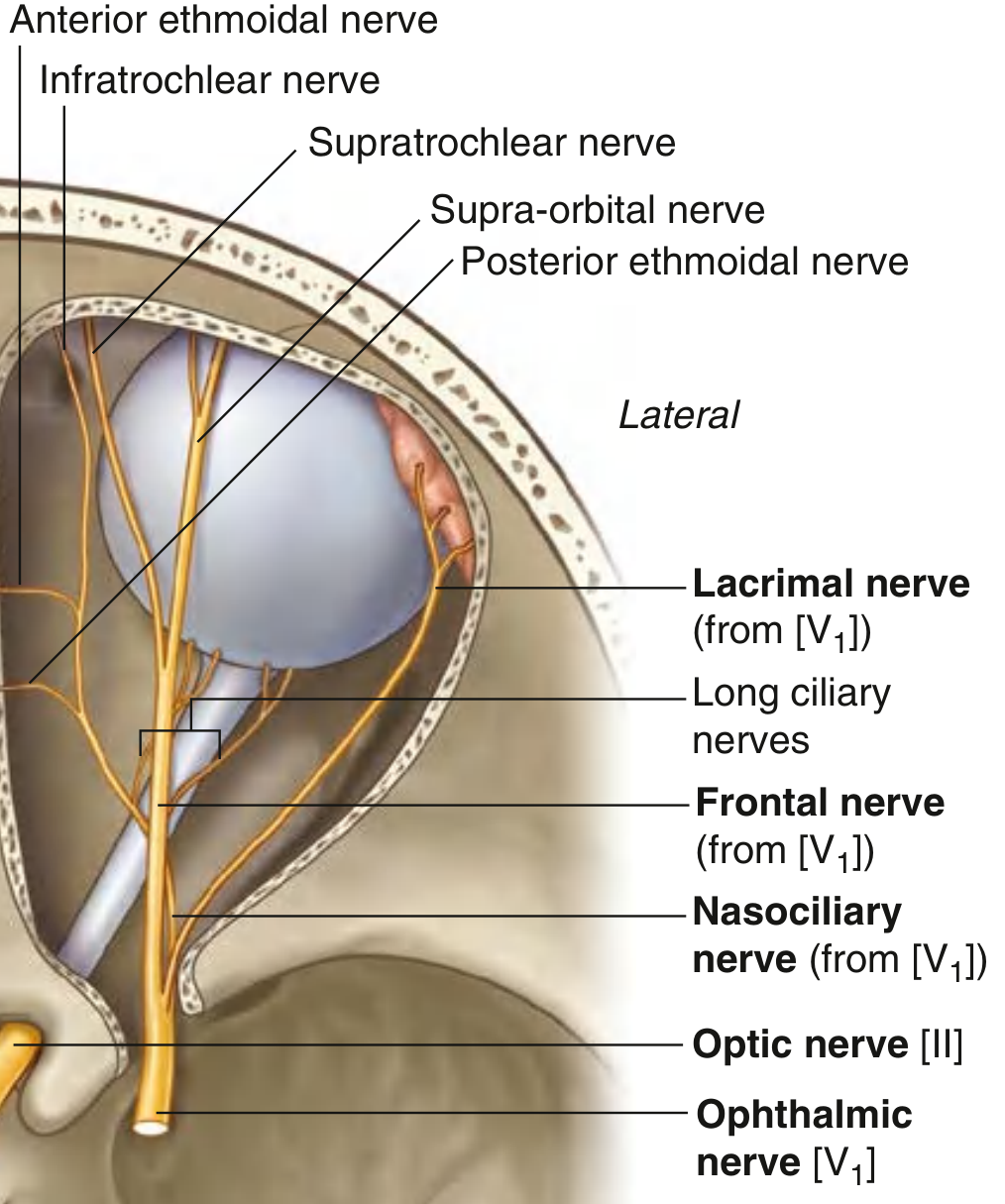
The three terminal branches of V1 - nasociliary, frontal, and lacrimal nerves - with their subdivisions in the orbit. (Gray's Anatomy for Students)
Clinical Relevance
| Situation | V1 Involvement |
|---|---|
| Cavernous sinus lesion | V1 (and V2) affected; often combined with III, IV, VI palsies |
| Superior orbital fissure lesion | V1 branches compressed along with III, IV, VI |
| Petrous apex / Gradenigo syndrome | V1 + VI + VII affected (following otitis media) |
| Herpes zoster ophthalmicus | Reactivation in V1 territory; rash on forehead, tip of nose (Hutchinson's sign via nasociliary nerve) indicates corneal involvement risk |
| Nasociliary nerve damage | Loss of corneal reflex; neuroparalytic keratitis |
| Perineural invasion (malignancy) | Insidious facial numbness in V1 territory; seen with head/neck adenoid cystic carcinoma, SCC, melanoma |
| Diabetes | Bilateral corneal hypoesthesia (45%); may progress to complete corneal anesthesia |
Key Relationships in the Cavernous Sinus
From superior to inferior in the lateral wall:
- CN III (oculomotor)
- CN IV (trochlear)
- CN V1 (ophthalmic) ← V1 is here
- CN V2 (maxillary)
- CN VI lies medially, in the sinus itself, lateral to the internal carotid artery
Sources: Gray's Anatomy for Students (9780323934237); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (9781138094634); Bradley and Daroff's Neurology in Clinical Practice (9780323642613); Localization in Clinical Neurology, 8e (9781975160241)
detailed notes on physiology of pain
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from four authoritative sources. Here are detailed, well-organized notes.
Physiology of Pain - Detailed Notes
1. Definition and Historical Background
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage. The scientific study of its mechanisms progressed through several theoretical frameworks:
- Specificity theory: Dedicated pain fibers and a specific pain center in the brain.
- Pattern theory: Pain results from stimulus intensity and the pattern of nerve impulses rather than specific fibers.
