
19281fef-a323-43c7-8d9d-c536a6401f27.jpeg
Physiology chages during pregnancy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I have all the key information needed for a comprehensive, well-structured answer. Here is the full response:
Physiological Changes During Pregnancy
(Source: Morgan and Mikhail's Clinical Anesthesiology, 7e)
Summary Table - Maximum Changes at Term
| Parameter | Change |
|---|---|
| Neurological - MAC | -40% |
| Oxygen consumption | +20 to 50% |
| Minute ventilation | +50% |
| Tidal volume | +40% |
| FRC | -20% |
| Airway resistance | -35% |
| PaCO2 | -15% |
| HCO3- | -15% |
| Blood volume | +35% |
| Plasma volume | +55% |
| Cardiac output | +40% |
| Stroke volume | +30% |
| Heart rate | +20% |
| Systolic BP | -5% |
| Diastolic BP | -15% |
| Peripheral resistance | -15% |
| Hemoglobin | -20% |
| Clotting factors | +30 to 250% |
| GFR | +50% |
1. Central Nervous System (Neurological) Changes
- MAC decreases by ~40% for all inhalational anesthetics at term; returns to normal by day 3 post-delivery.
- Progesterone rises to 20x normal at term and is at least partly responsible (it is sedating at pharmacological doses).
- β-endorphin surge during labor also reduces anesthetic requirements.
- Enhanced sensitivity to local anesthetics - epidural dose requirements reduced by up to 30%.
- Engorgement of epidural venous plexus (from inferior vena cava compression by the uterus) has three effects:
- Decreased spinal CSF volume
- Decreased potential epidural space volume
- Increased epidural pressure (becomes positive rather than negative)
- These enhance cephalad spread of local anesthetics during spinal/epidural anesthesia.
2. Respiratory Changes
- Oxygen consumption and minute ventilation increase progressively, up to 50% by term.
- Tidal volume increases (+40%), respiratory rate increases slightly (+15%).
- PaCO2 falls to 28-32 mmHg (physiological hyperventilation).
- Significant respiratory alkalosis is prevented by compensatory decrease in plasma bicarbonate.
- PaO2 increases slightly.
- 2,3-DPG rises to offset the Bohr effect - the P50 for hemoglobin shifts from 27 to 30 mmHg, enhancing O2 delivery to tissues.
- In the third trimester, the diaphragm is elevated but diaphragmatic motion is not restricted; the chest compensates with increased anteroposterior diameter.
- FRC decreases by up to 20% at term (returns to normal within 48 h post-delivery) - primarily due to reduced expiratory reserve volume.
- Vital capacity and closing capacity are minimally affected; airway resistance decreases.
- Physiological dead space decreases but intrapulmonary shunting increases.
- Critical clinical point: Decreased FRC + increased O2 consumption = rapid desaturation during apnea. Preoxygenation before GA induction is mandatory.
3. Cardiovascular Changes
- Blood volume increases 35%, plasma volume increases 55% - this "dilutional anemia" is physiological.
- Cardiac output increases 40% - primarily from increased stroke volume early, then heart rate later.
- Heart rate increases 20%, stroke volume increases 30%.
- Systemic and pulmonary vascular resistance both fall; BP decreases slightly despite higher cardiac output.
- During labor, cardiac output increases a further 10-25% with each contraction.
- Immediately post-delivery, cardiac output transiently rises even further due to:
- Relief of aortocaval compression
- Autotransfusion from the uterus
- Aortocaval compression: The enlarged uterus in the supine position compresses the inferior vena cava, reducing venous return and cardiac output (supine hypotension syndrome). Left uterine displacement corrects this.
