Cardiac conditions requiring open heart surgery: briefly describe the pathophysiology, clinical presentations and management of the following conditions:
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Searching PubMed
"atrial septal defect" AND management
Loading Image
I now have everything needed for a thorough answer. Here is the complete response:
Atrial Septal Defect (ASD)
ASD is one of the most common congenital cardiac lesions, occurring in approximately 13 per 10,000 live births, and is the most common congenital defect diagnosed in adults because - unlike VSDs - ASDs rarely close spontaneously. - Sabiston Textbook of Surgery, p. 2564
Types of ASD
There are three anatomic subtypes, classified by location:
| Type | Frequency | Location | Associated Anomalies |
|---|---|---|---|
| Secundum | ~90% | Fossa ovalis / central septum | Usually isolated |
| Primum | ~5% | Adjacent to AV valves | AV valve abnormalities, VSD |
| Sinus venosus | ~5% | Near SVC or IVC orifice | Anomalous pulmonary venous return |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 504
Pathophysiology
Normal fetal development: In fetal life, the lungs are non-functional and pulmonary pressures exceed systemic pressures, keeping the foramen ovale open (right-to-left). At birth, lung expansion drops pulmonary vascular resistance (PVR), left atrial pressure rises above right atrial pressure, and the foramen ovale closes.
ASD mechanism: When closure is incomplete (especially of the septum primum in secundum ASDs), a persistent communication between the atria remains. Because systemic vascular resistance (SVR) greatly exceeds PVR, and because the right ventricle is far more compliant than the left, blood flows left-to-right across the defect. - Robbins, p. 504

Fig. 12.3 - Common congenital causes of left-to-right shunts. Arrow in (A) shows the direction of ASD flow from LA to RA. (Robbins, Cotran & Kumar)
Consequences of chronic left-to-right shunting:
-
Pulmonary blood flow may be 2-8x normal (Qp/Qs can exceed 3:1 in large defects)
-
Right heart volume overload - right atrial and right ventricular dilation and hypertrophy
-
Increased flow through the pulmonary valve causes a flow murmur
-
Over decades, sustained right-sided pressure and volume overload can lead to pulmonary arterial hypertension - less common in ASDs than VSDs, but possible
-
Paradoxical right-to-left shunting can occur transiently during increased intrathoracic pressure (Valsalva, coughing), risking paradoxical embolism and stroke
-
In advanced disease: Eisenmenger syndrome (reversal of shunt to right-to-left, cyanosis) - though this is far less common than with VSDs
-
Sabiston Textbook of Surgery, p. 2564; Robbins, p. 504-505
Clinical Presentation
In children: Most are asymptomatic or have only mild exercise intolerance and frequent respiratory tract infections. - Sabiston, p. 2564
In adults (symptoms typically emerge in the 3rd-5th decade):
-
Dyspnea on exertion - the most common presenting symptom
-
Fatigue and exercise intolerance
-
Palpitations, atrial fibrillation/flutter - due to atrial dilation and volume overload
-
Syncope or stroke - from atrial arrhythmias or paradoxical embolism
-
Signs of right heart failure: peripheral edema, elevated JVP, hepatomegaly in late disease
-
More than 70% of patients are functionally impaired by the 5th decade if untreated
-
Goldman-Cecil Medicine, p. 980
Physical Examination
| Finding | Mechanism |
|---|---|
| Wide, fixed splitting of S2 | Hallmark sign - increased venous return raises right atrial pressure during inspiration, offsetting normal respiratory variation; delayed pulmonary valve closure from RV overload |
| Soft midsystolic murmur (2nd left interspace) | Increased flow across the pulmonary valve |
| Mid-diastolic murmur (lower left sternal border) | Increased flow across the tricuspid valve (with large shunts) |
| Right ventricular heave | RV volume overload, felt at left parasternal area |
- Goldman-Cecil Medicine, p. 984
Investigations
-
ECG: Incomplete right bundle branch block (rSR' pattern in V1) is characteristic; right axis deviation; prolonged PR interval, atrial fibrillation/flutter with advanced disease
-
Chest X-ray: Pulmonary vascular plethora (bilateral increased lung markings), dilated main pulmonary artery and branches, right atrial and right ventricular enlargement
-
Echocardiography (TTE/TEE): Definitive diagnostic tool - identifies the ASD location and size, quantifies the shunt ratio (Qp/Qs), estimates pulmonary artery pressures, and assesses RV function. Note: sinus venosus ASDs can be missed on TTE and require TEE or MRI
-
Cardiac catheterization: Not routinely needed, but used when pulmonary hypertension needs quantification
-
Goldman-Cecil Medicine, p. 985-986
Management
Indications for Closure
Closure is recommended when there is:
- Qp/Qs ratio ≥ 1.5:1 with evidence of right heart volume overload
- Paradoxical embolism
- Symptomatic patients at any age
Most centers recommend closure before school age (4-5 years) to prevent long-term right heart remodeling. Closure is generally contraindicated once irreversible pulmonary hypertension (Eisenmenger syndrome) has developed.
