Tubectomy procedures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of tubectomy (female sterilization) procedures, drawn from Berek & Novak's Gynecology and Pfenninger & Fowler's Procedures for Primary Care.
Tubectomy - Female Sterilization: Procedures
Tubectomy refers to any surgical procedure that permanently occludes the fallopian tubes to prevent fertilization. It is one of the most commonly performed elective surgical procedures worldwide.
Approaches / Routes of Access
Five main procedural routes are used:
| Route | Timing | Notes |
|---|---|---|
| Laparotomy at cesarean delivery | Intrapartum | Adds only minimal operative time |
| Postpartum minilaparotomy | Within 72 hours of vaginal delivery | 3-4 cm subumbilical incision; tubes lie in midabdomen |
| Interval minilaparotomy | ≥6 weeks postpartum | Popularized by Uchida; widely used in lower-resource settings |
| Laparoscopy | Interval (most common in USA) | 10-15 min; very small incision; requires insufflation |
| Hysteroscopy (transcervical) | Interval | Essure device; no incision needed |
Surgical Techniques for Tubal Occlusion
1. Pomeroy Technique (most common)
The classic and most widely performed method for both postpartum and interval ligation.
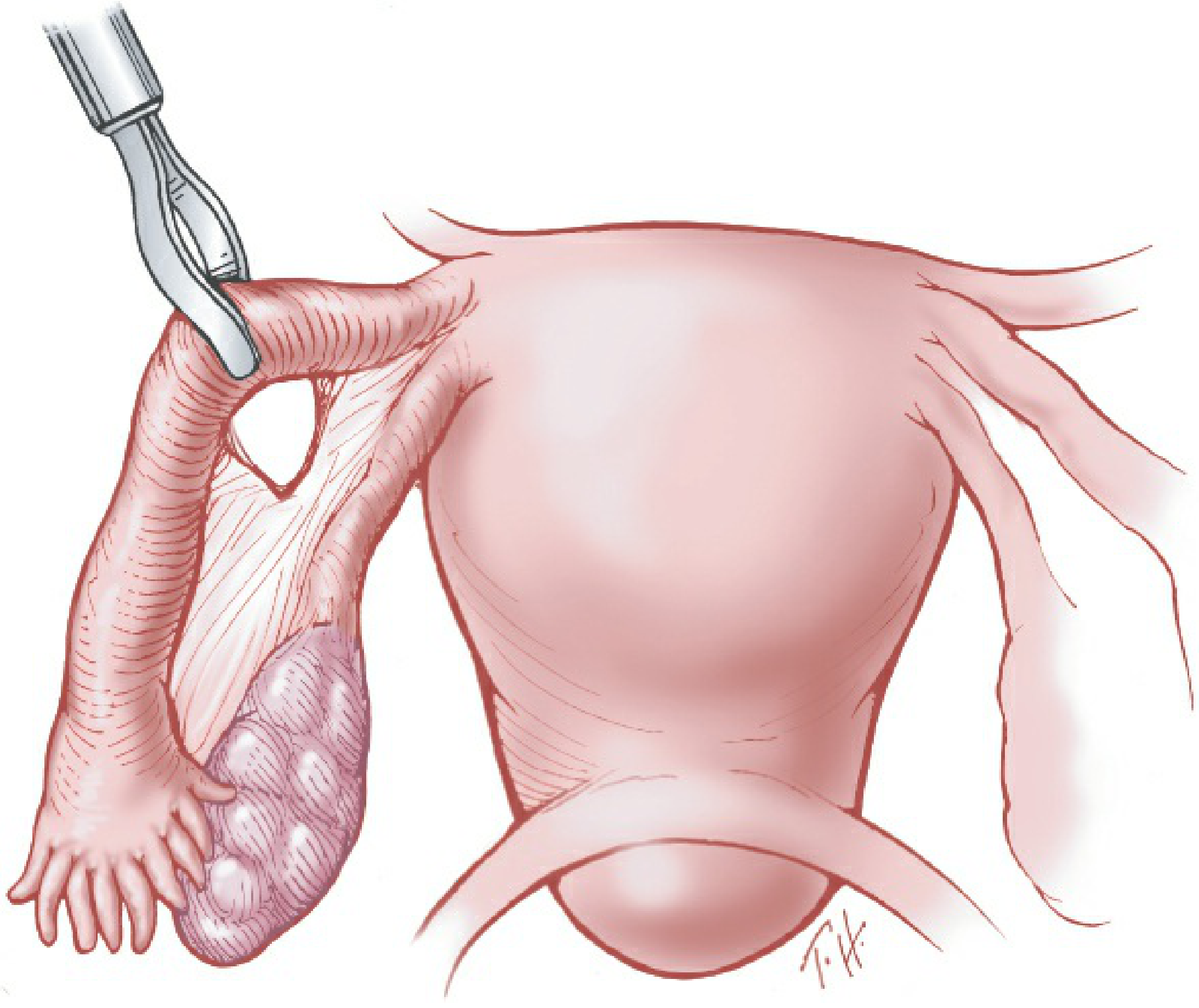
- A loop of the midportion (ampullary) tube is elevated
- The base of the loop is ligated with an absorbable catgut suture