4. Uteroplacental Circulation
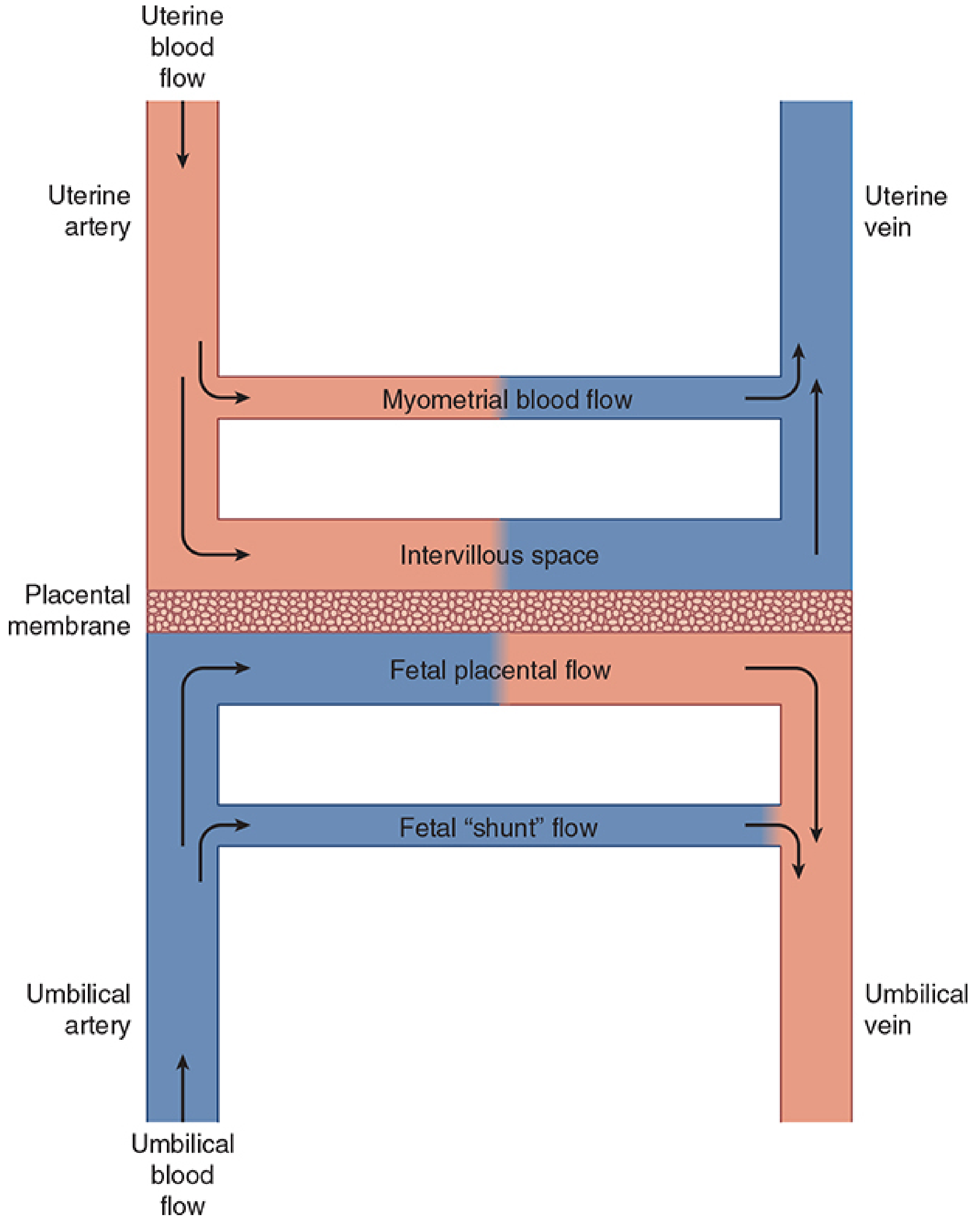
Uteroplacental circulation - Morgan and Mikhail's Clinical Anesthesiology, 7e
- At term, uterine blood flow = ~10% of cardiac output = 600-700 mL/min (vs. 50 mL/min non-pregnant).
- 80% goes to the placenta; 20% to the myometrium.
- Uterine vasculature is maximally dilated - no autoregulation but remains sensitive to α-adrenergic agonists.
- Three major factors reduce uterine blood flow:
- Systemic hypotension (aortocaval compression, hypovolemia, sympathetic blockade)
- Uterine vasoconstriction (catecholamines, α-agonists like phenylephrine)
- Uterine contractions (elevated venous pressure + arterial compression)
5. Hematological Changes
- Plasma volume increases more than RBC mass → physiological dilutional anemia (Hb decreases ~20%).
- Platelets decrease by ~10%.
- Clotting factors increase dramatically (30-250%) - pregnancy is a hypercoagulable state.
- Factors I (fibrinogen), VII, VIII, IX, X, XII all rise.