1. Catheter-Based (Device) Closure
Now the preferred approach for secundum ASDs, accounting for over 60% of ASD interventions worldwide. The Amplatzer Septal Occluder (and similar nitinol mesh devices) is deployed via transfemoral catheter under echocardiographic and fluoroscopic guidance. Requirements:
- Adequate septal rim (≥5 mm on most borders)
- Suitable defect anatomy (secundum type)
- Defect diameter typically ≤38 mm
A 2025 meta-analysis (de Liyis et al., PMID 38597284) comparing surgical vs. transcatheter closure in pediatric secundum ASD confirmed that both are highly effective, with transcatheter closure offering shorter hospital stays and fewer procedural complications.
2. Surgical Closure (Open Heart Surgery)
Indications for surgery over catheter closure:
- Primum and sinus venosus ASDs (not amenable to device closure)
- Inadequate septal rim for device anchorage
- Associated anomalies requiring surgical correction (anomalous pulmonary veins, AV valve repair)
- Failed device closure
Procedure: Performed under cardiopulmonary bypass via median sternotomy or minimally invasive right thoracotomy. A right atriotomy is made, and the defect is closed by:
- Direct suture closure - for small defects
- Patch closure - autologous pericardium or prosthetic material (Dacron/Gore-Tex) for larger defects
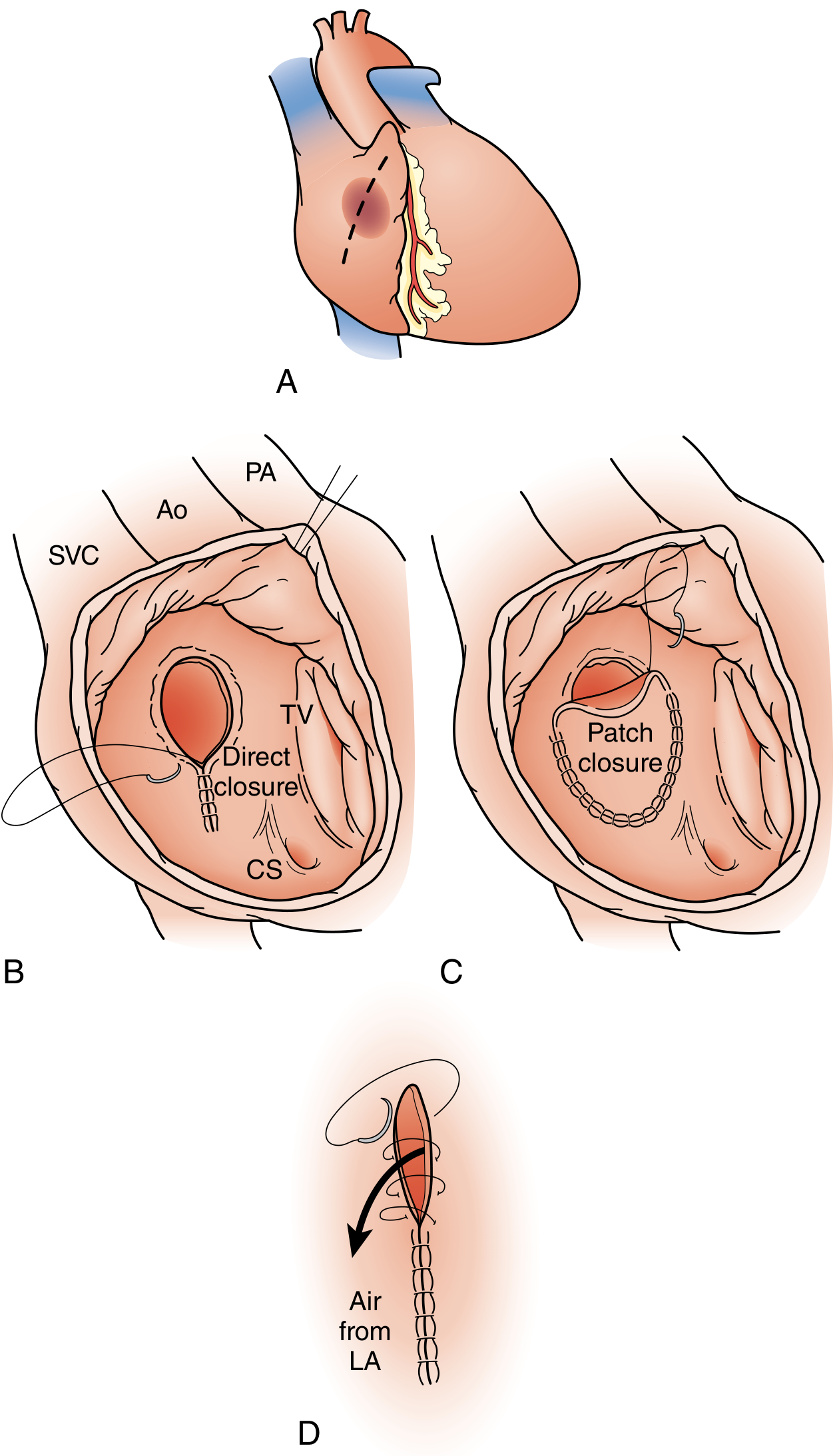
FIGURE 113.10 - Surgical closure for ASD: (A) Right atriotomy, (B) Direct suture closure, (C) Patch closure, (D) De-airing the LA. (Sabiston Textbook of Surgery)
For sinus venosus ASDs with partial anomalous pulmonary venous return, more complex repairs are required:
-
Superior type: intracardiac patch baffle, or the Warden procedure (SVC translocation) when anomalous veins drain high
-
Inferior type (scimitar syndrome): patch baffle in the IVC, potentially requiring hypothermic circulatory arrest
-
Sabiston Textbook of Surgery, p. 2564-2397
Outcomes: Surgical closure carries a very low perioperative mortality, with virtually no risk of residual defects. Post-operative survival is comparable to the general population when repair is done before the development of significant pulmonary hypertension. A 2025 systematic review (El-Andari et al., PMID 40517112) confirmed that minimally invasive approaches to surgical ASD repair have equivalent outcomes to conventional sternotomy with improved cosmesis and recovery.
