Lipid vulgar
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I have all the information needed. I'll now note that "Lipid vulgar" is almost certainly a misspelling/autocorrect of "Lupus vulgaris" and provide a comprehensive answer.
Lupus Vulgaris (Tuberculosis Luposa)
"Lipid vulgar" is not a recognized medical term. This appears to be an autocorrect or misspelling of Lupus vulgaris - the most common form of cutaneous tuberculosis.
What is Lupus Vulgaris?
Lupus vulgaris (LV) is an extremely chronic, progressive form of cutaneous tuberculosis occurring in individuals with moderate immunity and high tuberculin sensitivity. It is a post-primary, paucibacillary (few organisms) form of TB that results from hematogenous, lymphatic, or contiguous spread from a focus elsewhere in the body. - Fitzpatrick's Dermatology, p. 2894

Epidemiology
- Females are affected 2-3 times more often than males
- All age groups affected equally
- Less common in the United States than in Europe
- Incidence has declined steadily worldwide
Clinical Features
- Location: ~90% involve the head and neck - commonly starts on the nose, cheek, earlobe, or scalp
- Initial lesion: brownish-red, soft or friable macule or papule (smooth or hyperkeratotic surface)
- Pathognomonic sign: "Apple jelly" color on diascopy (pressing a glass slide on the lesion reveals a yellowish-brown translucent color - the hallmark of LV)
- Progression: elevation, deeper brownish color, plaque formation; gyrate outline due to involution in one area with expansion in another
- Small soft papules called "lupomas" are embedded deeply and diffusely in the infiltrated dermis
- Ulceration may occur; mucosae can be primarily involved
- Postexanthematic lupus: after measles (or other febrile illness), multiple disseminated lesions may arise from hematogenous spread - Andrews' Diseases of the Skin, p. 383
Histopathology
- Prominent tubercle formation (epithelioid granulomas) - the most characteristic feature
- Secondary changes: epidermal thinning/atrophy, acanthosis, pseudoepitheliomatous hyperplasia
- Acid-fast bacilli are usually NOT found (paucibacillary nature)
- Old lesions composed mostly of epithelioid cells - may be impossible to distinguish from sarcoidosis
Diagnosis
| Tool | Finding |
|---|---|
| Diascopy | Apple jelly nodules (highly characteristic) |
| Tuberculin test | Strongly positive (except early postexanthematic form) |
| Bacterial culture | May be negative |
| PCR for M. tuberculosis | Supports diagnosis when culture is negative |
| Dermoscopy | Yellowish-orange patch indicating dermal granulomas |
Differential Diagnosis
| Category | Conditions |
|---|---|
| Most likely | Discoid lupus erythematosus, Sarcoidosis |
| Consider | Leprosy, Lupoid leishmaniasis, Lymphocytoma, Tertiary syphilis |
| Always rule out | Blastomycosis or other deep mycotic infections |
- Also: Colloid milia, acne vulgaris, rosacea, chronic discoid lupus erythematosus, Hansen disease
Complications
- Cartilage destruction of nose or ear - extensive disfigurement
- Atrophic scarring (characteristic - may recur within a scar)
- Fibrosis - can be pronounced and mutilating
- Dry rhinitis, destruction of nasal septum cartilage
- Scarring of soft palate, laryngeal stenosis
- Malignant transformation: long-standing LV can lead to squamous cell carcinoma (SCC outnumbers BCC; high risk of metastases)
- 40% of patients: associated TB lymphadenitis
- 10-20%: active pulmonary TB or TB of bones/joints
- Pulmonary TB is 4-10 times more frequent in LV patients vs. the general population
Treatment
Treatment follows standard antituberculous therapy (same regimens as systemic TB):
- Standard 4-drug regimen: Isoniazid + Rifampicin + Pyrazinamide + Ethambutol for 2 months, then Isoniazid + Rifampicin for 4 months (total 6 months)
- Without therapy, the disease progresses over many years to functional impairment and disfiguration
- Complete healing rarely occurs without therapy, though spontaneous involution of some lesions is possible
Sources: Fitzpatrick's Dermatology, 9e, pp. 2894-2895 | Andrews' Diseases of the Skin, pp. 382-383
Hair loss
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer on hair loss (alopecia).