- Gate Control Theory (Melzack & Wall, 1965): A landmark refinement - large-diameter myelinated fibers (A-beta) excite inhibitory interneurons (I cells) in the dorsal horn, which then presynaptically inhibit the transmission ("T") cells. Conversely, small C fibers inhibit these I cells, leaving T cells in an excitatory state. They also postulated descending control from the brainstem, thalamus, and limbic lobes. This forms the basis for TENS therapy. While clinically influential, the gate control mechanism has known weaknesses and does not fully explain all pain phenomena.
2. Types of Stimuli That Activate Pain Receptors
Pain receptors respond to different stimuli depending on the tissue type:
| Tissue | Adequate Stimulus |
|---|---|
| Skin | Pricking, cutting, crushing, burning, freezing |
| Stomach/intestine | Engorged/inflamed mucosa, distension, spasm of smooth muscle, mesenteric traction |
| Skeletal muscle | Ischemia, necrosis, hemorrhage, prolonged contraction, injection of irritants |
| Cardiac muscle | Ischemia (primary mechanism) |
| Joints | Inflammation of synovial membrane, stretching/tearing of ligaments |
| Blood vessels | Piercing, inflammation, distension, traction |
| Nerve roots/ganglia | Compression (e.g., ruptured disc) |
| Periosteum | Mechanical injury |
3. Peripheral Nociceptors and Primary Afferent Fibers
Types of Primary Afferent Fibers
| Fiber Type | Diameter | Conduction Velocity | Ending | Sensation |
|---|---|---|---|---|
| A-alpha (Aα) | 15-20 μm | 70-120 m/s | Golgi/Ruffini/spindle | Proprioception |
| A-beta (Aβ) | 5-15 μm | 40-70 m/s | Encapsulated (Meissner, Pacinian, etc.) | Touch, pressure, vibration |
| A-delta (Aδ) | 1-5 μm | 10-35 m/s | Free nerve endings | "First pain" - sharp, well-localized; also innocuous cold |
| C fibers | <1 μm | 0.5-1 m/s | Free nerve endings | "Second pain" - burning, dull, poorly localized; also warmth |
- Aδ fibers mediate epicritic (fast) pain - the initial sharp, pricking, well-localized pain on tissue injury.
- C fibers mediate protopathic (slow) pain - the subsequent burning or aching, diffuse, poorly localized pain.