- The ligated loop is excised
- As the suture absorbs, the ends retract apart and are sealed by scarring
- Destroys 3-6 cm of tube
- Failure rate: 1-4 per 1,000 procedures
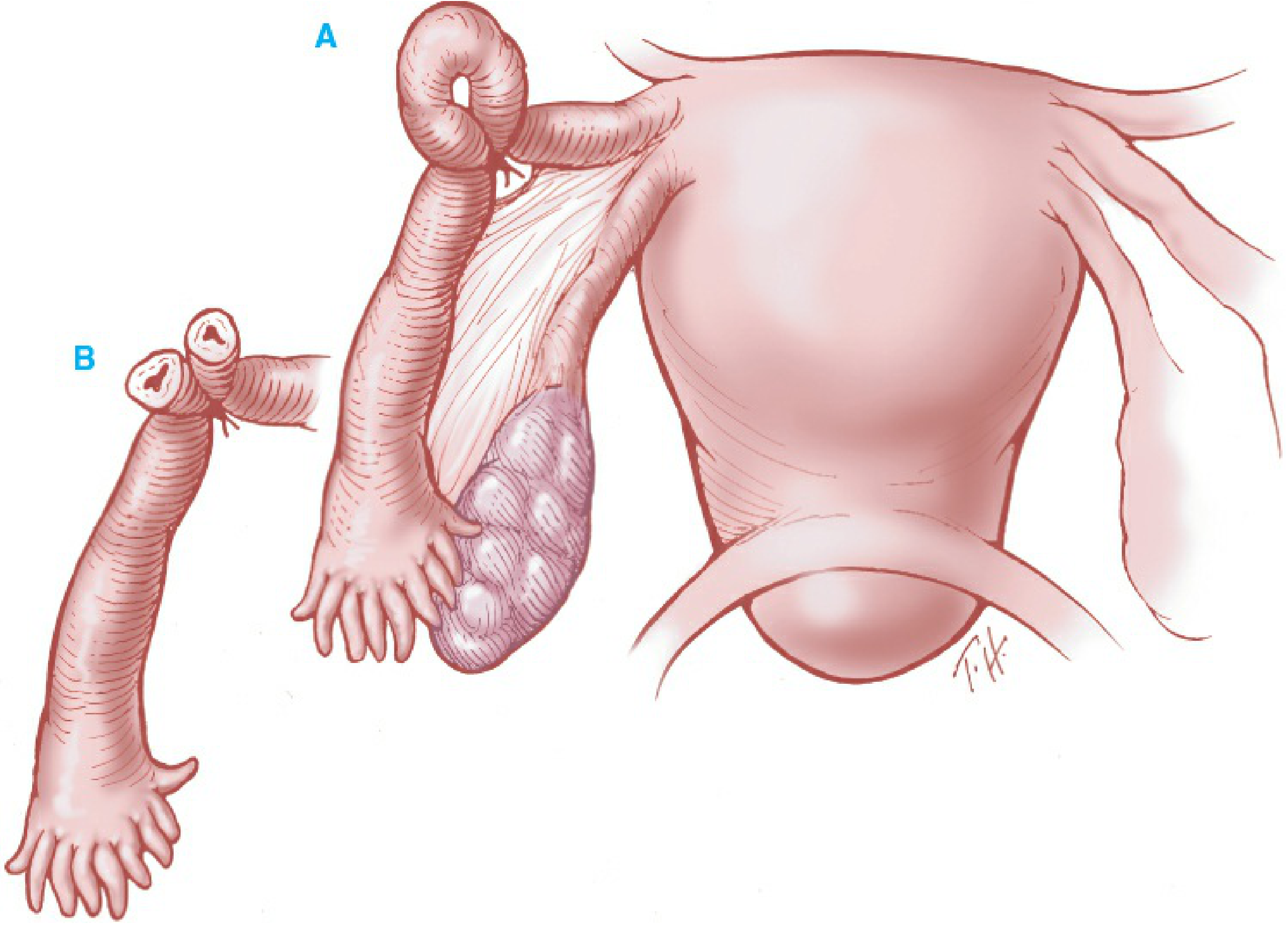
(Berek & Novak's Gynecology, Fig. 14-10: Pomeroy technique - A shows ligation of loop; B shows the separated cut ends)
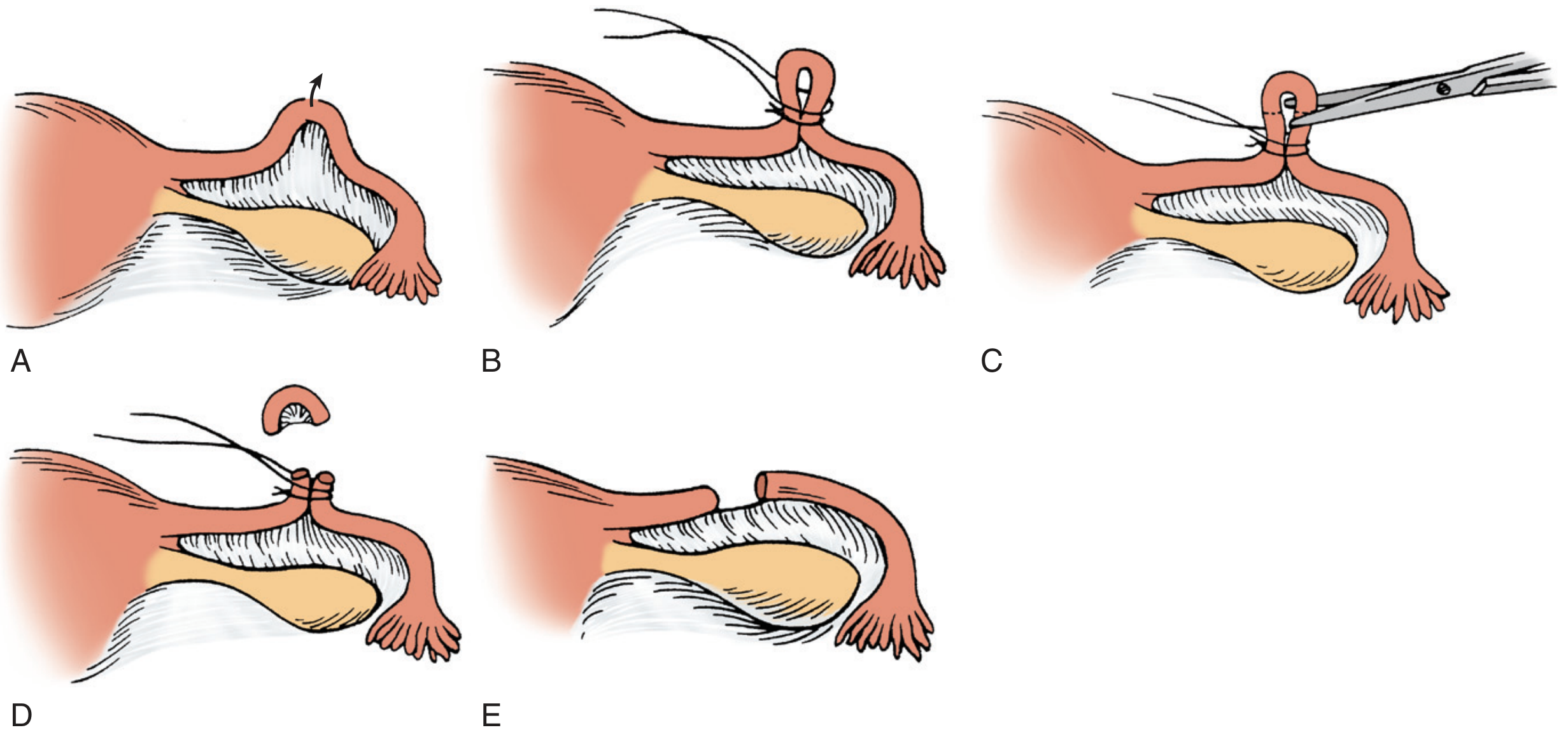
(Fig. 152-1: Modified Pomeroy technique - A: Lift loop, B: Double ligation with plain gut suture, C: Each limb cut separately, D: Loop removed, E: Later results)
2. Modified Pomeroy / Parkland Technique
- A small length of tube (about 2 cm) is separated from the mesosalpinx
- Ligated at each end with separate sutures
- The free segment between the ligatures is removed
- Also called: partial salpingectomy, Parkland Hospital technique, separate sutures technique
- Similar failure rate to classic Pomeroy
3. Irving Technique (very low failure rate)
- The midportion of the tube is excised
- The proximal stump is turned back and buried into a small stab wound in the uterine wall (creating a blind loop)
- The distal stump is buried in the mesosalpinx
- Pregnancy is exceedingly rare after this technique
- Not easily reversible
4. Uchida Technique (very low failure rate)
- Saline-epinephrine solution (1:1,000) is injected beneath the mucosa of the midportion, separating mucosa from underlying tube