Hair Loss (Alopecia)
Alopecia is the medical term for hair loss. The two major categories are scarring (permanent) and non-scarring (potentially reversible), depending on whether hair follicles are destroyed.
Classification Overview
| Type | Follicles | Reversible? | Examples |
|---|---|---|---|
| Non-scarring | Preserved | Yes | Androgenetic alopecia, alopecia areata, telogen effluvium, tinea capitis |
| Scarring (cicatricial) | Destroyed | No | Discoid lupus, lichen planopilaris, folliculitis decalvans, central centrifugal cicatricial alopecia |
In non-scarring alopecia, hair shafts are absent or miniaturized but follicles are preserved - explaining why regrowth is possible. In scarring alopecia, fibrosis and inflammation permanently destroy follicular openings. - Harrison's Principles of Internal Medicine 22E
1. Androgenetic Alopecia (Pattern Hair Loss)
The most common form in both men and women.
Male Pattern
- Begins in teens, 20s, or early 30s; starts with bitemporal recession ("professor angles") and vertex thinning
- Driven by dihydrotestosterone (DHT) - 5α-reductase converts testosterone to DHT, which miniaturizes follicles
- Each hair cycle produces finer, shorter hairs; terminal hairs are replaced by vellus hairs
- Progressive shortening of anagen phase; parietal and occipital areas typically spared
Female Pattern
- Diffuse thinning throughout the apical scalp; frontal hairline usually preserved
- Same follicular miniaturization and DHT mechanism as males, though less pronounced
- Always consider underlying androgen excess (PCOS, ovarian/adrenal tumor) if signs of virilization exist
Pathogenesis
- Polygenic inheritance with androgen sensitivity
- Higher 5α-reductase and androgen receptor levels in frontal vs. occipital follicles
- Androgen-inducible TGF-β1 from dermal papilla cells suppresses hair growth
- Eunuchs do not develop baldness - confirms androgen dependence
Treatment
| Drug | Mechanism | Key Facts |
|---|---|---|
| Minoxidil (topical 2%/5%) | Prolongs anagen, enlarges shaft diameter, promotes dermal papilla cell survival | Best for early cases (<10 yr), bald area <10 cm; must use indefinitely |
| Finasteride (1 mg/day, oral) | Type 2 5α-reductase inhibitor; blocks DHT production | Stops hair loss in ~90% of men; 65% show regrowth; takes ≥6 months; not for women of childbearing age |
| Dutasteride | Blocks both type 1 & type 2 5α-reductase | More complete DHT suppression than finasteride |
| Hair transplantation | Micrografts from occipital to frontal scalp | Excellent cosmetic results; occipital follicles are DHT-resistant |
- Andrews' Diseases of the Skin, pp. 871-872
2. Alopecia Areata (AA)
An autoimmune, non-scarring hair disorder affecting all ages and both sexes equally.