- This protects against hemorrhage at delivery but increases DVT/PE risk.
- WBC increases (neutrophilia).
6. Renal Changes
- GFR increases 50% due to increased cardiac output and reduced renal vascular resistance.
- Serum creatinine and urea fall (normal pregnancy values are lower than non-pregnant norms).
- Glycosuria can occur due to tubular maximum being exceeded (not necessarily pathological).
- Uterine compression of the ureters may cause physiological hydronephrosis (right > left).
7. Gastrointestinal Changes
- Gastric emptying is delayed; lower esophageal sphincter tone decreases (progesterone effect).
- Increased risk of aspiration - all pregnant patients at term are considered to have a full stomach for anesthetic purposes.
- Intragastric pressure is elevated by the gravid uterus.
8. Key Hormonal/Metabolic Drivers
| Hormone | Effect |
|---|---|
| Progesterone | Sedation, reduced MAC, LES relaxation, smooth muscle relaxation |
| Estrogen | Fluid retention, mucous membrane engorgement (difficult airway) |
| hCG | Nausea/vomiting (peak at 8-12 weeks) |
| hPL | Insulin resistance, lipid mobilization |
Clinical Takeaways:
-
The airway is often edematous/friable - smaller ETT may be needed; Mallampati class worsens with labor.
-
Delayed gastric emptying + reduced LES tone = aspiration risk; RSI + cricoid pressure is standard.
-
Supine position → aortocaval compression → always use left lateral tilt.
-
Rapid desaturation on induction - always pre-oxygenate thoroughly.
-
Morgan and Mikhail's Clinical Anesthesiology, 7e, Chapter 40 - pp. 1572-1581
Detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here is the fully detailed, system-by-system breakdown of physiological changes during pregnancy:
Physiological Changes During Pregnancy - Detailed Notes
1. GENITAL ORGANS
Uterus
- Non-pregnant uterus weighs ~60-70 g and has a capacity of ~10 mL.
- At term, it weighs ~1000 g with a capacity of ~5000 mL (500-fold increase in volume).
- Growth occurs by hypertrophy of existing myometrial cells (stimulated by estrogen and mechanical stretch) - NOT hyperplasia.
- Uterine blood flow at term = 600-700 mL/min (10% of cardiac output), vs. 50 mL/min when non-pregnant.
- 80% of uterine blood goes to the placenta; 20% to the myometrium.
- The uterine vasculature is maximally dilated - autoregulation is absent.
- Uterine vascular bed remains sensitive to α-adrenergic agonists (catecholamines, phenylephrine can cause vasoconstriction and fetal compromise).
- Three factors reduce uterine blood flow:
- Systemic hypotension (aortocaval compression, hypovolemia, regional anaesthesia)
- Uterine vasoconstriction (stress-induced catecholamine release)
- Uterine contractions (elevate venous pressure + compress arterial vessels)
- Softening of the cervix (Goodell's sign) - due to increased vascularity and edema; facilitated by relaxin.
- Hegar's sign - softening of the lower uterine segment (6-8 weeks).
- Osiander's sign - pulsation felt in lateral fornix due to increased uterine artery blood flow.
Vagina
- Increased vascularity and venous stasis → Chadwick's/Jacquemier's sign: mucosa changes from pink → violet → blue (from 4th month onward).
- Vaginal secretions increase (white, non-offensive leukorrhea of pregnancy).
- Vaginal pH decreases (more acidic) due to increased lactic acid from glycogen breakdown - protective against infection.
2. BREASTS
Changes proceed in a hormonal cascade across all three trimesters:
First Trimester
- Estrogen (from corpus luteum, then placenta): ductal proliferation and elongation, involution of adipose tissue.
- Progesterone: stimulates lobule development.
- hCG peaks at 9 weeks - prevents corpus luteum involution, maintains estrogen + progesterone.
- Mononuclear inflammatory cell infiltration of breast tissue begins.
- Breast enlargement and tenderness (one of the earliest signs of pregnancy).
Second Trimester (by 20 weeks)
- Mammary glands sufficiently developed to produce milk components (prolactin-stimulated).
- Secretory substances accumulate in lobule acini epithelial cells.
- Myoepithelial cells become flattened; epithelial cells enlarge.
- Areola darkens; areolar glands (Montgomery's tubercles) become more prominent.