- Most Aδ and C nociceptors are polymodal: they respond to mechanical, thermal, and chemical stimuli.
- Cell bodies of all primary afferents are located in the dorsal root ganglion (DRG).
Sub-types of Cutaneous Nociceptors
- High-threshold mechanoreceptors (HTMs) - associated with Aδ fibers; respond only to intense mechanical stimuli.
- Mechanothermal nociceptors (MTs) - also Aδ fibers; respond to both heat and mechanical stimuli.
- Polymodal nociceptors - associated with C fibers; respond to mechanical, chemical, and thermal stimuli.
Molecular Transduction Channels on Nociceptors
- TRP (Transient Receptor Potential) channels are the primary transducers of noxious stimuli at the peripheral terminal.
- TRPV1 (capsaicin receptor/vanilloid receptor 1): responds to capsaicin, heat (>43°C), and acid; expressed exclusively on nociceptors - a convergence point for multiple modalities in a single neuron.
- Activation of TRP channels opens voltage-sensitive Na+ and Ca2+ channels (Nav, Cav), initiating an action potential.
- Nav1.7 (SCN9A gene): Particularly important. Nonsense mutations of SCN9A cause congenital insensitivity to pain (complete inability to sense pain). Gain-of-function mutations cause erythromelalgia (paroxysmal burning extremity pain).
4. Chemical Mediators of Pain (Peripheral)
With tissue damage, proteolytic enzymes are released, acting on local proteins to liberate pain-producing substances:
- Histamine
- Prostaglandins (enhance Nav1.8 channel opening via membrane receptors)
- Serotonin (5-HT)
- Kinins (bradykinin) - released from sensory nerve endings or via circulation
- Potassium ions
- Substance P - released from C fiber nerve endings; causes cutaneous vasodilation (erythema) and edema (via histamine release from mast cells); acts as a chemoattractant for leukocytes
- CGRP (calcitonin gene-related peptide)
- Adenosine, ATP, galanin, somatostatin, NGF (nerve growth factor)
Neurogenic inflammation: Antidromic action potentials from small DRG cells cause local release of substance P, producing the axon reflex of Lewis (erythema + edema + flare around an injury site). This reflex is abolished in peripheral neuropathy.