Variants
- Patchy AA - circumscribed patches (most common)
- Alopecia totalis - complete loss of scalp hair
- Alopecia universalis - complete loss of all body hair
Pathogenesis
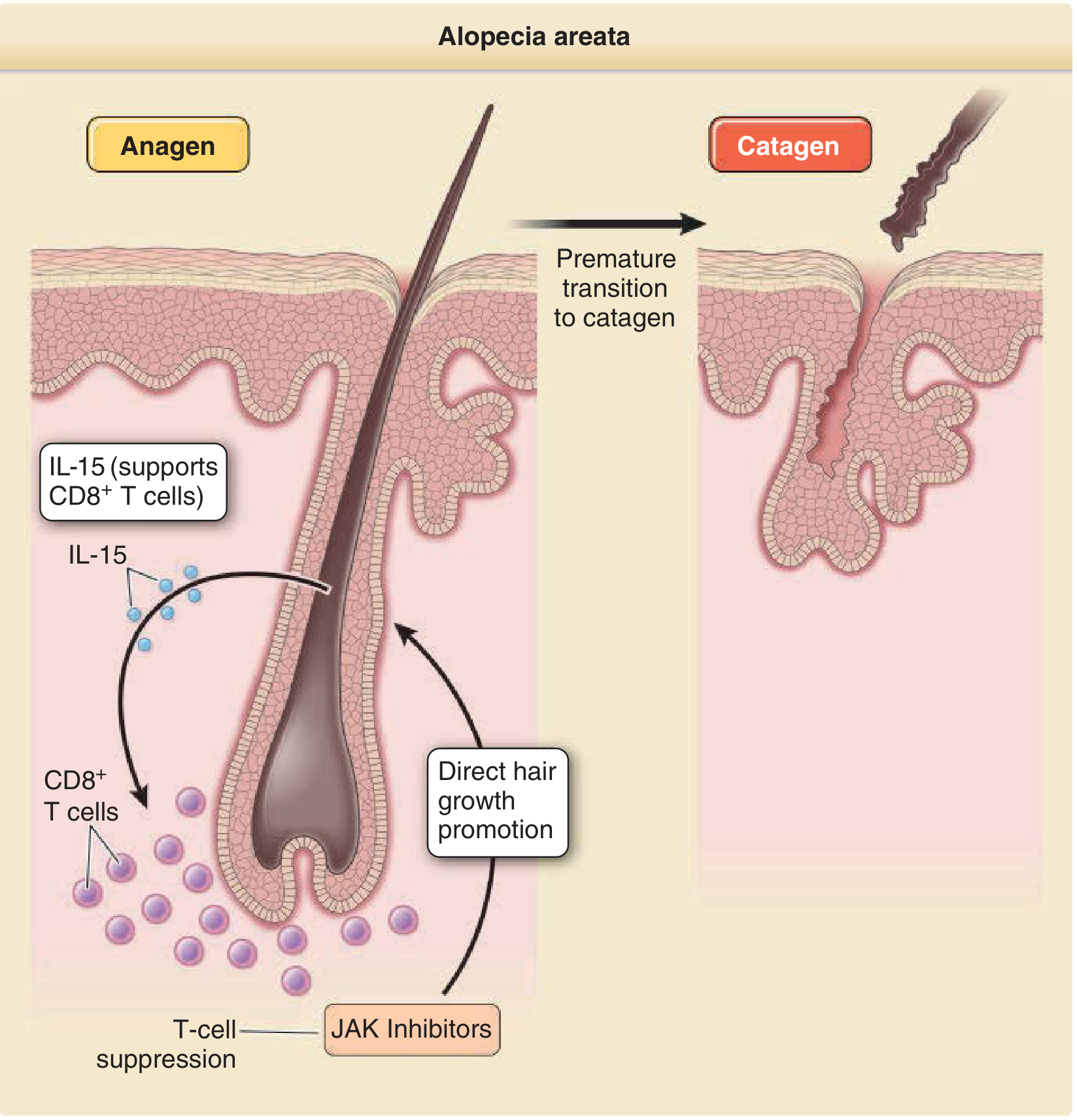
- Loss of immune privilege of the hair follicle - normally, follicles express low MHC Class I/II and produce local immunosuppressive cytokines
- CD8+ cytotoxic T cells (supported by IL-15 and IFN-γ) attack anagen hair bulbs, inducing premature catagen transition
- Since only the bulb is attacked (not the stem cell-containing bulge), regrowth is possible - classic non-scarring pattern
- Associated with other autoimmune diseases: thyroiditis, vitiligo, atopic dermatitis
- Fitzpatrick's Dermatology, p. 229
Clinical Features
- Well-demarcated, smooth, circular bald patches
- "Exclamation mark hairs" - broken, tapered hairs at patch margin
- Scalp biopsy: lymphocyte-predominant inflammation around anagen bulbs
Treatment
- Intralesional corticosteroids (triamcinolone acetonide) - first-line for limited disease
- Topical/systemic corticosteroids - for more extensive disease
- JAK inhibitors (baricitinib, ritlecitinib) - FDA-approved for severe AA; block JAK-STAT signaling, suppress inflammatory T cells, and directly promote hair follicle growth
- Topical minoxidil (adjunct)
- Spontaneous regrowth occurs in ~50% of patchy AA cases
3. Telogen Effluvium (TE)
The most common cause of diffuse hair loss. - Fitzpatrick's Dermatology
Mechanism
- Premature termination of the anagen (growth) phase of hair follicles → increased proportion in telogen (rest) phase → excessive shedding of club hairs (hairs with depigmented, club-shaped bulb, no sheath)
- Hair loss typically occurs 2-4 months after the triggering event
Common Triggers
- Fever / systemic illness
- Childbirth (postpartum effluvium) - most common type in women
- Major surgery or trauma
- Emotional stress
- Rapid weight loss / crash dieting
- Iron deficiency
- Hypothyroidism / hyperthyroidism
- Drugs (heparin, warfarin, propylthiouracil, isotretinoin, lithium, beta-blockers, interferons, colchicine, amphetamines)
- Chemotherapy (anagen effluvium - even more abrupt)
Types
| Subtype | Features |
|---|---|
| Acute TE | Classic; follows a known trigger; self-limiting |
| Chronic diffuse telogen hair loss | Multiple recurring triggers; no single identifiable cause |