Third Trimester
- Increased prolactin promotes alveolar cell differentiation and initiates lactogenesis stage I.
- Colostrum is produced: thin yellowish fluid containing free fat globules and large phagocytic cells - present from ~16 weeks.
- Actual milk production is inhibited by high estrogen + progesterone (these fall rapidly post-delivery to allow let-down).
- Striae (silver lines/linea albicantes) appear on breasts after 6th month.
- Surface veins become prominent - visible as blue lines.
Post-delivery
- After parturition, estrogen and progesterone fall → prolactin uninhibited → milk production begins.
- Colostrum is replaced by milk ~10 days post-delivery.
- Post-lactation: massive apoptosis, acinar involution, connective tissue remodelling (loose → dense structure), basement membrane thickening.
3. CUTANEOUS CHANGES
| Sign | Description | Cause |
|---|---|---|
| Linea nigra | Dark line from pubis to above umbilicus | Increased MSH (melanocyte-stimulating hormone) |
| Chloasma/melasma gravidarum | Mask of pregnancy - hyperpigmentation of face | Estrogen + MSH effect |
| Striae gravidarum | Stretch marks on abdomen, breasts, thighs | Skin stretching + glucocorticoid effect on dermal collagen |
| Palmar erythema | Redness of the palms | Elevated estrogen levels |
| Spider angiomas/telangiectasiae | Vascular spiders on skin | Elevated estrogen |
| Vulval hyperpigmentation | Darkening of external genitalia | Elevated MSH + estrogen |
| Increased sweating | Hyperhidrosis | Increased basal metabolic rate |
| Nail changes | Soft, brittle nails with transverse grooves | Metabolic changes |
4. WEIGHT GAIN
Recommended total weight gain at term: 11-16 kg (average ~12.5 kg for normal BMI).
Composition:
| Component | Weight |
|---|---|
| Fetus | ~3.3 kg |
| Placenta | ~0.6 kg |
| Amniotic fluid | ~0.8 kg |
| Uterus (hypertrophy) | ~0.9 kg |
| Breast tissue | ~0.4 kg |
| Blood volume increase | ~1.2 kg |
| Extracellular/extravascular fluid | ~1.2 kg |
| Maternal fat stores | ~3.5 kg |
5. BODY WATER METABOLISM
- Total body water increases by 6-8 litres at term.
- Of this, approximately 3.5 L is in the fetus, placenta, and amniotic fluid; the rest is in the mother.
- Plasma volume increases by 55% (most disproportionate change - produces dilutional anemia).
- Red blood cell mass increases by 45%.
- Plasma osmolality decreases by 8-10 mOsm/kg (the osmotic threshold for ADH secretion and thirst is reset downward).
- Dependent edema of the ankles is physiological (occurs in up to 80% of pregnancies due to increased venous pressure from IVC compression).
6. HEMATOLOGICAL CHANGES
Erythrocytes
- RBC mass increases by ~45% (less than plasma volume increase of 55%) → physiological dilutional anaemia.
- Hemoglobin at term usually remains >11 g/dL.
- Physiological anaemia of pregnancy - not true iron deficiency; Hb falls to ~11-12 g/dL.
- Iron supplementation is required because fetal demands + increased RBC production exceed normal dietary intake.
- Folate deficiency anaemia can develop if supplements are not taken (fetal utilization of folate).
White Blood Cells
- Leukocytosis up to 21,000/μL during third trimester (predominantly neutrophilia).
- Further leukocytosis during labor (up to 25,000-30,000/μL).
Platelets
- Platelet count decreases by ~10% (gestational thrombocytopenia); usually >100,000/μL and clinically insignificant.
Coagulation - Hypercoagulable State
Pregnancy is a prothrombotic state (evolutionary adaptation to limit hemorrhage at delivery):
| Factor | Change |
|---|---|
| Fibrinogen (Factor I) | Increases 50-100% (from ~300 → 450-600 mg/dL) |
| Factor VII | Increases |
| Factor VIII | Increases |
| Factor IX | Increases |
| Factor X | Increases |
| Factor XII (Hageman) | Increases |
| Factor XI | May decrease |
| Protein S | Decreases (anticoagulant) |
| Protein C | Unchanged |
| Antithrombin III | Slightly decreased |
| Fibrinolysis | Accelerated late in third trimester |
Net result: 5-6x increased risk of venous thromboembolism (DVT/PE) during pregnancy and puerperium.