5. Peripheral Sensitization
Inflammation lowers the pain threshold by a process called sensitization:
- Inflammatory mediators (prostaglandins, cytokines, bradykinin) act on peripheral nociceptors, reducing their activation threshold.
- Nociceptors that were previously silent ("silent nociceptors") become active.
- This produces primary hyperalgesia - exaggerated pain response at the site of injury.
- TNF-α plays a key role: decreases potassium conductance after injury, increasing neuronal excitability. Long-term changes occur via second-messenger activation and altered protein production.
6. The Dorsal Horn - First Central Relay
Rexed Laminae and Afferent Terminations
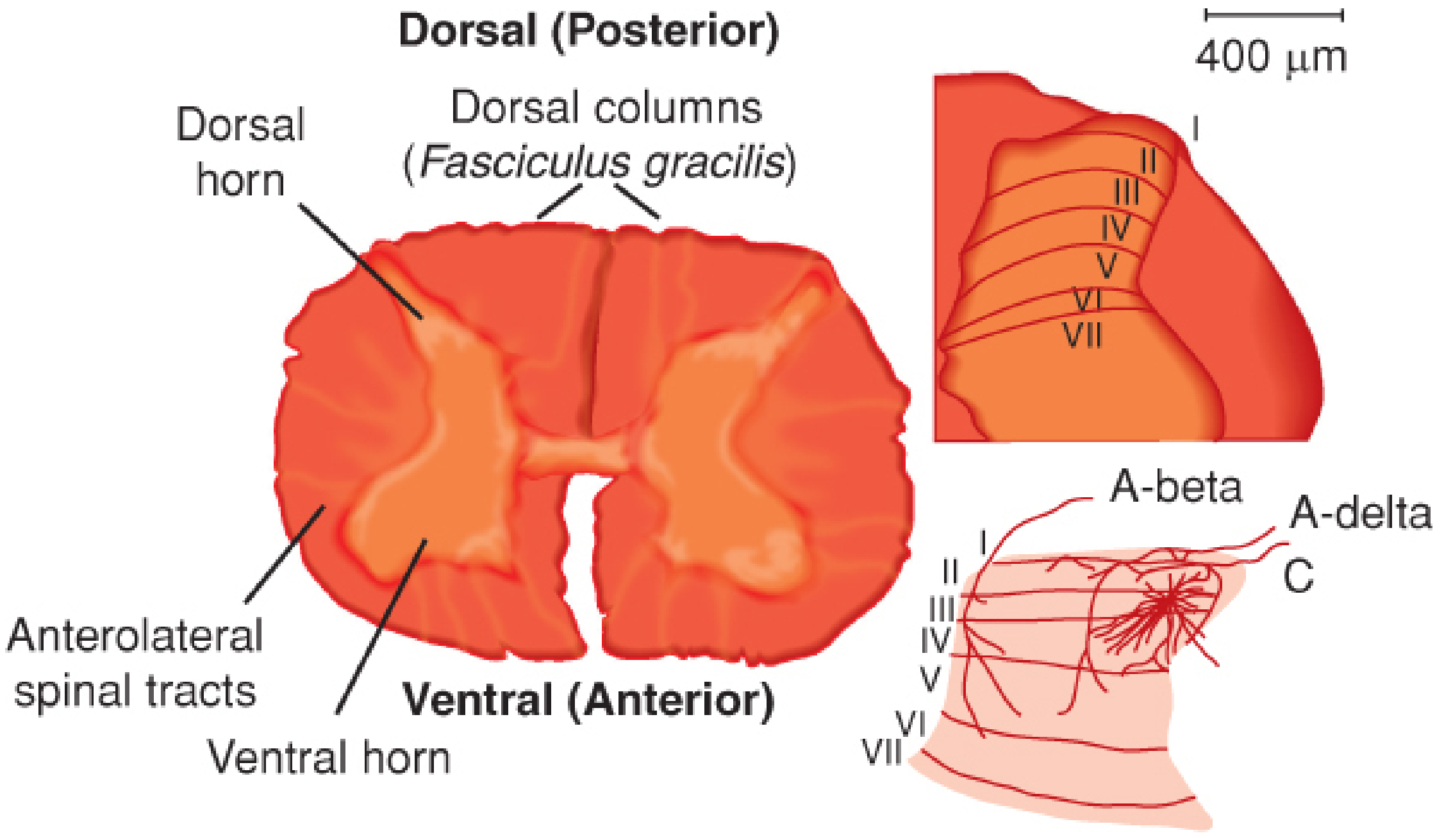
Rexed laminae of the dorsal horn and their primary afferent inputs. A-delta and C fibers terminate in laminae I-II; A-beta fibers in laminae III-V. (Barash et al., Clinical Anesthesia)
| Lamina | Name | Afferent Input | Neuron Type |
|---|---|---|---|
| I | Marginal nucleus | Aδ (HTM, MT) + C fibers | Projection neurons + interneurons |
| II | Substantia gelatinosa | C fibers (primarily) | Excitatory + inhibitory interneurons (few projection neurons) |
| III-IV | Nucleus proprius | Aβ (mainly) | Dorsal column pathway neurons |
| IV-VI | Deep dorsal horn | Aδ + some nociceptive | Wide dynamic range (WDR) neurons + projection neurons |
| V | - | Aδ (HTM) + visceral C | WDR neurons (important for convergence and referred pain) |
| X | Around central canal | Visceral C fibers | Visceral nociceptive relay |
Types of Dorsal Horn Neurons
- Nociceptive-specific (NS) neurons - respond only to noxious stimuli; in laminae I-II.
- Wide dynamic range (WDR) neurons - respond to both noxious and non-noxious stimuli; in lamina V. Important in wind-up phenomenon and referred pain.
Neurotransmitters at the Dorsal Horn Synapse
- Glutamate is the primary neurotransmitter.
- Acute, brief signals: AMPA receptor - produces fast, robust depolarization by increasing Na+ conductance.
- Prolonged/intense signals: NMDA receptor - activated after AMPA-mediated depolarization removes the Mg2+ block. Critical for central sensitization.