| Chronic TE | Unknown etiology; mostly middle-aged women; whole-scalp involvement |
Diagnosis
- Pull test: grasp 40 hairs, slow pull - >4-6 club hairs is abnormal
- Shed hairs show depigmented club-shaped bulb (vs. anagen hairs which have pigmented bulb + sheath)
- Normal scalp has ~100,000 hairs; normal daily loss 100-150; in TE, 150-400+ shed daily
Treatment
- Identify and remove the trigger - spontaneous recovery is expected in most acute cases
- No specific therapy usually required; full recovery once the cause is corrected
- Andrews' Diseases of the Skin, p. 870
4. Scarring Alopecias
| Condition | Key Features |
|---|---|
| Discoid lupus erythematosus | Erythematous scaly plaques; hypopigmented center, hyperpigmented rim |
| Lichen planopilaris | Violaceous perifollicular macules at periphery of patches |
| Folliculitis decalvans | Follicular pustules at periphery; can cause reactive arthritis |
| Central centrifugal cicatricial alopecia | Most common scarring alopecia in Black women; starts at vertex |
| Linear scleroderma (morphea) | Band of sclerosis along scalp |
Active inflammation is at the periphery; fibrosis and follicular destruction is at the center. Biopsy + direct immunofluorescence is needed to differentiate these conditions.
5. Other Causes of Hair Loss
| Cause | Pattern | Notes |
|---|---|---|
| Tinea capitis | Patchy with scaling | Fungal; treated with systemic antifungals |
| Secondary syphilis | "Moth-eaten" scattered patches | Serologic testing |
| Traction alopecia | Marginal/frontal | From tight hairstyles; early cases are reversible |
| Alopecia mucinosa | Follicular papules with mucin | May be associated with lymphoma |
| Hypothyroidism/hyperthyroidism | Diffuse thinning | Reversible with treatment |
| SLE (non-scarring form) | Frontal "lupus hairs" | Coincides with disease flares |
| Pressure alopecia | Localized | From prolonged pressure (surgery, ICU) |
Diagnostic Approach Summary
- Scarring vs. non-scarring - look for follicular openings on scalp
- Pattern - diffuse vs. patchy vs. patterned
- Pull test - assess telogen shed
- History - triggering events 2-4 months prior, medications, systemic symptoms
- Labs - TSH, ferritin, CBC, androgens (in women with virilization)
- Scalp biopsy - gold standard for scarring alopecias and diagnostic uncertainty
- Dermoscopy/trichoscopy - non-invasive assessment of follicular miniaturization, exclamation mark hairs, etc.