- Mucosa is incised along the antimesenteric border
- A tubal segment is excised under traction so the proximal stump retracts beneath the mucosa
- The mucosa is then closed, burying and separating the proximal stump from the distal stump
- In Uchida's personal series of >20,000 cases: zero pregnancies
- Technically demanding; becoming more popular in the USA
5. Fimbriectomy
- Complete removal of the fimbriated end of the tube
- Higher pregnancy failure rate than other techniques
- Reversal is not feasible
6. Madlener Technique (abandoned)
- A loop of tube was crushed by cross-clamping, ligated with permanent suture, and excised
- Now abandoned due to high failure rates
Laparoscopic Occlusion Techniques
Laparoscopy is the most common method of interval sterilization in the USA. Tubal occlusion at laparoscopy is performed by one of four methods:
Bipolar Electrocoagulation
- The midisthmic portion of the tube is grasped with bipolar forceps
- Radiofrequency current is applied to three adjacent areas, coagulating 3 cm of tube
- Generator must deliver at least 25 W into 100-Ω resistance to ensure full-thickness coagulation
- If inadequate energy is used, intrauterine pregnancy can occur through an intact inner lumen
- After bipolar failure, ectopic pregnancy results in >50% of cases (tuboperitoneal fistula)
(Fig. 14-11: Bipolar electrocoagulation technique)
Falope Ring (Silastic Band)
- A small Silastic ring is stretched and placed over a loop of the midisthmic tube, then released
- Tube is blocked by ischemic compression (2-3 cm segment involved)
- If the tube cannot be easily pulled into the applicator, change to electrical coagulation to avoid tube laceration
- More post-procedure pain than clips; can be reduced with bupivacaine bathing
- Better reversibility than electrocautery, Irving, or Uchida techniques
Hulka Spring Clip
- Placed at right angles across the midisthmus
- Applicator must be perpendicular to tube with the tube completely contained before closing
- Can only be used on non-thickened tubes (not after prior salpingitis)
Filshie Clip (titanium + silicone rubber liner)
- Hinged titanium device with a silicone rubber liner
- Placed at right angles across the midisthmus
- The posterior jaw anvil should be visible through the mesosalpinx to confirm full-thickness tube capture
- Lower pregnancy rate than Hulka clip - has largely supplanted it
- First introduced in the USA in 1996; extensively used in UK and Canada

(Fig. 14-13: Filshie clip for tubal sterilization)
Vaginal Approaches (Less Common)
Colpotomy: Surgical incision in the posterior vaginal fornix through which the tube is delivered and occluded by ligation, clips, or rings.