- Substance P - neuropeptide co-released with glutamate from C fibers; acts on NK1 receptors; contributes to sustained excitation and central sensitization.
- Other peptides: CGRP, ATP, adenosine, galanin, somatostatin, BDNF.
Visceral vs. Somatic Afferent Termination
- Somatic C fibers terminate 1-2 segments from entry (laminae I, II).
- Visceral C fibers terminate up to 5 segments rostrally or caudally, and bilaterally (laminae I, II, V, X, and contralateral V, X). This wider branching explains why visceral pain is poorly localized.
7. Ascending Pain Pathways
Spinothalamic Tract (STT) - Main Pathway
Second-order neurons from laminae I, IV, V cross in the anterior white commissure and ascend in the contralateral anterolateral quadrant as the spinothalamic tract.
The STT is somatotopically organized:
- Sacral fibers: posterolateral
- Cervical fibers: anteromedial
The STT divides into two functionally distinct components:
| Pathway | Termination | Function |
|---|---|---|
| Neospinothalamic tract | VPL nucleus of thalamus → primary somatosensory cortex (SI) | Fast, well-localized, discriminative pain ("where and how intense") |
| Paleospinothalamic tract | PAG, brainstem reticular formation → central/intralaminar thalamic nuclei | Slow, poorly localized pain; emotional/affective component ("how unpleasant") |
Cortical Processing of Pain ("Pain Matrix")
Multiple cortical areas are activated (shown by fMRI and PET):
- Primary somatosensory cortex (SI) - basic pain processing, intensity and localization
- Secondary somatosensory cortex (SII) - higher-order sensory processing
- Insular cortex - interoception, emotional dimension of pain
- Anterior cingulate cortex (ACC) - affective/motivational component ("suffering")
- Prefrontal cortex - attention, cognitive modulation
- Thalamus, hypothalamus, PAG - also activated in proportion to stimulus intensity
8. Referred Pain
Visceral and somatic nociceptors from different tissues converge on the same pool of second-order neurons in the dorsal horn. The brain misattributes the pain to the somatic structure:
- Cardiac pain (T1-T4 afferents) → referred to inner arm, ulnar border, precordium.
- Diaphragmatic irritation (C3-C5 phrenic nerve) → referred to shoulder tip.
- Renal colic → referred to groin and inner thigh.
The WDR neurons of lamina V are key mediators of referred pain. Once a pool of sensory neurons is activated, additional noxious stimuli can heighten activity across the whole sensory field - both ipsilateral and, to a lesser extent, contralateral.
Sclerotomes (Kellgren): Pain referral patterns from bones and ligaments that do not precisely overlap with dermatomes.
9. Endogenous Pain-Control Mechanisms
Descending Inhibitory System
Discovered by Reynolds (stimulation of PAG produces profound analgesia in rats). Key components:
- Periaqueductal gray (PAG) - receives input from hypothalamus, limbic cortex, and prefrontal cortex. Activates descending inhibitory pathways.
- Rostroventral medulla (RVM) - nucleus raphe magnus and adjacent reticular formation. Serotonergic and noradrenergic neurons descend in the dorsolateral funiculus.
- Dorsolateral pontine tegmentum (locus coeruleus) - noradrenergic descending fibers.
These descending fibers inhibit neurons in Rexed laminae I, II, and V of the dorsal horn via:
- Serotonin (5-HT)
- Noradrenaline
- Endogenous opioids (enkephalins, endorphins, dynorphins) acting on mu, delta, and kappa receptors
Strong emotion (fear, rage) activates the descending noradrenergic system, suppressing pain - the basis of "stress analgesia."
Endogenous Opioids
Naturally occurring brain opioid peptides share properties with exogenous opiates:
- Beta-endorphin (from POMC; hypothalamus/pituitary)
- Enkephalins (met-enkephalin, leu-enkephalin; widely distributed in CNS)
- Dynorphins (spinal cord, brainstem)
They act on mu (μ), delta (δ), and kappa (κ) opioid receptors at presynaptic and postsynaptic sites in the dorsal horn and brain.