3. Medical Management
- There is no medical therapy that closes the defect
- Antiplatelet therapy (aspirin) may be prescribed post-device closure for 3-6 months
- Rate/rhythm control and anticoagulation for atrial arrhythmias
- Diuretics and heart failure therapy if right heart failure is present
Summary Table
| Feature | Detail |
|---|---|
| Incidence | 13/10,000 live births |
| Most common type | Secundum (90%) |
| Shunt direction | Left-to-right (initially) |
| Hallmark sign | Wide, fixed splitting of S2 |
| ECG finding | Incomplete RBBB (rSR' in V1) |
| Echo finding | RV dilation, interatrial shunt on Doppler |
| Primary treatment | Device closure (most secundum ASDs) or surgery |
| Surgery needed for | Primum, sinus venosus, complex anatomy |
| Bypass technique | Cardiopulmonary bypass via right atriotomy |
| Prognosis (repaired) | Normal life expectancy if closed before PH develops |
Exam answer detailed
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, exam-level content from multiple authoritative sources (Braunwald's, Harrison's, Sabiston, Robbins, Goldman-Cecil). Here is the full, structured MBBS finals exam answer:
ATRIAL SEPTAL DEFECT (ASD)
Detailed MBBS Finals Exam Answer
DEFINITION
An Atrial Septal Defect (ASD) is an abnormal, fixed communication between the left and right atria through the interatrial septum. It is one of the most common congenital cardiac defects, occurring in 13 per 10,000 live births, and is the most frequent congenital heart lesion diagnosed in adults (since most ASDs - unlike VSDs - do not close spontaneously). - Robbins & Kumar, Pathologic Basis of Disease, p. 503
EMBRYOLOGY & CLASSIFICATION
Understanding ASD classification requires knowing normal atrial septum development:
Normal septal development:
- The septum primum grows down as a crescent-shaped membrane to partition the atria; the anterior gap beneath it is the ostium primum (allows fetal right-to-left flow)
- Before the ostium primum closes, perforations develop posteriorly forming the ostium secundum
- A second ingrowth - the septum secundum - grows from the right side to cover the ostium secundum, leaving a residual channel: the foramen ovale
- In fetal life, pulmonary pressure > systemic pressure, so the foramen ovale stays open (right-to-left)
- At birth, lung expansion drops pulmonary vascular resistance (PVR), left atrial pressure exceeds right atrial pressure, and the foramen ovale closes
ASD develops when this closure is incomplete or the septum is deficient. - Robbins, p. 503-504
Types of ASD (Classified by Location)
| Type | Frequency | Location | Key Associations |
|---|---|---|---|
| Secundum ASD | 90% | Fossa ovalis / central septum | Deficient septum primum; usually isolated; can be single, multiple, or fenestrated |
| Primum ASD | 5% | Adjacent to AV valves (AV canal region) | Always with AV valve abnormalities (mitral cleft); often + VSD; associated with Down syndrome |
| Sinus venosus ASD | 5% | Near SVC or IVC junction | Associated with partial anomalous pulmonary venous return (PAPVR); NOT amenable to device closure |
| Coronary sinus defect | Rare | Between coronary sinus and LA | Rare; requires surgery |
- Harrison's Principles of Internal Medicine 22E, p. 2114; Robbins, p. 504
Exam tip: Primum ASD + mitral cleft + VSD = Atrioventricular Septal Defect (AVSD) / Endocardial cushion defect - seen in Down syndrome (trisomy 21).
Do NOT confuse ASD with Patent Foramen Ovale (PFO): PFO is persistence of the flap valve of the fossa ovalis without true septal deficiency. It causes no right heart dilation and is present in ~25% of adults. It is detected by bubble contrast echo (agitated saline) with Valsalva. - Harrison's, p. 2114
PATHOPHYSIOLOGY
Direction of Shunt
In a normal heart after birth, systemic vascular resistance (SVR) greatly exceeds pulmonary vascular resistance (PVR), and the right ventricle is far more compliant (distensible) than the left ventricle. Through the ASD, blood flows left-to-right, from the high-pressure/low-compliance left atrium to the lower-pressure/high-compliance right side. - Robbins, p. 505
Hemodynamic Consequences
Left atrium → (through ASD) → Right atrium
↓
Increased RV volume load
↓
Increased pulmonary blood flow (Qp/Qs may be 2-8x normal, up to >3:1)
↓
Right heart dilation (RA + RV enlargement)
↓
Dilated pulmonary artery trunk and branches
- Robbins, p. 505; Sabiston Textbook of Surgery, p. 2564
Progression over Time
| Stage | Mechanism | Clinical Consequence |
|---|---|---|
| Early (childhood) | Compensated RV volume overload | Often asymptomatic |
| Middle (3rd-4th decade) | Progressive RA/RV dilation | Exercise intolerance, palpitations, SVT, AF |
| Late (4th-5th decade) | RV failure, PA dilation | Dyspnea at rest, right heart failure |
| End-stage | Sustained pulmonary hypertension | Eisenmenger syndrome (shunt reversal to R→L, cyanosis) |
Eisenmenger Syndrome: Chronic high pulmonary blood flow causes intimal hyperplasia and medial hypertrophy of pulmonary arterioles. PVR rises progressively until it exceeds SVR, reversing the shunt to right-to-left. The patient becomes cyanotic. At this stage, ASD closure is contraindicated (would acutely overload the left heart). - Braunwald's Heart Disease, p. 879
Exam tip: Eisenmenger is less common in ASDs than in VSDs or PDAs because the lower-pressure atrial shunt causes less vascular trauma to pulmonary arterioles.