Sources: Harrison's Principles of Internal Medicine 22E, p. 2070-2082 | Fitzpatrick's Dermatology 9e, pp. 229-234 | Andrews' Diseases of the Skin, pp. 869-873
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I have all I need for a detailed, well-sourced answer on the radiological changes in psoriasis shown in the image.
Radiological Changes in Psoriasis (Psoriatic Arthritis)
The image is from a Dermatology workbook and lists the classic radiological findings in psoriatic arthritis (PsA) using the mnemonic POISON:
P - Pencil in Cup Deformity O - Osteolysis I - Ivory Phalanx S - Sausage Digits O - Opera Glass Deformity N - Narrowing of Joint Spaces
Here is the actual X-ray demonstrating pencil-in-cup deformity at the DIP joint of the middle finger:

Detailed Breakdown of Each Finding
1. Pencil-in-Cup Deformity
- The most pathognomonic radiological finding of psoriatic arthritis
- Erosions on the distal side of the DIP joint cause the head of the bone to become tapered and pointed ("pencil"), while the base of the next phalanx becomes eroded and widened into a cup shape
- The tapering/whittling of the phalanges with cupping of the proximal end is what creates the classic pencil-in-cup appearance
- Seen at DIP and PIP joints of both hands and feet
- "Erosions on the distal side of the joint classically merge together to produce a 'pencil-in-cup' appearance considered by some to be pathognomonic of the disease" - Grainger & Allison's Diagnostic Radiology
2. Osteolysis
- Acro-osteolysis: resorption/destruction of the distal phalangeal tufts - a hallmark feature
- Helps distinguish PsA from erosive osteoarthritis
- Progressive osteolysis of terminal phalanges gives them a peg-like appearance
- May progress to involve most or all of a phalanx
- Osteolysis of metatarsals also occurs
3. Ivory Phalanx
- Increased density (sclerosis) of a phalanx, giving it a uniformly dense, white "ivory" appearance on X-ray