7. CARDIOVASCULAR CHANGES
Cardiac Output
- Increases 40% by term = largest single physiological change in the cardiovascular system.
- Mechanism: Stroke volume ↑30% + Heart rate ↑20%.
- Timeline:
- Cardiac output rises early in the 1st trimester (by 8 weeks - mostly stroke volume driven).
- Peaks in the 2nd trimester.
- 3rd trimester: Relatively stable; does not appreciably rise further until labor.
- During labor: Each contraction adds 10-25% more output (autotransfusion of 300-500 mL from the contracting uterus).
- Immediately post-delivery: Cardiac output rises further (relief of IVC compression + uterine autotransfusion).
- Returns to normal 2 weeks after delivery.
Blood Pressure
- Systolic BP: decreases slightly (~5%).
- Diastolic BP: decreases more (~15%) - nadir in mid-2nd trimester.
- Fall in BP despite increased cardiac output is entirely due to peripheral vasodilatation (progesterone-mediated smooth muscle relaxation, local prostaglandins, nitric oxide).
- Returns toward baseline in 3rd trimester.
Vascular Resistance
- Peripheral vascular resistance: decreases 15%.
- Pulmonary vascular resistance: decreases 30% - pulmonary hypertension does not develop despite higher blood flow.
Blood Volume
- Total blood volume increases 35% (1000-1500 mL by term).
- Total blood volume at term = 90 mL/kg.
- Expected blood loss at delivery: 200-500 mL (vaginal), 800-1000 mL (cesarean).
- Blood volume normalizes 1-2 weeks post-delivery.
Structural Cardiac Changes
- Cardiac chambers enlarge; myocardial hypertrophy on echocardiography.
- Heart is displaced upward and leftward by the elevated diaphragm → chest X-ray shows apparent cardiomegaly + left axis deviation on ECG.
- T-wave changes and ST depression can occur normally.
- Physical exam:
- Grade I-II systolic ejection (flow) murmur (due to increased blood flow - normal)
- Exaggerated splitting of S1
- S3 may be audible (normal in pregnancy)
- Small asymptomatic pericardial effusion may occur
- Central venous pressure, pulmonary artery pressure, and PAOP (wedge pressure) remain unchanged despite expanded volume (due to reduced resistance).
Aortocaval Compression
- After week 20, the gravid uterus compresses the inferior vena cava when supine → reduces venous return → decreases cardiac output by up to 30%.
- 5% of women at term: Supine hypotension syndrome - hypotension + pallor + nausea/vomiting.
- The aorta is also compressed → reduces blood flow to lower limbs and uteroplacental circulation.
- Correction: left lateral tilt >15° (wedge under right hip).
- Chronic partial IVC obstruction in 3rd trimester: venous stasis, edema, DVT risk in lower limbs; distension of epidural veins.
8. RESPIRATORY CHANGES
Volumes and Capacities
| Parameter | Change | Notes |
|---|---|---|
| Tidal Volume (TV) | +40% | Most significant change |
| Respiratory Rate | +15% | Mild increase |
| Minute Ventilation | +50% | TV × RR |
| Inspiratory Reserve Volume | Slight increase | |
| Functional Residual Capacity (FRC) | -20% | Returns to normal in 48h post-delivery |
| Expiratory Reserve Volume | Decreases | Primary cause of FRC reduction |
| Vital Capacity | Minimally affected | |
| Closing Capacity | Minimally affected | |
| Physiological Dead Space | Decreases | Narrows arterial-end tidal CO2 gradient |
| Airway Resistance | -35% | Progesterone-mediated bronchial smooth muscle relaxation |
Blood Gases
| Parameter | Change |
|---|---|
| PaO2 | Slightly increased (+10%) |
| PaCO2 | Decreases to 28-32 mmHg (-15%) |
| HCO3- | Decreases to ~18-22 mEq/L (-15%) - compensatory |
| pH | Slightly alkalotic (7.40-7.45) |
| P50 (hemoglobin) | Increases from 27 → 30 mmHg (rightward shift) |
Mechanisms
- Hyperventilation is driven primarily by progesterone (direct stimulatory effect on the respiratory centre).