Culdoscopy: A culdoscope is passed through a smaller colpotomy incision for tube identification and occlusion.
- Both share higher complication and failure rates than abdominal approaches
- Not suitable as postpartum methods
Transcervical Approaches
Essure (hysteroscopic): An inner stainless steel coil + outer superelastic coil (4 cm x 0.8 mm) inserted hysteroscopically into the fallopian tubes. FDA approved in 2002. (Note: Essure was voluntarily withdrawn from the US market by Bayer in 2018 due to safety concerns.)
Silastic plugs: Placed under hysteroscopic guidance; still considered experimental.
Salpingectomy for Sterilization
Complete or partial salpingectomy has been gaining favor as an alternative to tubal occlusion, as most epithelial ovarian cancers are now thought to arise from the distal fallopian tube. Key points:
- No increase in complication rates compared to occlusion methods
- Operative time increased by approximately 6-13 minutes
- Does not significantly affect ovarian reserve (AMH levels comparable)
- Recommended by ACOG when women undergo gynecologic surgery for other benign indications (opportunistic salpingectomy)
- Cost-effective: incremental cost-effectiveness ratio of ~$31,432 per QALY gained
Minilaparotomy vs. Laparoscopy - Comparison
| Feature | Minilaparotomy | Laparoscopy |
|---|---|---|
| Training required | Basic surgical skill | Specialized training |
| Instruments | Inexpensive | Expensive, requires maintenance |
| Duration | Longer | 10-15 minutes |
| Incision | 3-5 cm | Very small (umbilical) |
| Pain | More (abdominal incision) | Less |
| Postpartum use | Yes (preferred) | Not recommended |
| Complications if they occur | Usually minor | Can be serious (insufflation risks) |
Risks and Safety
- Overall complication rate: 1.7 per 100 procedures (CREST study, 9,475 cases)
- Risk factors for complications: general anesthesia, prior pelvic/abdominal surgery, PID history, obesity, diabetes
- Most common major complication: unintended laparotomy due to intra-abdominal adhesions
- Mortality: 1-2 per 100,000 sterilizations (national US data); nearly half from complications of general anesthesia
- International data: 4.7 deaths per 100,000 female sterilizations vs. 0.5 per 100,000 vasectomies
- When general anesthesia is used for laparoscopy, endotracheal intubation is mandatory (pneumoperitoneum increases aspiration risk)
- Prophylactic antibiotics are NOT indicated for laparoscopy or laparotomy sterilization (per ACOG/AHA guidelines)
Sterilization Failure
- Many apparent "failures" are pregnancies that began before surgery - a sensitive pregnancy test should be performed on the day of surgery
- Causes of true failure: misapplication of clip/ring, inadequate coagulation energy, anatomic abnormalities/adhesions
- 10-year cumulative failure rates (CREST study):
- Bipolar coagulation: 36.5 per 1,000 procedures (if <3 sites coagulated)
- Clip methods: lower when correctly applied
- Pomeroy/partial salpingectomy: 1-4 per 1,000
- Irving/Uchida: near zero
Noncontraceptive Benefits
- Reduced ovarian cancer risk: Tubal ligation associated with HR 0.76 (95% CI 0.64-0.90) for ovarian cancer (Nurses' Health Study, 29,340 women)
- Significant reduction in high-grade serous carcinomas (RR 0.77), endometrioid (RR 0.54), and clear cell tumors (RR 0.55)
- Complete salpingectomy is expected to offer even greater cancer risk reduction
Sources: Berek & Novak's Gynecology, pp. 762-769 | Pfenninger & Fowler's Procedures for Primary Care, 3rd ed., pp. 1063-1068
This is a shared conversation. Sign in to Orris to start your own chat.