- Due to periosteal new bone formation and sclerosis
- A unique feature of psoriatic arthritis not seen in RA
- Most commonly seen in the terminal phalanx
4. Sausage Digits (Dactylitis)
- Global uniform swelling of an entire digit from tip to base
- Caused by enthesitis at multiple sites within the digit plus tenosynovitis of the flexor tendon sheath
- Clinically: the whole finger/toe looks like a sausage
- Radiologically: diffuse soft-tissue swelling of the whole digit
- "Global swelling of a digit in the form of dactylitis or the so called 'sausage digit' is typical" - Grainger & Allison
5. Opera Glass Deformity (Arthritis Mutilans)
- Seen in the most severe destructive form of PsA - arthritis mutilans (~5% of patients)
- Severe osteolysis of phalanges and metacarpals causes shortening and telescoping of digits
- The skin wrinkles and folds as the bone collapses inward - resembles a collapsible opera glass/telescope
- Clinically, the digit can be pulled out to normal length ("telescoping" or "main en lorgnette")
- "Typically involving multiple digits, this rare arthropathy has been termed arthritis mutilans or the opera glass hand" - Firestein & Kelley's Rheumatology
6. Narrowing of Joint Spaces
- Due to cartilage destruction from synovial inflammation
- Involves DIP and PIP joints preferentially; relative sparing of MCP and MTP joints (helps distinguish from RA)
- May progress to bony ankylosis (complete fusion) - another feature distinguishing PsA from RA
- Note: periarticular osteopenia is characteristically absent in PsA (unlike RA where it is prominent) - this is a key distinguishing feature
Other Notable Radiological Features of PsA
| Feature | Details |
|---|---|
| No periarticular osteopenia | Distinguishes PsA from RA |
| Enthesitis pattern erosions | New bone formation at and adjacent to erosion sites |