Paradoxical Embolism
Even before Eisenmenger, patients are at risk of transient right-to-left shunting during moments of raised intrathoracic pressure (Valsalva, coughing, sneezing). A venous thrombus (even a small DVT) can cross the defect and enter the arterial circulation, causing cryptogenic stroke or systemic embolism. - Braunwald's Heart Disease, p. 969
CLINICAL FEATURES
In Children
Most children are asymptomatic or have mild:
- Recurrent respiratory tract infections (due to increased pulmonary blood flow)
- Mild exercise intolerance
In Adults (symptoms typically emerge after the 3rd decade)
>70% of patients are functionally impaired by the 5th decade if untreated. - Goldman-Cecil Medicine, p. 980
Symptoms:
- Dyspnea on exertion (most common presenting symptom)
- Fatigue and reduced exercise tolerance
- Palpitations - from supraventricular arrhythmias (SVT, atrial flutter, AF)
- Syncope - from arrhythmias or reduced cardiac output
- Stroke - from paradoxical embolism or AF
- Signs of right heart failure in advanced disease: peripheral edema, elevated JVP, hepatomegaly
Physical Examination Findings
| Sign | Mechanism | Significance |
|---|---|---|
| Wide, FIXED splitting of S2 | Hallmark sign. RV ejection is prolonged by volume overload. Inspiration normally increases right-sided return and delays P2, but in ASD the increased venous return also decreases left-to-right shunting, offsetting the change - so splitting is constant regardless of respiration | Pathognomonic for ASD |
| Soft midsystolic ejection murmur (2nd left interspace) | Increased flow through pulmonary valve (flow murmur, NOT the ASD itself) | Heard in majority |
| Mid-diastolic murmur (lower left sternal border) | Increased tricuspid flow with large shunts | Indicates significant shunt |
| RV heave / parasternal lift | Right ventricular hypertrophy and dilation | Left parasternal area |
| Pulmonary artery pulsation | Dilated pulmonary trunk | 2nd left intercostal space |
| Cyanosis + clubbing | Late - Eisenmenger syndrome (shunt reversal) | Poor prognostic sign |
- Goldman-Cecil Medicine, p. 984; Braunwald's, p. 878
INVESTIGATIONS
1. ECG
- Incomplete right bundle branch block (rSR' pattern in V1) - most characteristic finding
- Right axis deviation
- Right atrial enlargement (tall peaked P waves)
- Prolonged PR interval (1st degree heart block)
- Atrial fibrillation / flutter in older patients
- In primum ASD: left axis deviation (due to involvement of the AV node region)
Exam tip: Left axis deviation on ECG + ASD = Primum ASD (down syndrome link). Incomplete RBBB = Secundum ASD.