10. Central Sensitization
A pathological state of increased central neuronal responsiveness responsible for much chronic pain:
Triggers: Sustained or intense peripheral nociceptive input → repetitive firing in C fibers → wind-up (temporal summation) in dorsal horn WDR neurons.
Mechanisms:
- NMDA receptor activation (after Mg2+ block removed by AMPA-mediated depolarization) → Ca2+ influx → intracellular kinase activation → phosphorylation of AMPA and NMDA receptors → increased sensitivity.
- Expansion of dorsal horn receptive fields.
- Loss of GABAergic inhibition in the dorsal horn.
Consequences:
- Hyperalgesia - exaggerated pain response to a normally noxious stimulus.
- Allodynia - pain in response to a normally innocuous stimulus (e.g., light touch). Mediated partly by Aβ fibers undergoing a phenotypic switch - after injury, Aβ fibers begin expressing substance P, converting them to nociceptive signaling ("C-fiber phenotype").
- Expansion of the pain area beyond the original injury site (secondary hyperalgesia).
- Referred pain and hyperalgesia across multiple spinal segments.
11. Chronic Pain Mechanisms
-
Ectopic discharges: Injured C and Aδ fibers develop spontaneous activity due to overexpression of Nav channels at injury sites. Adrenergic receptor overexpression makes them sensitive to circulating catecholamines (basis of causalgia/CRPS and its response to sympathetic blockade).
-
Central autonomous overactivity: Dorsal horn neurons chronically bombarded with pain impulses become autonomously hyperactive, maintained by excitatory amino acids (glutamate via NMDA). This persists even after peripheral injury resolves - basis of deafferentation pain and phantom limb pain.
-
Neuroinflammation: Non-neuronal cells (immune cells, glial cells, keratinocytes, cancer cells) release cytokines and other inflammatory mediators (TNF-α, prostaglandins) that sustain peripheral and central sensitization.
-
Dysregulated descending inhibition: Failure of the PAG-RVM inhibitory system contributes to chronic widespread pain (fibromyalgia, central sensitization syndromes).
12. Perception of Pain - Modulating Factors
| Factor | Effect on Pain |
|---|---|
| Inflammation | Lowers threshold (sensitization) |
| Local anesthetics, opioids | Raise threshold |
| Distraction/suggestion | Reduce awareness (not threshold) |
| Fear, rage | Suppress pain (activates descending noradrenergic system) |
| Depression | Enhances pain |
| Mania | Lessens pain |
| Frontal lobe lesions | Threshold unchanged; reaction abolished ("asymbolia for pain") |
| Placebos | Reduce pain in ~1/3 of patients (likely endogenous opioid release) |
Summary Flowchart
Tissue damage / noxious stimulus
↓
Peripheral nociceptors (free nerve endings)
- TRP channels, Nav, Cav
↓
Chemical mediators released (histamine, PGs, bradykinin, K+, SP)
→ Peripheral sensitization
↓
Action potential in Aδ (fast/sharp) and C fibers (slow/burning)
↓
DRG (cell body) → dorsal root → Lissauer's tract → Dorsal horn
- Aδ → Laminae I, V
- C fibers → Laminae I, II
↓
Glutamate (AMPA → fast; NMDA → sensitization) + Substance P
WDR neurons (lamina V) + NS neurons (laminae I-II)
↓
Cross anterior white commissure → Spinothalamic tract (contralateral)
- Neospinothalamic → VPL → SI (fast, localized)
- Paleospinothalamic → PAG/reticular → intralaminar thalamus (slow, emotional)
↓
Cortical pain matrix (SI, SII, insula, ACC, prefrontal)
↓
Conscious pain perception + emotional response
↑ Descending inhibition (PAG → RVM → dorsolateral funiculus)
via serotonin, noradrenaline, enkephalins (gate modulation)
Sources: Adams and Victor's Principles of Neurology, 12th Ed. (9781264264520); Bradley and Daroff's Neurology in Clinical Practice (9780323642613); Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed. (9781975199074); Localization in Clinical Neurology, 8th Ed. (9781975160241)
This is a shared conversation. Sign in to Orris to start your own chat.