| Asymmetric sacroiliitis | Unlike the symmetric sacroiliitis of AS |
| Paravertebral ossification | Large, bulky syndesmophytes |
| "Bamboo spine" is rare | When spine is involved; differs from classic AS |
| Bony ankylosis | Complete joint fusion - can occur |
Clinical Patterns of PsA (5 Types)
| Pattern | Frequency | Key Features |
|---|---|---|
| Oligoarthritis (asymmetric) | 70% | Most common; swelling + tenosynovitis |
| Asymmetric DIP arthritis | 16% | With nail damage |
| RA-like symmetric polyarthritis | 15% | Claw hand |
| Arthritis mutilans | 5% | Opera glass hand, severe osteolysis |
| Ankylosing spondylitis pattern | 5% | Spinal + large joint disease |
- HLA-B27 positive in ~50% of patients
- Skin involvement precedes joint disease by several years
Sources: Grainger & Allison's Diagnostic Radiology, pp. 1122-1123 | Andrews' Diseases of the Skin, p. 1333-1345 | Firestein & Kelley's Textbook of Rheumatology | Miller's Review of Orthopaedics 9e
Radiology image
It looks like you'd like to discuss a radiology image, but no image was attached to your message.
Could you please:
- Upload the radiology image (X-ray, CT, MRI, ultrasound, etc.), or
- Describe what you're seeing in the image, or
- Tell me the topic you'd like me to find radiology images for from the medical textbooks?
For above find in psoriasis
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here are all the radiology images from the textbooks showing the classic findings of psoriatic arthritis, mapped to the POISON mnemonic:
Radiology Images - Psoriatic Arthritis (POISON)
🔴 Image 1 - Pencil-in-Cup Deformity + Osteolysis (DIP Joints, Fingers)
What to see: The middle finger (white arrow) shows the classic pencil-in-cup erosive deformity at the DIP joint - the proximal bone is tapered (pencil) fitting into a widened erosive cup of the distal bone. Multiple digits show varying degrees of bone loss and peg-like phalangeal appearance (osteolysis). Note the absence of periarticular osteopenia.