- Elevated 2,3-DPG offsets hyperventilation's effect on O2-Hb affinity (keeps rightward shift intact).
- Compensatory metabolic acidosis (HCO3- falls) prevents frank respiratory alkalosis.
Diaphragm/Chest Wall
- Diaphragm is elevated by ~4 cm in 3rd trimester.
- Compensatory increase in anteroposterior chest diameter.
- Diaphragmatic motion is NOT restricted.
- CXR shows elevated diaphragm + prominent vascular markings.
Clinical Hazards
- Rapid desaturation during apnea - decreased FRC + increased O2 consumption → preoxygenation mandatory before GA induction.
- Atelectasis in supine position - closing volume can exceed FRC at term → atelectasis and hypoxemia.
- Respiratory mucosa engorgement - upper airway edema and friability → trauma with laryngoscopy; use smaller ETT (6-6.5 mm); Mallampati score worsens.
- Faster inhalational anesthetic uptake (decreased FRC + increased minute ventilation).
9. RENAL CHANGES
- Renal plasma flow increases by 75% early in pregnancy.
- GFR increases 50% by 16 weeks (due to increased cardiac output + reduced renal vascular resistance).
- Serum creatinine falls to as low as 0.5 mg/dL (normal non-pregnant ~0.9 mg/dL).
- BUN may decrease to 9 mg/dL.
- Glycosuria (1-10 g/day): tubular reabsorption maximum is exceeded even at normal blood glucose - NOT necessarily pathological.
- Mild proteinuria (<300 mg/24h) - normal; >300 mg/24h = pre-eclampsia threshold.
- Plasma osmolality decreases by 8-10 mOsm/kg (osmostat is reset).
- Physiological hydronephrosis: ureteric compression by the gravid uterus (right > left due to dextrorotation) + progesterone-induced smooth muscle relaxation → stasis → increased UTI risk.
- Urinary frequency: in early pregnancy (uterine pressure on bladder) and near term.
10. GASTROINTESTINAL CHANGES
- Gastric emptying delayed (progesterone inhibits smooth muscle).
- Lower esophageal sphincter (LES) tone reduced (progesterone) → gastroesophageal reflux and esophagitis are common.
- Stomach displaced upward and anteriorly by the uterus → promotes sphincter incompetence.
- Gastric acid and volume: Do NOT significantly change in normal pregnancy.
- Aspiration risk: All pregnant patients at term treated as "full stomach" - RSI + cricoid pressure required.
- Pseudocholinesterase (plasma cholinesterase) decreases 25-30% at term (dilutional + reduced hepatic synthesis) → rarely clinically significant prolongation of succinylcholine effect; normalizes 6 weeks post-partum.
- Liver: Hepatic function and blood flow are unchanged. Minor elevations of transaminases and LDH in 3rd trimester. Alkaline phosphatase rises (placental isoenzyme). Serum albumin decreases (dilutional) → reduced colloid oncotic pressure.
- Gallbladder: Progesterone inhibits cholecystokinin → incomplete gallbladder emptying → bile stasis → increased cholesterol gallstone risk.
- Nausea and vomiting (morning sickness): peaks at 8-12 weeks; correlates with hCG peak.
11. METABOLIC CHANGES
Carbohydrate Metabolism - "Accelerated Starvation / Facilitated Anabolism"
- Pregnancy is diabetogenic despite fasting hypoglycemia - an apparent paradox.
- Fasting state: Blood glucose ↓, amino acids ↓, insulin ↓ → exaggerated fasting hypoglycemia.
- Fed state: Hyperinsulinemia + insulin resistance → glucose and amino acids are preferentially shunted to the fetus.
- Insulin resistance caused by:
- Human chorionic somatomammotropin (hCS/hPL) - most important
- Human placental growth hormone (hPGH)
- Elevated cortisol
- Elevated estrogen + progesterone
- Pancreatic β-cell hyperplasia occurs to compensate for insulin resistance → insulin levels progressively rise.
- Rapid return to normal glucose metabolism after delivery = evidence that fetoplacental hormones are the diabetogenic drivers.