2. Chest X-Ray
- Pulmonary plethora - increased bilateral vascular markings (increased pulmonary blood flow)
- Dilated main pulmonary artery and its branches
- Right atrial and right ventricular enlargement
- Normal or small aortic knuckle (relatively reduced systemic flow)
- In Eisenmenger: oligaemic lung fields peripherally + dilated central pulmonary arteries ("pruning")
3. Echocardiography (Definitive Investigation)
- TTE (transthoracic echo): Identifies primum and secundum ASDs, measures defect size, shows right heart dilation. Doppler estimates Qp/Qs and pulmonary artery pressure
- TEE (transoesophageal echo): Required for sinus venosus ASDs (often missed on TTE) and for pre-procedural sizing before device closure. Also used intra-operatively during device deployment
- Bubble contrast echo (agitated saline): Detects right-to-left shunting (bubbles in LA/LV = positive); needed to detect PFO during Valsalva
- Findings: drop-out of interatrial septum signal, RV volume overload (RV dilation, paradoxical septal motion), LA-to-RA color Doppler jet
4. Cardiac MRI
- Excellent for sinus venosus defects, anomalous pulmonary venous anatomy, and pre-surgical planning
- Accurately quantifies Qp/Qs
5. Cardiac Catheterization
- Not routinely needed for diagnosis
- Indicated when: pulmonary hypertension suspected, conflicting echo results, pre-operative assessment of PVR
- Finding: step-up in oxygen saturation at the right atrial level (due to mixing of oxygenated left atrial blood)
- Qp/Qs calculated from oxygen saturations
6. Pulse Oximetry
- At rest and on exercise - to detect right-to-left shunting (desaturation) in patients with suspected Eisenmenger syndrome - Braunwald's, p. 878
MANAGEMENT
General Principles
- Closure is recommended when Qp/Qs ≥ 1.5:1 with RV volume overload, regardless of symptoms
- Optimal timing: before school age (4-5 years); adult repair still beneficial if done before irreversible PH develops
- Contraindication to closure: Eisenmenger syndrome (fixed severe pulmonary hypertension with resting right-to-left shunt)
-
60% of ASD interventions worldwide are now catheter-based - Sabiston, p. 2565
1. Catheter-Based (Percutaneous) Device Closure
Indications: Secundum ASD with adequate septal rim (≥5 mm on most sides) and defect diameter typically ≤38 mm
Procedure:
- Transfemoral venous access; catheter guided across the defect
- Amplatzer Septal Occluder (most widely used) - a self-centering, double-disc nitinol mesh device deployed under TEE + fluoroscopic guidance
- Device endothelialises within 3-6 months
Advantages: No thoracotomy, shorter hospital stay, faster recovery, excellent cosmesis
Post-procedure complications:
- Atrial arrhythmias
- Complete heart block (rare)
- Device thrombus (aspirin prescribed for 3-6 months)
- Device erosion (~1 in 1000 cases) - can cause haemopericardium; any chest pain post-procedure warrants urgent echo - Braunwald's, p. 878-879
A 2025 meta-analysis (de Liyis et al., PMID 38597284) comparing surgical vs. transcatheter closure in pediatric secundum ASD confirmed both are highly effective, with transcatheter offering fewer complications and shorter hospital stays.
2. Surgical Closure (Open Heart Surgery)
Indications for surgery over device closure:
- Primum ASD (always requires surgery; device not possible)
- Sinus venosus ASD (always requires surgery; cannot be catheter-closed)
- Coronary sinus defect
- Secundum ASD with inadequate rims for device anchorage
- Very large secundum defects
- Associated anomalies requiring surgical repair (AV valve repair, PAPVR repair)
- Failed or complicated device closure
Procedure:
- General anaesthesia; median sternotomy (or right mini-thoracotomy for minimally invasive approach)
- Cardiopulmonary bypass established (aortic + venous cannulation)
- Aortic cross-clamp + cardioplegia for myocardial protection
- Right atriotomy - direct visualisation of the defect
- Closure:
- Direct suture closure - for small defects (primary closure with continuous suture)
- Patch closure - autologous pericardium or synthetic patch (Dacron / Gore-Tex) for larger defects
- De-airing of the left atrium before closure
- Termination of bypass; closure
Sinus venosus ASD (superior type) with PAPVR to SVC:
- Intracardiac patch baffle redirecting anomalous pulmonary veins to LA
- Warden procedure: SVC is divided, the cardiac end oversewn, and the cephalic SVC end is anastomosed to the right atrial appendage; a patch baffles the anomalous veins to the LA
Inferior sinus venosus ASD (Scimitar syndrome):
- Complex repair; may require patch baffle within the intrahepatic IVC
- May need hypothermic circulatory arrest - Sabiston, p. 2396
A 2025 systematic review (El-Andari et al., PMID 40517112) confirmed that minimally invasive surgical approaches (right mini-thoracotomy, robotic) produce equivalent outcomes to sternotomy with better cosmesis and shorter recovery.