🔴 Image 2 - DIP Erosion + Enthesophyte Formation
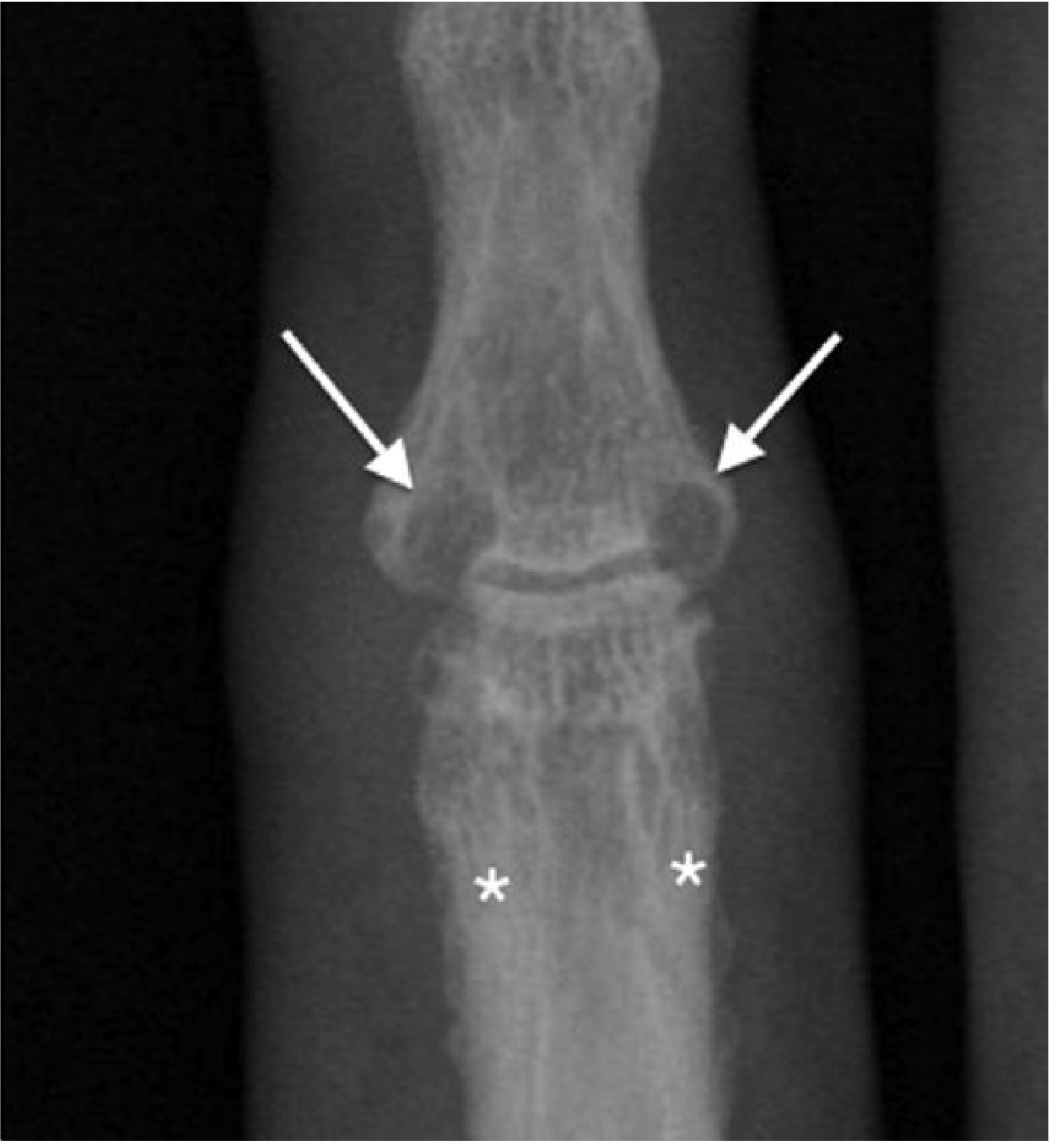
What to see: Close-up of a single digit DIP joint.
- Arrows = erosion of the distal phalanx at the joint margins
- Asterisks = prominent fluffy enthesophyte (new bone) formation both proximal and distal to the DIP joint
- This "bone erosion + new bone formation" combination is characteristic of PsA (unlike RA which shows pure erosion)
🔴 Image 3 - Arthritis Mutilans / Opera Glass Deformity (Foot, MTP Joints)

What to see: X-ray of the forefoot (metatarsals labeled MT).
- Subluxation and complete erosion/loss of the phalanges at the MTP joints
- The 4th toe shows nearly complete dissolution of the middle and distal phalanges - severe osteolysis
- This extreme bone destruction leads to the opera glass / arthritis mutilans appearance clinically
🔴 Image 4 - Psoriatic Spondylitis + Asymmetric Sacroiliitis (Spine)
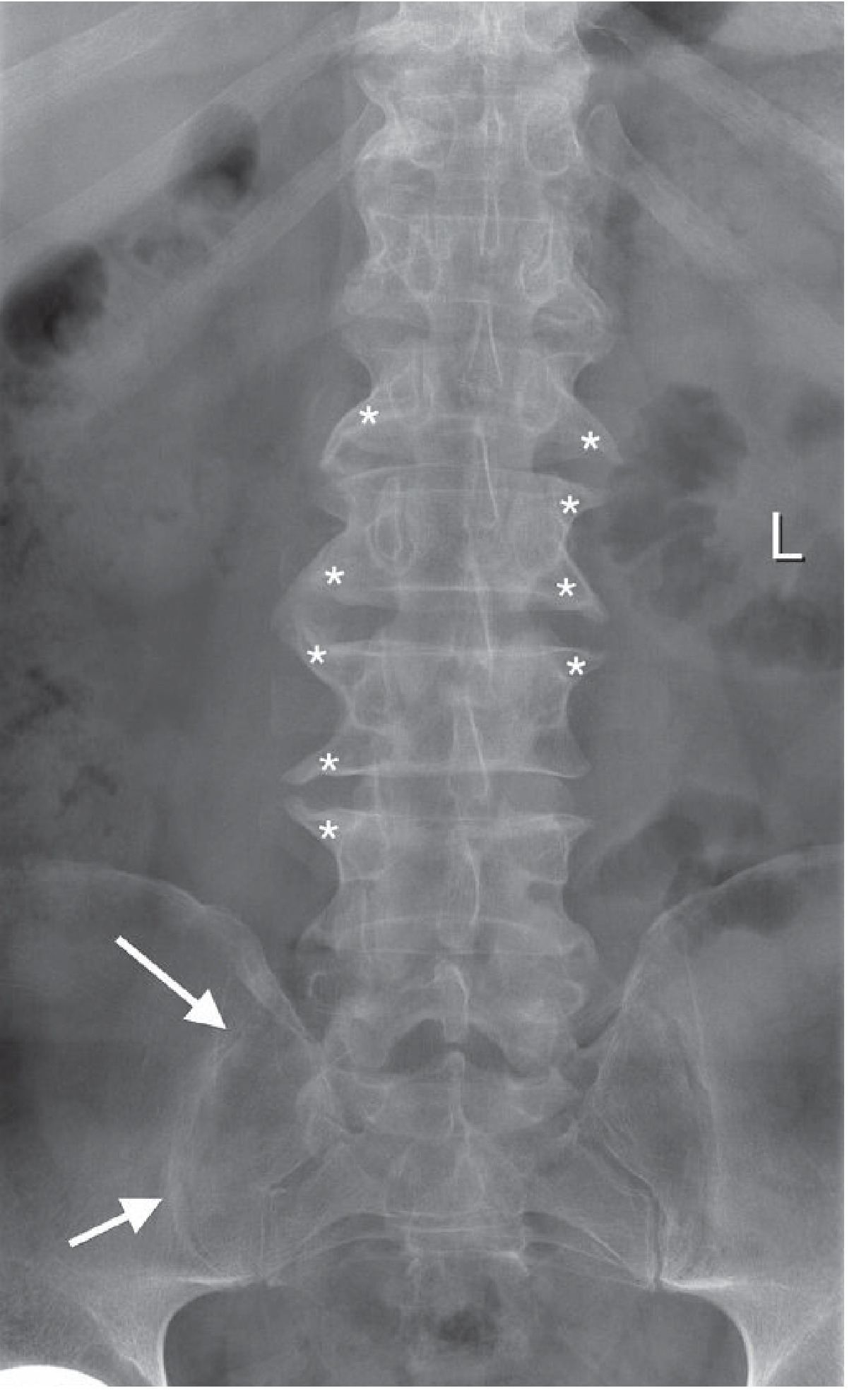
What to see:
- Arrows = Asymmetric sacroiliitis (unilateral/asymmetric joint space loss on the left - distinguishes PsA from AS which is symmetric)
- Asterisks = Spinal enthesophytes that are coarse and more horizontally oriented (compared to the fine, vertically oriented syndesmophytes of ankylosing spondylitis)
- No "bamboo spine" (complete fusion) - that is more characteristic of AS
Summary: What Each Image Shows
| Image | Finding | POISON Letter |
|---|---|---|
| Image 1 | Pencil-in-cup at DIP + peg-like phalanges | P + O |
| Image 2 | DIP erosion + fluffy enthesophytes | P + N |
| Image 3 | Arthritis mutilans (foot MTP) | O + O (osteolysis + opera glass) |
| Image 4 | Asymmetric sacroiliitis + horizontal enthesophytes | N (narrowing) |
Source: Grainger & Allison's Diagnostic Radiology, pp. 1122-1123
This is a shared conversation. Sign in to Orris to start your own chat.