Metabolic Fuel Values (Late Pregnancy vs Non-Pregnant Fasting)
| Compound | Non-Gravid | Late Pregnancy |
|---|---|---|
| Glucose | 79 mg/dL | 68 mg/dL (↓) |
| Insulin | 9.8 μU/mL | 16.2 μU/mL (↑) |
| Amino acids | 3.82 μmol/L | 3.18 μmol/L (↓) |
| Free fatty acids | 76 mg/dL | 181 mg/dL (↑) |
| Cholesterol | 163 mg/dL | 205 mg/dL (↑) |
Fat Metabolism
- Total plasma lipids increase significantly from 24 weeks onward.
- Triglycerides, cholesterol, and free fatty acids all increase markedly.
- HDL cholesterol increases early; LDL cholesterol increases later.
- Free fatty acids and ketones elevated (fuel for mother) to spare glucose for fetus.
Protein Metabolism
- Plasma amino acid levels fall (fetal utilization).
- Prolonged fasting → exaggerated hyperketonemia and hypoglycemia.
- Gluconeogenesis is NOT adequately increased to compensate for glucose loss to the fetus.
Thyroid
- hCG and elevated estrogens promote thyroid gland hypertrophy.
- Thyroid-binding globulin (TBG) increases → total T4 and T3 increase.
- Free T4, free T3, and TSH remain normal (euthyroid state).
- Clinically: goiter may develop; do not treat total T4 elevation as hyperthyroidism.
Calcium
- Total serum calcium decreases (dilutional, lower albumin).
- Ionized calcium remains normal (physiologically active form - no clinical consequence).
12. MUSCULOSKELETAL CHANGES
- Relaxin (secreted by corpus luteum, decidua, and placenta):
- Softens and ripens the cervix.
- Relaxes pubic symphysis and sacroiliac joints.
- Inhibits uterine contractions.
- Increases ligamentous laxity throughout the spine.
- Lumbar lordosis increases to shift the center of gravity.
- Diastasis recti - separation of rectus abdominis muscles.
- Carpal tunnel syndrome - fluid retention compresses the median nerve at the wrist (common in 3rd trimester).
- Back pain is very common (ligamentous laxity + postural changes).
13. CENTRAL NERVOUS SYSTEM CHANGES
- MAC (Minimum Alveolar Concentration) for all inhalational anesthetics decreases progressively:
- By term: decreases 40%.
- Returns to normal by day 3 post-delivery.
- Mechanism: progesterone (sedating in pharmacological doses, rises 20x normal at term) + β-endorphin surge during labor.
- Sensitivity to local anesthetics increases:
- Epidural dose requirements: reduced by up to 30%.
- MLAC (minimum local analgesic concentration) concept.
- Mechanisms: hormonal sensitization + physical epidural space changes.
- Epidural space changes (from IVC compression → epidural vein engorgement):
- Decreased CSF volume in the spinal canal.
- Decreased potential epidural space volume.
- Epidural pressure becomes positive (normally negative).
- Enhanced cephalad spread of epidural/spinal blocks.
- Increased risk of inadvertent intravascular injection of epidural catheter.
Key Hormonal Drivers Summary
| Hormone | Source | Key Physiological Effect |
|---|---|---|
| Progesterone | Corpus luteum → placenta | Smooth muscle relaxation (uterus, GI, vessels, bronchi), sedation, ↑ ventilation, ↓ LES tone |
| Estrogen | Corpus luteum → placenta | Ductal growth, fluid retention, skin changes, ↑ TBG, ↑ coagulation factors |
| hCG | Trophoblasts | Maintains corpus luteum; nausea/vomiting (hCG peak = morning sickness peak at 9 weeks) |
| hCS/hPL | Placenta | Insulin resistance, lipolysis, ensures fetal glucose supply |
| Placental GH | Placenta | Insulin resistance |
| Relaxin | Corpus luteum, decidua | Joint laxity, cervical softening, inhibits contractions |
| Prolactin | Anterior pituitary | Breast lobular development, lactogenesis (inhibited by E2 + P4 during pregnancy) |
| MSH | Anterior pituitary | Skin pigmentation (linea nigra, chloasma) |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Chapter 40 (pp. 1572-1581)
- Creasy & Resnik's Maternal-Fetal Medicine - Chapter 10 (Endocrine-Metabolic Changes)
- Current Surgical Therapy, 14e - Pregnancy Changes to the Breast
- Parikh's Textbook of Medical Jurisprudence - Presumptive Signs of Pregnancy
This is a shared conversation. Sign in to Orris to start your own chat.