Outcomes: Perioperative mortality is very low (<1%). Post-operative survival equals that of the normal population when repair is performed before development of significant pulmonary hypertension. - Robbins, p. 505
Residual issues post-repair:
- Atrial arrhythmias may persist (especially AF) - surgery does not reliably reduce arrhythmia burden in older adults - Braunwald's, p. 878
- Follow-up TTE at 1 week, 1 month, then annually for at least 5 years (device closure)
- Patients with elevated PVR at closure need ongoing monitoring as PAH can progress
3. Medical Management
- No pharmacological therapy closes the defect
- Antiplatelet therapy (aspirin 75-150 mg/day) for 3-6 months post-device closure (prophylaxis against device thrombus)
- Rate/rhythm control + anticoagulation (warfarin or NOAC) for atrial fibrillation
- Diuretics + ACE inhibitors for right heart failure symptoms
- Pulmonary arterial hypertension (PAH) therapy (e.g., sildenafil, bosentan, prostacyclins) for Eisenmenger syndrome - treats symptoms but does not reverse the shunt
- Endocarditis prophylaxis: NOT routinely required for isolated secundum ASD (low risk); required for 6 months post-device/surgical repair
COMPLICATIONS OF UNTREATED ASD
| Complication | Mechanism |
|---|---|
| Right heart failure | Chronic RV volume overload |
| Atrial fibrillation / flutter | RA dilation causing electrical remodelling |
| Pulmonary arterial hypertension | Chronic high-flow pulmonary circulation |
| Eisenmenger syndrome | Reversal of shunt due to fixed PVR > SVR |
| Paradoxical embolism / stroke | Venous thrombus crossing atrial defect |
| Infective endocarditis | Rare in secundum ASD; more common with primum |
QUICK COMPARISON: ASD vs PFO
| Feature | ASD | PFO |
|---|---|---|
| Definition | True deficiency of septal tissue | Incomplete fusion of flap valve |
| Prevalence | 13/10,000 live births | ~25% of adults |
| Right heart dilation | Yes (if large) | No |
| Detectable on TTE | Usually | No (needs bubble echo + TEE) |
| Spontaneous closure | Rarely | Often remains patent |
| Clinical significance | Shunting, RV overload, arrhythmias | Paradoxical embolism risk |
| Treatment | Closure (device or surgery) | Device closure if cryptogenic stroke |
SUMMARY - KEY EXAM POINTS
| Feature | Answer |
|---|---|
| Incidence | 13 per 10,000 live births |
| Most common type | Secundum (90%) |
| Most common CHD in adults | ASD (due to lack of spontaneous closure) |
| Shunt direction | Left-to-right initially |
| Hallmark auscultatory sign | Wide, fixed splitting of S2 |
| ECG in secundum ASD | Incomplete RBBB (rSR' in V1), right axis deviation |
| ECG in primum ASD | Incomplete RBBB + left axis deviation |
| CXR findings | Pulmonary plethora, dilated PA, RA+RV enlargement |
| Definitive investigation | Echocardiography (TTE ± TEE) |
| Step-up in O2 saturation at catheter | At right atrial level |
| Qp/Qs for closure | ≥ 1.5:1 with RV overload |
| Preferred treatment (secundum) | Amplatzer device (catheter-based) |
| Types requiring surgery | Primum, sinus venosus, coronary sinus defects |
| Surgical approach | Cardiopulmonary bypass, right atriotomy, suture or patch |
| Contraindication to closure | Eisenmenger syndrome |
| Down syndrome association | Primum ASD (AVSD / endocardial cushion defect) |
| Prognosis after timely repair | Normal life expectancy |
Next ventricular septal defect tetralogy of Fallot, double outlet right ventricle. transposition of great vessels, AV canal defect.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Here is the complete MBBS Finals exam-level answer for all five conditions. Here's a quick orientation guide:
Quick Navigation
| Condition | Key Exam Points |
|---|---|
| VSD | Most common CHD; L→R shunt; pansystolic murmur at LLSB; patch closure via right atriotomy |
| TOF | Most common cyanotic CHD; 4 features from one malalignment; boot-shaped heart; tet spells; repair = VSD patch + RVOT relief |
| DORV | Both vessels from RV; physiology depends on VSD position; Taussig-Bing = TGA-like; repair strategy varies by anatomy |
| TGA | Aorta from RV; parallel circuits; cyanosis at birth; emergency PGE1 + Rashkind BAS; definitive = Arterial Switch Operation within 2-3 weeks |
| AVSD | ASD + VSD + AV valve defect; endocardial cushion failure; Down syndrome; left axis deviation on ECG; 2-patch repair protecting AV node |
The single most important distinguishing exam fact for each:
- VSD: loudest murmur in small defects (maladie de Roger)
- TOF: murmur from RVOT stenosis, NOT the VSD; squatting relieves tet spells
- DORV: Taussig-Bing (subpulmonic VSD) is physiologically TGA
- TGA: the only condition where cyanosis does NOT respond to oxygen; single loud S2; egg-on-a-string CXR
- AVSD: left/superior axis deviation on ECG + Down syndrome = pathognomonic combination
Focus more on surgery part and resend
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a surgery-heavy MBBS Finals answer for all five conditions. Key highlights of what was expanded vs. the previous answer:
What's New / Expanded in This Version
VSD:
- Full operative steps: right atriotomy vs. ventriculotomy vs. pulmonary arteriotomy by defect type
- Conduction anatomy with exact suture placement rules (anterosuperior safe, posteroinferior must go into RV muscle)
- Supracristal VSD: aortic cusp repair at same sitting
- Swiss-cheese VSD: PA banding, oversized patch, hybrid device closure
- Amplatzer device closure: indications and heart block risk
TOF:
- Historical context: Blalock-Taussig 1944; classic vs. modified BT shunt with diagrams
- Full transatrial-transpulmonary repair steps
- Transannular patch decision criteria (Z-score <-2.5; PA/Ao ratio <0.5; RV/LV ratio >0.7)
- Anomalous LAD crossing RVOT: use RV-PA conduit (Hancock/homograft)
- TOF with pulmonary atresia + MAPCAs: unifocalisation surgery
- Late PVR: transcatheter Melody/Sapien valve criteria (RVEDVi >160 mL/m²)
DORV:
- Full repair strategy by each VSD subtype
- Taussig-Bing without PS: ASO + VSD closure
- Taussig-Bing with PS: Rastelli, REV, or Yasui procedure
- Non-committed VSD: Rastelli-type tunnel + conduit; PA banding timing
- Conduit timing: delay until 2-3 years if extracardiac conduit needed (allows larger size)
TGA:
- Full step-by-step ASO: great vessel transection → coronary transfer (trapdoor technique, Yacoub A-E configurations) → Lecompte manoeuvre → anastomoses → pericardial patch reconstruction
- DHCA in neonates
- LV retraining protocol (PA band + BT shunt)
- TGA-VSD with severe PS: Rastelli, REV, Nikaidoh procedures
- Mustard/Senning: full explanation of physiologic vs. anatomic correction and why they failed (systemic RV)
AVSD:
- Rastelli A/B/C classification with surgical implications
- Full two-patch technique step-by-step: AV valve division → cleft closure → VSD patch (with conduction system protection) → AV valve-to-patch suturing → ASD patch
- Diagram of AV node position at posteroinferior junction
- Pulmonary hypertensive crisis management post-op
This is a shared conversation. Sign in to Orris to start your own chat.